Survivorship - Food for thought: Systematic review of Cancer Survivors Perceptions of Food Related Information
Canham, R1,2, Shaw, R.L2*
1 Senior Consultant, Greenstreet Berman Ltd, London, UK.
2 School of Life and Health Sciences, Aston University Birmingham B4 7ET, UK.
*Corresponding Author
Dr. Rachel Shaw
School of Life and Health Sciences,
Aston University Birmingham, B4 7ET, UK.
E-mail: r.l.shaw@aston.ac.uk
Received: March 31, 2016; Accepted: April 22, 2016; Published: May 11, 2016
Citation: Rebecca C, Shaw RL (2016) Survivorship - Food for thought: Systematic Review of Cancer Survivors Perceptions of Food Related Information. Int J Food Sci Nutr Diet. S3:004,23-34. doi: dx.doi.org/10.19070/2326-3350-SI03004
Copyright: Shaw RL© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
During 2011, 331,487 new cases of cancer were diagnosed within the UK. Within the same year, cancer survival rates were reported to be approximately 50%, with those diagnosed said to live, on average, 10 more years following diagnosis. Cancer patients are considered ‘at risk’ of food borne illness, in particular, from Listeria Monocytogenes. Whilst common, Listeria can prove fatal to cancer patients who may be immune suppressed. Appropriate food safety and nutritional advice is therefore important to ensuring the health and continued recovery of cancer sufferers during the stages of diagnosis and treatment, but also through to survival and transition back into ‘normal’ life.
This Mixed Studies Review (MSR) therefore sought to better understand Cancer survivors’ perceptions of food related information, with a view to enhancing the effectiveness of such information in future. The findings revealed a preference for receiving more information as opposed to less, with survivors primarily seeking relevant and prescriptive guidance via practitioners and paper based channels. Food related information was also valued when provided as part of broader lifestyle advice.
Theoretical implications are discussed and recommendations for theory and practice are presented, however, the few studies identified by this review provide little evidence on which to base definitive decisions for future practice, in particular with regards to food safety messages. Further research in this area is therefore required.
2.Introduction & Rationale
2.1.Cancer survivorship within the UK
2.2.Vulnerability to food borne illness
3.Review Aims
4.Method
4.1.Systematic search
4.2.Screening
4.3.Critical appraisal of material
4.4.Synthesis
5.Results
5.1.Included studies
5.2.Appraisal
5.3.Synthesis of results
6.Findings & Implications For Practice
6.1.Constructs identified
6.2.Advice
6.3.Contents of information
6.4.Delivery of information
6.5.Change
6.6.Beliefs
7.Discussion
7.1.Summary of key findings
7.2.Strengths and limitations
7.3.Recommendations
8.Conclusion
9.References
Keywords
Food Safety; Nutrition; Information Dissemination; Education; Consumer Health Information; Cancer Survivors.
Introduction & Rationale
According to Cancer Research UK [1], there were 331,487 new cases of cancer diagnosed in the UK during 2011. Within the same timeframe, CRUK also reported a survival rate of approximately 50%, with those diagnosed living a further 10 more years. Two of the most common types are cancer of the breast and bowel, with 50,285 and 41,581 cases recorded respectively within 2011 [2]. Of these cases, survival rates are strong and continue to rise, with an estimated two in three women diagnosed with breast cancer surviving in excess of 20 years and approximately 6-10 bowel cancer diagnoses surviving in excess of 10 years.
These figures demonstrate the need to focus intervention and support beyond the stages of diagnosis and treatment, but through to survival and transition back into ‘normal’ life. For many survivors, the advice and support provided to help manage the physical, psychological and emotional experiences following treatment is variable. Knowing how to find useful and reliable information can help increase confidence, quality of life and long term recovery [3].
Cancer patients have been identified as a vulnerable group, considered ‘at risk’ of Listeria Monocytogenes, a common and severe food borne pathogen [4, 5]. Once contracted Listeria Monocytogenes can prove fatal to cancer patients who may be resistant to antibiotics, as tumour cells genetically resist cytostatic drugs [6].
Qualitative research with cancer patients has previously revealed discrepancies between risk awareness, susceptibility and mitigating behaviours. Despite acknowledging their enhanced vulnerability to food borne illness, patients did not link this vulnerability to food handling or consumption behaviours, with many reporting consumption of foods considered to be of high risk of lysteriosis, such as eggs with runny yolks or cured meats [7]. In some instances, patients lacked awareness of food considered to be ‘high risk’ when immune compromised [8].
In a review of consumer food safety practices commissioned by the Food Standards Agency [4] the following recommendations were proposed to manage the increased risk of Listeria Monocytogenes amongst cancer patients:
- Development of targeted dietary advice, if possible in collaboration with the professionals that care for cancer patients, such as oncologists, dieticians, oncology centres and chemotherapy units;
- Advice be communicated to patients by those healthcare professionals; and
- Work should involve specialist organisations, such as the Oncology Section of the Royal Society of Medicine and the NHS Cancer Programme.
Review Aims
The objective of this Mixed Studies Review (MSR) was to better understand Cancer survivors’ perceptions of food related information, with a view to enhancing the effectiveness of such information in future. The study method comprised four key stages: a) Systematic search; b) critical appraisal of studies; c) Constant comparison of the data; and d) Interpretative thematic analysis. The following research questions were proposed to guide the review:
- How do Cancer survivors perceive the food related information they receive? In particular:
- the delivery mechanism/channel used to communicate the information;
- relevance of content; and
- understanding of the message.
- Which sources of food related information are used and trusted amongst cancer survivors?
- What content is covered within the food related information provided to cancer survivors?
- Does the information cover both dietary advice and food safety recommendations?
- What theoretical models and interventions have been applied to improve nutritional intake and safe food handling practices amongst cancer survivors?
It was beyond the scope of this research to evaluate the success of the various methods/interventions with regards to their impact on health behaviours and outcome measures taken.
Method
The present MSR incorporated qualitative, quantitative and mixed methods studies.
The SPIDER (Sample, Phenomenon of Interest, Design, Evaluation and Research type, as illustrated in Figure 1, adapted from [9]) tool enabled selection and refinement of search terms.
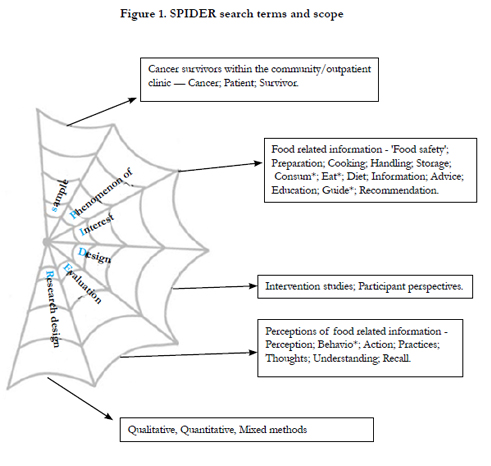
Figure 1. SPIDER search terms and scope
A systematic search was conducted within Web of Knowledge, Scopus, PubMed and the Cochrane database of systematic reviews. The search terms outlined in Table 1 were combined using Boolean logic (‘and’ and ‘or’) and wildcards within each database.
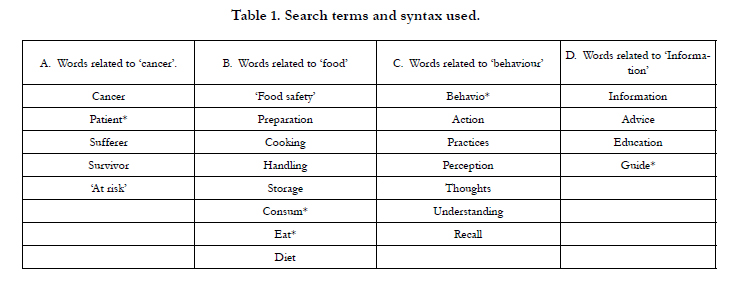

Table 1. Search terms and syntax used.
Defined inclusion criteria (presented within Table 2) were used to guide the search and ensure that only the most relevant studies were included in the review.
Following the initial database search, study tittles were searched by hand before being screened against the inclusion criteria, first on the basis of title and abstract (R1 - round one screening) and then using the full text (R2 - round two screening). All excluded papers and the reasons for their exclusion, were reviewed by a second researcher, although no changes were made following this review. Reference chaining was also conducted for included studies. A PRISMA flowchart containing details of the search and screening output is provided in Figure 2.
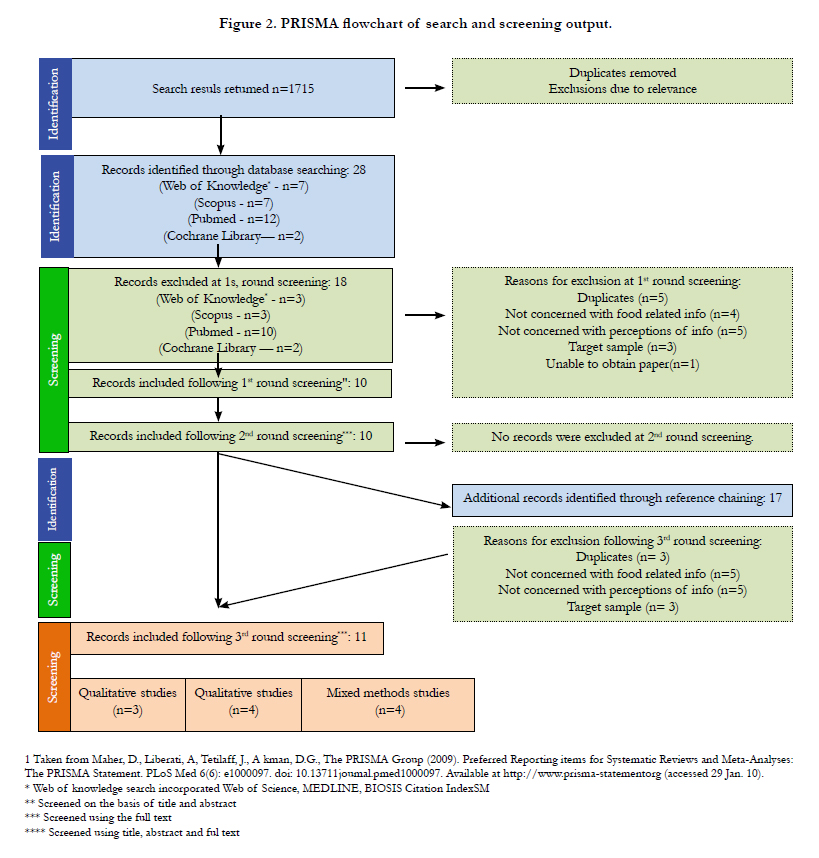
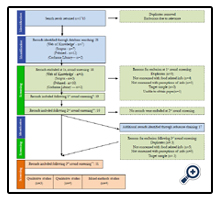
Figure 2. PRISMA flowchart of search and screening output.

Table 2. inclusion/exclusion search criteria.
A single mixed methods critical appraisal tool was sought to evaluate the quality of all studies. This was deemed preferable to selecting different appraisal tools to rate the qualitative and quantitative research, in order to provide continuity of approach and a more robust comparative appraisal. The Mixed Methods Appraisal Tool (MMAT, [10]) was selected due to its applicability to diverse research methods.
The MMAT provides bespoke appraisal criteria for the different methodological approaches used within the research, namely: Qualitative, Quantitative randomised controlled trials, Quantitative non-randomised, Quantitative descriptive and Mixed methods. Criteria are presented as specific questions to which the researcher must select a response of ‘Yes’, ‘No’ or ‘Can’t tell’ and record the rationale for their response. An overall quality appraisal score (of 0, 25, 50, 75 or 100%) can then be generated for each paper (based on the weakest component), in addition to a descriptive summary.
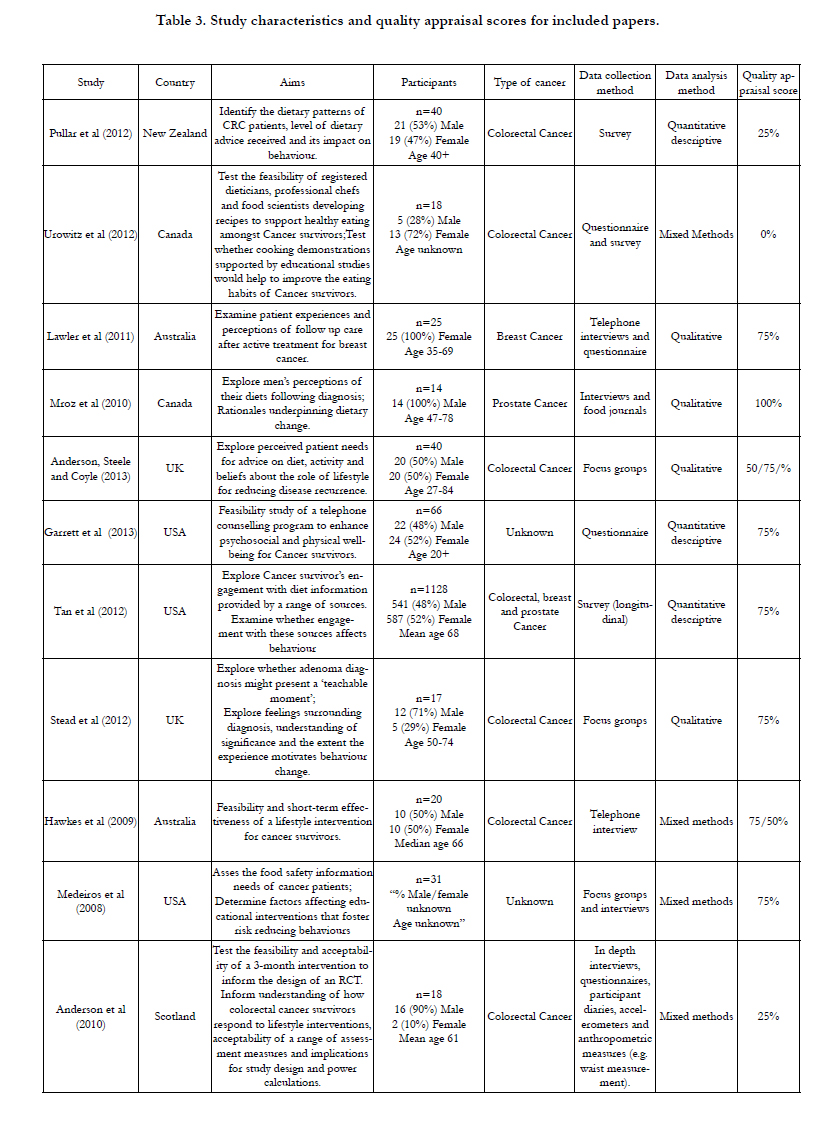
Table 3. Study characteristics and quality appraisal scores for included papers.
Firstly, relevant data was extracted from each of the included studies. This was done by copying all text excerpts from the results sections of each study and recording the theme assigned to these excerpts by the author(s). When no authors’ theme was provided, the researcher allocated their own theme based on their interpretation of the information.
Constant comparison of themes was then conducted by laying out all data excerpts in an open space and ‘eyeballing’ the theme titles, authors’ commentary and participant quotes for similarities and differences. These were then re-grouped together under descriptive themes, before being reviewed by the second researcher.
Interpretive thematic analysis was then used to generate a set of analytic themes following constant comparison of the data. An explanation/rationale for these themes was also articulated, with the support of quotations and implications for findings drawn out [11].
Results
Following the initial database search, a total of 1715 studies were returned. Following screening, 10 papers were included. With a further paper added following reference chaining. A synthesis of 11 papers was therefore conducted.
The included studies incorporated a range of research methods including qualitative (n=4), quantitative descriptive (n=3) and mixed methods (n=4). Following independent quality appraisal, the scores assigned for all papers were reviewed by both researchers. There was high agreement between researchers regarding the quality appraisal scores assigned to 9 out of 11 studies, with variable quality out of a potential score of 100% identified (n=1 scored 0, n=2 scored 25%, n=5 scored 75%, and n=1 scored 100%). Two papers were rated 1 mark differently by the researchers. Following detailed discussion of the rationale for these rating, both researchers felt that their scores were appropriate and hence a duel score of 50/75% was given to these papers [12, 13].
Overall, the modal score assigned across all studies was 75%. Only one research paper [14] received the highest possible appraisal score of 100. A single research paper [15] also received the lowest possible appraisal score of 0%, as it failed to meet any of the criteria specified (see Table 3 for individual quality appraisal scores).
The 11 included papers encompass research conducted in the UK (n=3), America (n=3), Canada (n=2), Australia (n=2) and New Zealand (n=1). Studies were varied in their research design, with four using mixed methods, four using qualitative methods and three studies using quantitative descriptive research design (n=3). Colorectal cancer survivors were the most frequent research participants across the 11 papers (n=6), and the majority of studies (n=8) included a combination of both male and female participants. The age range of participants (where known) was 20-84 years, with participant numbers ranging from 14-1128.
Findings & Implications For Practice
Following interpretive thematic analysis, five key themes were identified, along with10 sub themes (as illustrated within Figure 3). Each theme and sub-theme is presented within Table 4, along with a record of the papers where these constructs were present, and a first order construct to illustrate the theme.
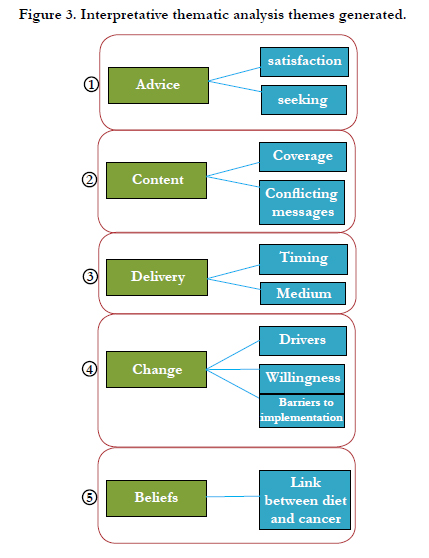
Figure 3. Interpretative thematic analysis themes generated.
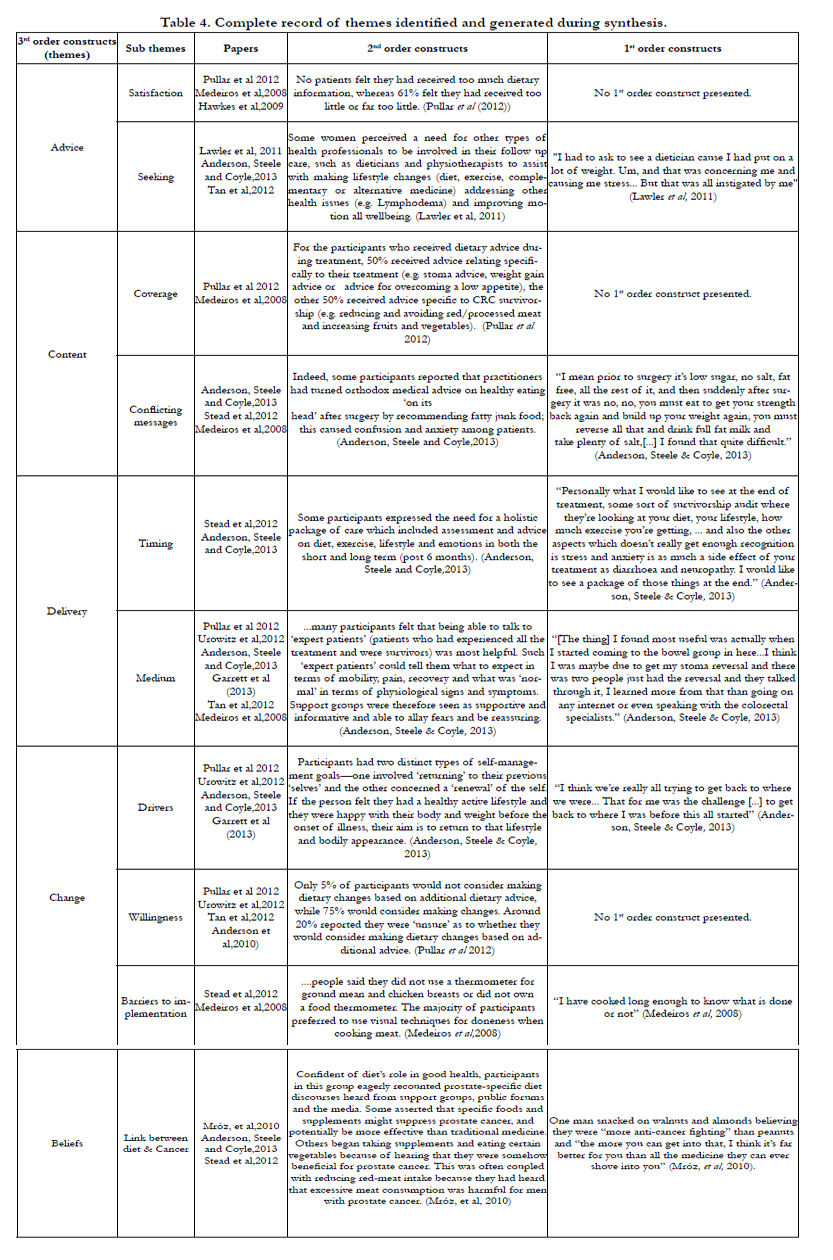
Table 4. Complete record of themes identified and generated during synthesis.
With regards to satisfaction with advice, one study [16] comparing obese patients with healthy/low weight individuals identified a difference in perceptions of advice provision between these two groups. All obese study participants reported that they had not received dietary advice, however relatively even numbers in each participant group were provided with such advice. “Despite this 33% of obese participants felt the dietary information received met their needs.”
Another study [13] found different levels of satisfaction depending on the source/channel of information provision:
“…76% of participants rated the programme overall as excellent, 100% rated the health coach as excellent, whilst 75% rated the handbook as excellent.”
Excess of food related information does not appear to be a problem as none of the research cited having too much information as problematic, illustrated by the following Second order quotes:
“No patients felt they had received too much dietary information, whereas 61% felt they had received to little or far too little” [16].
“The majority of patients selected the prototype titled ‘Food Borne Disease and Cancer Patients’ because it contained the most information they needed….” [7].
Information and advice was most commonly sought from the media, friends and family, health professionals and practitioners. Drivers for seeking information from these sources included:
“I had to ask to see a dietician cause I had put on a lot of weight. Um, and that was concerning me and causing me stress...” [20]
“.....diarrhoea and flatulence were daily problems for which they sought simple practical dietary advice on foods to avoid” [12].
“The relief of the all clear combined with a health professional warning you could maybe have a wee bit of help with losing weight to make sure this doesn’t happen again....” [17].
Studies therefore show that patients have a preference to receive more information as opposed to less, so that they are able to select the advice that best meets their needs and circumstance. Most commonly participants sought advice or information in order to lose weight, control bodily functioning or to reduce the threat of illness reoccurrence. This would suggest that advice given also needs to explicitly address these drivers.
The majority of resources focused on provision of dietary/nutritional advice, with only one of the included research papers [7] focused on the provision of food safety information, concerning cooking, handling and storage. The content of food safety advice was explored in detail with recipients citing statistics and information on food borne illness, pathogens and symptoms to be the most helpful content in order to raise awareness of the risk and severity of food borne illness. Bespoke guides for Cancer patients were reported to be helpful, specifically those related to eating away from the home, safe cooking temperatures and safe food storage. In addition, information concerning foods best avoided and why was also met with positive feedback from participants.
Most Participants in this study recalled hearing recommendations to wash their hands frequently as well as washing fruits and vegetables prior to consumption. Recommendations widely accepted by cancer survivors [7] included avoidance of ‘high risk’ foods such as raw seafood, sprouts and unpasteurised juice and dairy products and not handling pets when preparing food.
Some participants reported dislike of the medical terminology used within food safety advice and difficulty pronouncing terms such as cryptosporidiosis and campylobacteriosis [7]. Participants instead reported a preference for text based information to be “…accurate, but not too technical…. Perhaps bullet point format…”. Participants receiving dietary advice and information cited confusion which appears to be routed in the specificity of information provided. Some examples include generic advice to “eat little and often” [12] which resulted in excess weight gain; broad information branded as ‘useless’ following a suggested trial and error approach to identify foods in response to problems experienced with bodily functions [17]. Dissonance of information was another source of confusion, as participants received information from practitioners which appeared to conflict with population recommendations, such as “the odd bit of vegetable that’s not green in colour and maybe half the fruit a day” [12], as opposed to the standard guidance to eat five portions per day; and recommendations to consume fatty junk food following surgery, e.g. “...eat to get your strength back again and build up your weight again [...] drink full fat milk and take plenty of salt..” [12].
This highlights that cancer survivors are looking for prescriptive guidance that is easy to understand, along with contextual information to appreciate how and why the targeted recommendations provided to cancer survivors may appear to conflict with other generic health guidance they may be familiar with.
With regards to the timing of information and advice provision, the research was inconclusive as illustrated by the following excerpts:
“.....soon after adenoma treatment, whilst recollections of the procedures were still hot" [17].
“.....I would like to see at the end of treatment, some sort of survivorship audit where they're looking at your diet, your lifestyle, how much exercise your getting....." [12].
"... early after diagnosis and as soon as the first oncology appointment." [7].
One study delivering telephone counselling received extremely high rates of engagement which was attributed to the flexibility of delivery, at evenings and weekends, access to the counsellor via email and phone and regular appointment reminders [18].
This would suggest that cancer patients would value food related information as part of lifestyle advice and linked to the different phases experienced as a cancer survivor, from diagnosis to after treatment completion. This may help to build familiarity with the information and confidence to implement the recommended practices.
There were conflicting findings across the literature with regards to the preferred interpersonal source of dietary advice, as illustrated by the following excerpts:
“The most frequent source of dietary advice was a dietitian or friend/family member. No patients reported receiving dietary information from doctors or nurses.” [16].
“Participants reported that the most common type of exposure to dieting information came from discussions with their physicians [19].
Moreover, positivity was expressed for the usefulness of cooking demonstrations, supplemented with recipe booklets and education [15].
In the context of food handling practices: “The patients preferred that physicians (five of six focus groups) or nurses (five of six focus groups) provide the information.” [7]. Nutritionists were also cited as credible sources.
Secondary to interpersonal sources of information, were written brochures/booklets, pamphlets, or fact sheets [16, 12]. Fact sheets were also cited as the preferred format for receiving safe food handling advice [7]. Other less frequently cited modes of food related advice included:
- Media sources - stumbling across as opposed to actively seeking dietary information [19].
- Web sites/forums [7,12].
- CD or downloadable PDF [16].
- Telephone helplines, such as Bowel Cancer UK [12].
- Support groups offering opportunity to talk to so called 'expert patients', who had first-hand experience of cancer treatment [12].
One study [7] identified that cancer patients were more likely to follow advice provided by nutritionists, physicians or nurses, perceived to be credible, as opposed to other sources such as the media, health coaches, herbalists and naturopathic doctors who were cited less frequently. Another highlighted the value added by different mediums, as exemplified within the following participant quote:
“ [the thing] I found most useful was actually when I started coming to the bowel group in here...I think I was maybe due to get my stoma reversal and there was two people just had the reversal and they talked through it, I learned more from that than going on any internet or even speaking with the colorectal specialists” [12].
Whilst there is a broad range of formats and channels used to communicate food related information, those most commonly used and cited were documented takeaway information and/or interpersonal discussions with health professionals or practitioners. It is possible however that less formal interpersonal channels, such as forums and support groups may not be seen as information sources but rather sources of social support.
A range of factors were cited which motivated individuals to make food and lifestyle changes. These included “the constant threat of [illness] reoccurrence” [14], reaching a desired vision of self, either by returning to their pre-cancer lifestyle and body shape or creating a new healthy self-identity [12], and fear of foodborne illness or related death [7].
Information, advice and increasing personal knowledge were often cited as instigators for change, leading to one or more of the above prompts to change. Consequently, it seems as though availability and provision of food related information plays a pivotal role in raising risk awareness, self-reflection and subsequently, facilitating healthy lifestyle change.
Broadly, the data indicates a general willingness to make, or consider making, changes to their food related behaviour and lifestyle, particularly following some form of information or advice [16, 15, 18] as illustrated by the following excerpt:
“...dieting was reported by 49.5% of those who did and only 29.7% of those who did not discuss dieting with their physicians” [19].
“...participants who received the Healthy Options module (n=33),a statistically significant increase in daily consumption of fruits and vegetables was found, from 3.8 to 4.6 daily servings (p=0.02)” [18].
It would seem that information or advice provision serves as a prompt to consider or initiate nutritional behaviour change. The variance in format, channel and content however make it difficult for this review to determine the specific format which is most beneficial for change amongst this at risk population.
Some recommendations were deemed to be ‘common sense’, such as not handling pets whilst preparing food [7], or using a thermometer when cooking meat: “I have cooked long enough to know what is done or not” [7]. Consequently, participants were reluctant to implement such recommendations.
Lack of concern was identified as a barrier to implementing recommendations, both with regards to food safety [7] and making lifestyle changes [17]. Personal preference for consuming unpasteurised foods, inconvenience of recommended practices and lack of knowledge surrounding ‘dangerous’ foods were all cited as factors contributing to high risk food consumption and handling behaviours [7].
Advice on lifestyle change was also perceived to lack consistency, making it difficult to follow: “If you read the newspapers you realise that whatever you do is bad for you!” [17].
This would suggest that food related advice in future should seek to address common barriers to implementation, namely: justifying the value of advice that may be considered ‘common sense’, conveying risk severity, promoting a consistent message and highlighting substitutions for high risk foods and handling practices that are both convenient and appealing.
Cancer survivors were varied in their perception of the relationship between general health and the onset and survival of cancer, with three broad schools of thought emerging across the research as follows:
a) Positive link between diet and cancer outcomes
Some participants enthusiastically described lifestyle changes that they had made in order to improve cancer outcomes, such as reducing consumption of red meat and increasing consumption of walnuts and almonds for their cancer fighting properties. One individual spoke about implementing a range of recommendation to support optimum immune system functioning, stating “...if your immune system is in tip top shape then you can beat cancer just like you can heal from anything else” [14].
b) Negative/no link between diet and cancer outcomes
Some individuals remained unconvinced by the evidence linking diet with cancer and consequently, showed resistance to making lifestyle change. Some first order quotes exemplifying this include:
“There’s no data on prostate cancer, there’s absolutely no data reliable information about what works and what doesn’t” [14].
“...I think that so called cures occur occasionally for reasons, which people don’t really understand, and food I don’t think has much to do with it” [14].
One researcher also highlighted scepticism over delivering lifestyle advice to cancer patients as this presented a convenient interaction opportunity and “just because it’s the done thing”, regardless of whether such individuals specifically would benefit from lifestyle advice [17].
Other individuals displayed resentment towards the link between diet and cancer, feeling as though they were being blamed for their illness. Instead they attributed stress as a major cause or contributor to their diagnosis [12]. Moreover, a small number of individuals cited the opinion and experience that lifestyle change may actually increase cancer risk and upset bodily functions. Consequently, a need for bespoke tailored advice under regular review was sought by such individuals [12].
c) Diet as a preventative measure.
Lack of understanding concerning causes and prevention of cancer, were exacerbated by the fact that “participants were not encouraged to think about prevention during the treatment process...” [17].
Some participants perceived their diet to be healthy prior to cancer onset and hence, no major improvements were deemed necessary. However, such individuals still reported intensifying efforts and supplementing certain foods [17].
Furthermore, it would seem that some cancer survivors view the progress of their illness as an indicator of their overall health, rather than their health as a risk or indicator of cancer onset or remission. ‘All clear’ messages communicated by health professionals were seen to reinforce current lifestyle behaviours, thus fostering resistance to change. For example, “To me, that tells me that I’m all clear..... so why do I need to change my diet?” [17].
The studies highlight the need to contextualise food related advice with the evidence base for effectiveness and the benefits to both cancer survivorship and general health. Moreover, it illustrates the challenge of encouraging preventative food related health behaviours at a time when individuals already see themselves as fit and healthy.
Discussion
Following a systematic MSR of literature in this field (n=11 studies), it can be said that there is a preference for receiving more information as opposed to less, with survivors primarily seeking prescriptive guidance that is easy to understand, via a broad range of channels, most commonly discussions with health professionals/ practitioners or written takeaway information. Food related information was valued as part of broader lifestyle advice, in particular when linked to the different phases experienced, from diagnosis to after treatment completion. Finally, information or advice provision appears to serve as a prompt to consider or initiate nutritional behaviour change, with cancer diagnosis often referred to as a teachable moment. However, encouraging preventative food related health behaviours at a time when individuals already see themselves and fit and healthy, following remission, is acknowledged to be challenging.
Due to the advances in Cancer research and changes in the channels/ technology used to convey health communications, the researcher chose to limit searches to include only material published within the last six years. This may present a limitation of the current review however, the present review could be supplemented by a review of earlier literature if this is deemed to be useful and relevant to current practice. Furthermore, future studies may wish to incorporate grey literature sources and contact the authors of all included studies to ensure that a fully comprehensive review of literature on the subject has been reviewed.
The quality of the review will be dependent on the quality of the included studies, which in this case was variable. From a pool of 11 relevant studies identified, four studies [16, 14, 15, 19] specially focused on diet, one paper [7] focused on safe food handling practices and five papers [20, 12, 18, 17, 13, 21] explored food related information in the context of wider health services and lifestyle interventions. Understanding cancer patients’ experiences of food related information was not an explicit research objective amongst any of the papers and hence, there was also considerable variation in the research aims and methods employed across the literature identified.
A core strength of this systematic mixed studies review (MSR) is the incorporation of qualitative, quantitative and mixed method studies, enabling synthesis of different types of evidence, and concomitant quality appraisal using the MMAT [22].
Recommendations
The following recommendations for policy and practice can be drawn from present review of current literature.
- Raising perceptions of risk susceptibility seems necessary prior to increasing awareness and perceived efficacy of safe and healthy food related behaviours.
- Increasing the consistency of nutritional messaging through a diverse range of channels would seem beneficial in order to increase consumer confidence to implement.
- Contextualising information relative to the consumer journey, from diagnosis and as a cancer patient though to survivorship and back into normal life.
- Increase consumer awareness of the benefits and risks to different food related behaviours such that they are better able to make informed food handling and consumption decisions.
The apparent lack of relevant research indicates a lack of evidence on which to base definitive decisions for future practice however. In particular, with regards to food safety messages. Further research in this area is therefore required in order to better inform this population group and meet their needs with respect to both nutrition and food safety information.
Conclusion
To conclude, this review sought to better understand Cancer survivors’ perceptions of food related information, with a view to enhancing the effectiveness of such information in future. Based on the findings, survivors appear to seek simple, relevant and prescriptive guidance via practitioners and paper based channels. If cancer survivorship is to be capitalised as a teachable moment with regards to improving food safety and nutrition, further empirical research is necessary to understand and enhance food related behaviours amongst cancer survivors, an acknowledged ‘at risk’ group.
References
- Cancer Research UK (2015) Cancer Statistics for the UK, retrieved August 2015 from
http://www.cancerresearchuk.org/health-professional/cancerstatistics. - Cancer Research UK (2014) Data Table: Cancer cases and deaths in the UK, retrieved August, 2015 from
http://publications.cancerresearchuk.org/cancerstats/statsincidence/dtcasesdeaths.html, Accessed. - LiveStrong Foundation (2015) Finding and Evaluating Cancer Information, retrieved August, 2015 from
http://www.livestrong.org/we-can-help/justdiagnosed/finding-and-evaluating-cancer-information/ - Greenstreet BermanLtd (2011) Evidence review of food safety behaviours in the home. Food Standards Agency.
http://www.food.gov.uk/sites/default/files/700-1-1185_X04009_FINAL.pdf - Food Standards Agency (2010) Science and Evidence Strategy 2010–2015. Retrieved August, 2015 from
http://tna.europarchive.org/20110912091909/http://www.food.gov.uk/multimedia/pdfs/publication/sciencestrat0210.pdf - Hof H, Nichterlein T, Kretschmar M (1997) Management of listeriosis. Clin Microbiol Rev 10(2): 345-357.
- Medeiros LC, Chen G, Hillers VN, Kendall PA (2008) Discovery and development of educational strategies to encourage safe food handling behaviours in cancer patients. J Food Prot 71(8): 1666-1673.
- Kendall P, Medeiros LC, Hilliers V, Chen G, DiMascola S (2003) Food handling behaviors of special importance for pregnant women, infants and young children, the elderly, and immunocompromised people. J Am Diet Assoc 103(12): 1646-1649.
- Cooke A, Smith D, Booth A (2012) Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res 22(10): 1435-1443.
- Pluye P, Robert E, Cargo M, Bartlett G, O’Cathain A, et al. (2011) Proposal: A mixed methods appraisal tool for systematic mixed studies reviews.Retrieved on [July 2015] from http://mixedmethodsappraisaltoolpublic.pbworks.com.
- Braun V, Clarke V (2006) Using thematic analysis in psychology. Qualitative Research in Psychology 3(2): 77-101.
- Anderson AS, Steele R, Coyle J (2013) Lifestyle issues for colorectal cancer survivors - Perceived needs, beliefs and opportunities. Support Care Cancer21(1): 35-42.
- Hawkes A, Gollschewski S, Lynch B, Chambers S (2009) A telephone-delivered lifestyle intervention for colorectal cancer survivors 'CanChange': A pilot study. Psychooncology 18(4): 449-455.
- Mróz L, Chapman G, Oliffe J, Bottorff J (2010) Prostate cancer, masculinity and food. Rationales for perceived diet change. Appetite 55(3): 398-406.
- Urowitz S, Chiu W, Cockburn M, Dunlop B, Fierini D, et al. (2012) Building Recipes and Understanding Nutrition for Cancer-survivor Health (BRUNCH). J Nutr Educ Behav 44(4): 384-386.
- Pullar J, Chisholm A, Jackson C (2012) Dietary information for colorectal cancer survivors: an unmet need. N Z Med J 125(1356): 27-37.
- Stead M, Caswell S, Craigie A, Eadie D, Anderson A, et al. (2012) Understanding the potential and challenges of adenoma treatment as a prevention opportunity: insights from the BeWEL formative study. Prev Med 54(1):97-103.
- Garrett K, Okuyama S, Jones W, Barnes D, Tran Z, et al. (2013) Bridging the transition from cancer patient to survivor: Pilot study results of the Cancer Survivor Telephone Education and Personal Support (C-STEPS) program. Patient Educ Couns 92(2): 266-272.
- Tan AS, Mello S, Hornik RC (2012) A longitudinal study on engagement with dieting information as a predictor of dieting behavior among adults diagnosed with cancer. Patient Educ Couns 88(2): 305-310.
- Lawler S, Spathonis K, Masters J, Adams J, Eakin E (2011) Follow-up care after breast cancer treatment: experiences and perceptions of service provision and provider interactions in rural Australian women. Support Care Cancer 19(12): 1975-1982.
- Anderson AS, Caswell S, Wells M, Steele RJ, Macaskill S (2010) “It makes you feel so full of life" LiveWell, a feasibility study of a personalised lifestyle programme for colorectal cancer survivors. Support Cancer Care 18(4): 409-415.
- Pace R, Pluye P, Bartlett G, Macaulay A, Salsberg J, et al. (2012) Testing the reliability and efficiency of the pilot mixed methods appraisal tool (MMAT) for systematic mixed studies review. Int J Nurs Stud 49(1): 47-53.





