The Impact of Chronic Diseases on the Quality of Life among Elderly Survivors from Earthquake in-Northern Thailand
Sudnongbua S*
Faculty of Public Health, Naresuan University, Phitsanulok, Thailand.
*Corresponding Author
Supaporn Sudnongbua,
Faculty of Public Health, Naresuan University,
Phitsanulok, Thailand.
Tel: +66 (0) 94 7574800/+66 (0)82 4001221
E-mail: lillysupaporn@gmail.com
Received: July 18, 2018; Accepted: September 26, 2018; Published: September 30, 2018
Citation: Sudnongbua S. The Impact of Chronic Diseases on the Quality of Life among Elderly Survivors from Earthquake in Northern Thailand. Int J Chronic Dis Ther. 2018;4(3):75-81. doi: dx.doi.org/10.19070/2572-7613-1800015
Copyright: Sudnongbua S© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
This study aimed to identify impact of chronic diseases on quality of life among elderly survivors in Northern Thailand. A cross sectional survey, consisting of 90 questions including the 24-item WHOQOL-OLD (World Health Organization Quality of Life in old age) were administered to 197 randomly selected elderly participants suffering from chronic diseases. Cronbach Alpha coefficient of WHOQOL-OLD in Thai version was 0.84 by the process of forward and backward word translation by three bilinguals. Multiple regression analysis was performed to determine the factors included chronic diseases predicting the quality of life. The results presented that the large majority 99% of those were independent elderly people (well elders or social-bound elderly people). Approximately two-thirds of elderly people (62.1%) had the quality of life at a medium level.
Seven factors were statistically significant with Total WHOQOL-OLD and were found to make a unique contribution to this prediction. Correlation for regression was significantly different from zero [F(7, 281) = 16.41, p < .001] with R2 at 0.69. The adjusted R2 value of 0.66 indicates that 66% of the variability in impacts on quality of life among elders with chronic diseases is predicted by 7 factors such as 1) Paralysis/Semi-paralysis, 2) Level of attitudes towards earthquake, 3) Sensory abilities, 4) Autonomy, 5) Past Present and Future, 6) Death and Dying, and 7) Intimacy (being loved or doing love). With respect to recommendation, the aged people with paralysis/semi-paralysis should be the first priority for earthquake preparedness.
2.Abbreviations
3.Introduction
4.Materials and Methods
4.1 Study Design
4.2 Subjects
4.3 Data Analysis
4.4 Ethical Considerations
5.Results
6.Discussion
7.Implications and Future Directions
8.Conclusion
9.Acknowledgements
10.References
Keywords
Chronic Diseases; Earthquake; Quality of Life; Elderly; Northern Thailand.
Abbreviations
UNISDR: United Nations International Strategy for Disaster Reduction; WHOQOL-OLD: World Health Organization Quality of Life in Old Age; ADL: Activities of Daily Living; QOL: Quality of Life; PTSD: Post-Traumatic Stress Disorder.
Introduction
Recently, all nations in the world are faced with the growth of number and proportion of aged people [1]. United Nations Population Fund reported that elderly population built up 12.3% of the world population, and that that number will rise to approximately 22% per cent by 2050 [2]. According to the increase of aged population, health status score among elders in each country in the world has declined with age, as expected. Elderly women have lived longer than elderly men on average, but have had poorer health status. In addition, the number of disabled people in most developing countries seems to rise as the number of elder people continues to grow [3].
With regard to climate change, most countries in the world are concerned with disaster. In 2015, World Conference on Disaster Reduction with convening support from the UN International Strategy for Disaster Reduction (UNISDR) was held in order to focus on world awareness and commitment to address the landscape alteration of natural disasters [4]. According to the disaster preparedness from the UN, government sectors and networks of individuals are strategized on how to improve the preparation for disasters. However, in Thailand the disaster preparedness had not been strategized, until the earthquake occurred in Northern Thailand in 2014 [5]. On 5th May 2014, the 6.3 magnitude quake battered the Northern part of Thailand, where this research took place [6]. Mae Lao district, Chiang Rai province, where the research area was located, was struck by the serious quake. It killed one aged person and injured 32 people [7]. In addition, 54,000 residents in seven districts in Chiang Rai province had been affected suffering 300 aftershocks so far [7]. The quake threatened elderly people’s physical well-being as well as psychological well-being. The aging persons with chronic diseases were more suffered by the quake than other aging people. Those aging might experience chronic stress and anxiety, phobias, and depression [8]. Although the elders with chronic diseases would survive from the quake; they might have impacts on their quality of life.
Cross-sectional survey was employed among elderly people aged 60 years old and over (According to the Thai government and United Nations, elderly people are the people, who aged 60 years old and over.) who had chronic diseases and lived in Mae Lao district, Chiang Rai province, Thailand where affected the earthquake. Of those, 197 were selected randomly by simple random sampling and a questionnaire was administered to those participants. Face to face administration of the questionnaire was regarded as the most suitable way to gather information from those participants.
A questionnaire consisted of close-ended questions emphasized on socio-demography, Barthel ADL (Activities of Daily Living) in Thai version [9, 10], as well as rating scales of WHOQOLOLD (World Health Organization in old age) in Thai version [11-13]. The Cronbach alpha coefficient was 0.84. In terms of the WHOQOL-OLD in Thai version, it was used by the process of forward and backward word translation by three bilinguals.
The subjects used for this study were drawn from all those over the age of 60 (N=1.015) registered with the regional health care center in Mae Lao district, Chiang Rai province, Thailand; an earthquake area in Northern Thailand. One-hundred-and-ninety seven names were randomly selected as potential subjects in this study.
Regarding the cross-sectional survey, its data were analyzed using SPSS. Descriptive statistics such as means, standard deviations, ranges, and frequencies, were used for summarizing Barthel ADL (Activities of Daily Living) as well as subscale of WHOQOLOLD (World Health Organization in old age) [14], sociodemography and characteristics of samples. Standard multiple regression analyses were conducted to identify Barthel ADL, socio-demography, and characteristics that significantly associated with total score of the WHOQOL-OLD.
Human Ethic procedures were approved by Naresuan University’s Human Ethics Committee and carried out in accordance with the tenets of the Treaty of Helsinki. Potential informants were contacted by the researcher and invited to participate in the study. The purpose of the study was explained to them. Also, they were informed that they had their rights to decline to participate, to withdraw from participation at any time or to refuse to answer any questions. The anonymity of the participants was protected with data stored by participant code only and kept in a controlled place. All data were damaged by document shredder and all electronic files were deleted.
Results
In regard to sample characteristics as well as socio-demography shown in Table 1, the majority of respondents were from 60 to 69 years old (According to the Thai government and United Nations, this group is elderly people) (N = 111; 57.5%). The major respondents were female (N = 130; 66.0%), married (N = 107; 54.3%), and lived with spouse (N= 113; 57.7%). In addition, the major respondents had from 1 to 6 years of formal education (N = 101; 51.8%). Half of them are not working (N = 98; 50%). Most of the respondents reported that main source of income were pension from the government (N = 111; 57.2%), and others responded that their source of income were from personal income (N= 50; 25.8%), and children, grandchildren or other relatives (N= 33; 17.0%) respectively. In terms of knowledge and attitudes towards earthquake, majority of them had a medium level of the knowledge (N = 122; 62.9%) and had a medium level of the attitudes (N = 118; 61.5%). With respect to chronic diseases, most of them had hypertension (N = 106; 53.8%). Moreover, most of them were provided support from their family members ( X = 12.68, SD = 2.49).
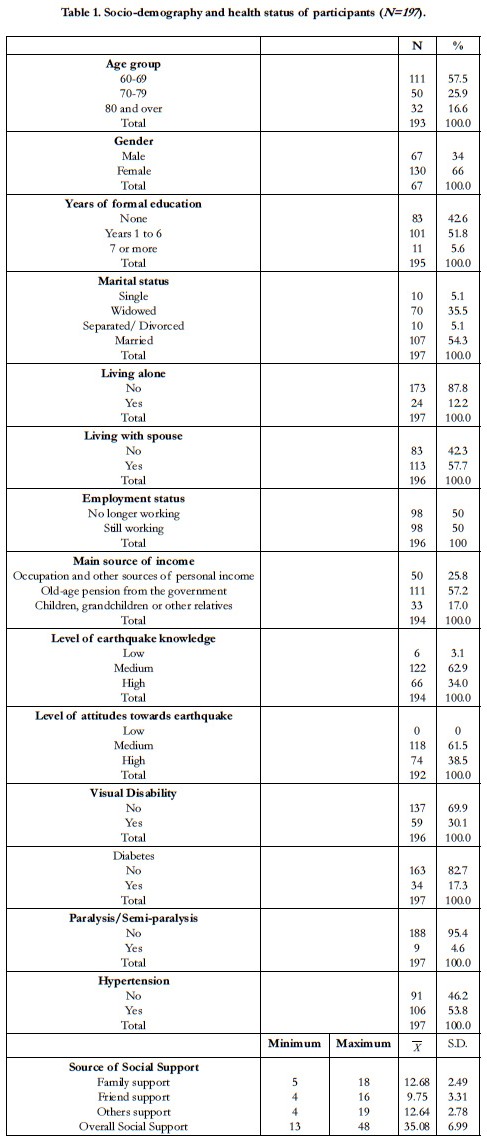

Table 1. Socio-demography and health status of participants (N=197 ).
As can be seen in Table 2, in order to classify the functional level of the subjects who were aging people with chronic diseases, scores of Barthel Activities of Daily Living (Barthel ADL) were employed. It was found that the major respondents were independent elders (well elder or social-bound elderly)(N = 195; 99.0%).
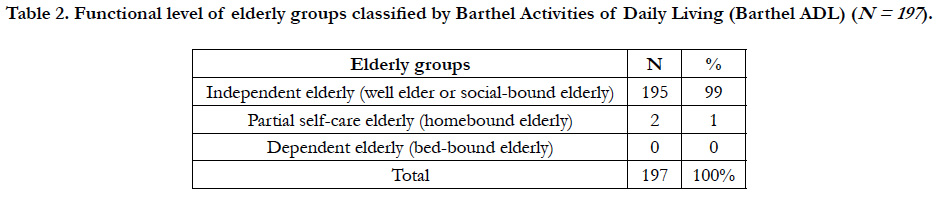
Table 2. Functional level of elderly groups classified by Barthel Activities of Daily Living (Barthel ADL) (N = 197 ).
With regard to a level of quality of life in old age, a WHOQOLOLD questionnaire with 1-5 rating scales was used to classify [14]. The levels were divided into 3 levels regarding QOL scores of each facet: fair level (4-9 scores), medium level (10-15 scores), and good level (16-20 scores). Three levels of total QOL were fair level (24-56 scores), medium level (57-89 scores), and good level (90-120 scores).
Total numbers of respondents were 190. Six facets were measured for quality of life among elderly people: 1) Sensory abilities, 2) Autonomy, 3) Past, present and future, 4) Social participation, 5) Death, and 6) Intimacy. The medium level of quality of life were found in 5 facets which were Sensory abilities (N = 90; 47.4%), Autonomy (N= 111; 58.4%), Past, present and future (N= 109; 57.4%), Social participation (N= 95; 50.0%), and Intimacy (N= 131; 68.9%). Only the facet of Death and dying was a good level of quality of life (N = 89; 46.8%). Moreover, overall level of quality of life from all six facets was medium (N = 118; 62.1%).
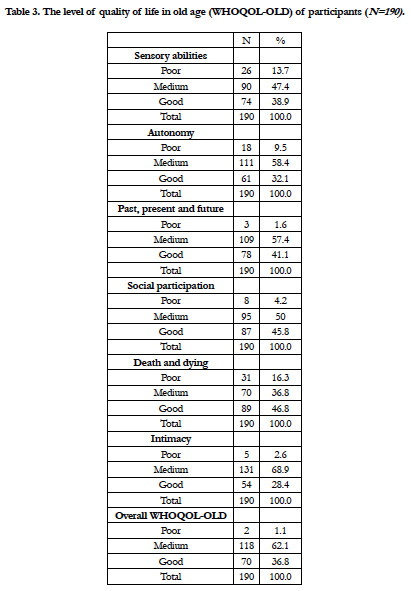
Table 3. The level of quality of life in old age (WHOQOL-OLD) of participants (N=190).
As can be seen in Table 4, the relationship between a dependent variable (Total WHOQOL-OLD) and 15 independent variables; they were Marital status, Years of formal education, Living with spouse, Paralysis/Semi-paralysis, Employment status, Total Barthel ADL, Family support, Level of earthquake knowledge, and Level of attitudes towards earthquake, Sensory abilities, Autonomy, Past Present and Future, Death and Dying, and Intimacy. Preliminary analyses were performed to ensure no violation of the assumptions of normality, linearity and homoscedasticity [15]. There was strong correlation between nine variables with Total WHOQOL-OLD.
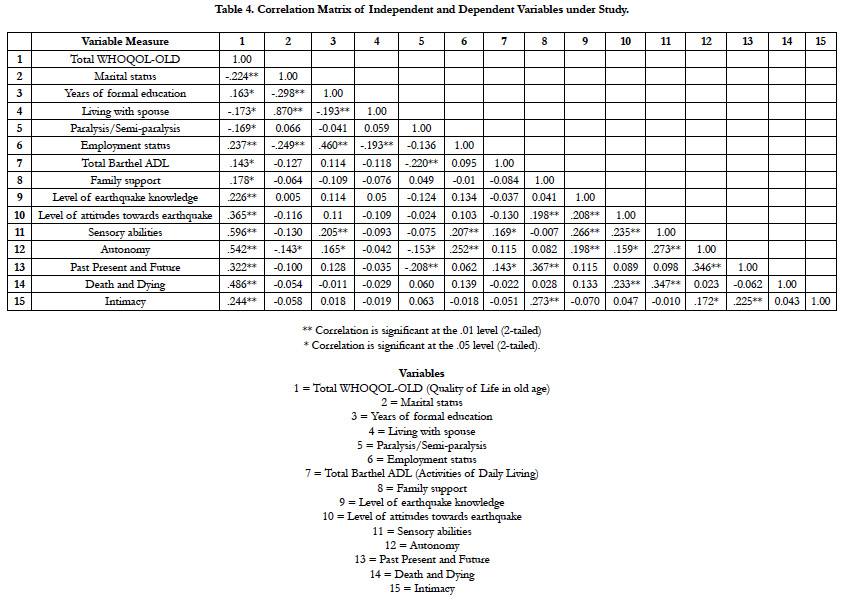
Table 4. Correlation Matrix of Independent and Dependent Variables under Study.
As can be seen in Table 5, standard multiple regression was used to assess the ability of 14 control measures (Marital status, Years of formal education, Living with spouse, Paralysis/Semi-paralysis, Employment status, Total Barthel ADL (Activities of Daily Living), Family support, Level of earthquake knowledge, Level of attitudes towards earthquake, Sensory abilities, Autonomy, Past Present and Future, Death and Dying, and Intimacy) to predict levels of Total WHOQOL-OLD. Preliminary analyses were conducted to ensure no violation of the assumptions of normality, linearity, multicollinearity, and homoscedasticity [15]. The results were found that only seven control measures explained an additional 69% (66% adjusted) of the variance. Seven control measures were statistically significant, with Total WHOQOLOLD. Thus, these seven variables were found to make a unique contribution to this prediction. These variables were Sensory abilities (β = 0.324, p < 0.001), Autonomy (β = 0.343, p < 0.001), Death and Dying (β = 0.316, p < 0.001), Intimacy (β = 0.153, p = 0.001), Level of attitudes towards earthquake (β = 0.138, p = 0.004), Past Present and Future(β = 0.135, p = 0.010), Paralysis/ Semi-paralysis (β = -0.098, p = 0.038) respectively.
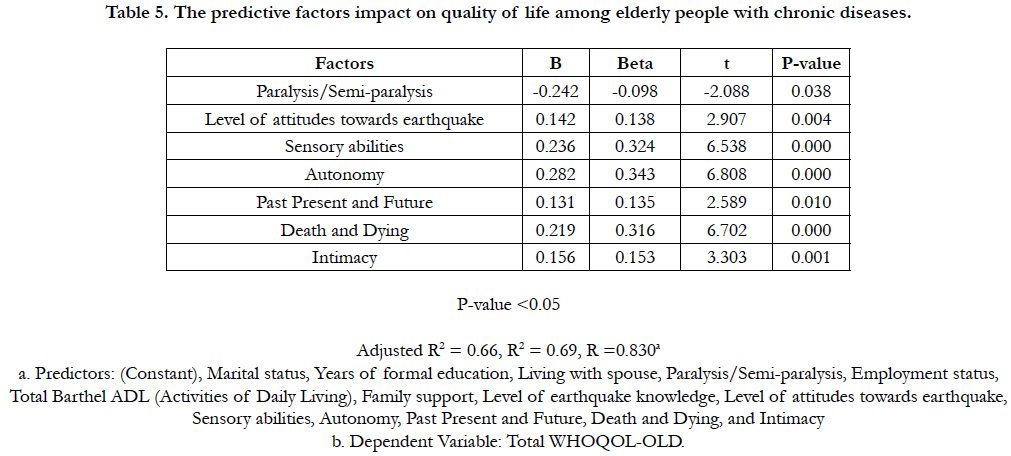
Table 5. The predictive factors impact on quality of life among elderly people with chronic diseases.
Discussion
The discussion integrates the findings to address the research objective. Factors predicting quality of life among elderly survivors, who had chronic diseases, from earthquake in Northern Thailand were Sensory abilities, Autonomy, Death and Dying, Intimacy, Level of attitudes towards earthquake, Past Present and Future, and Paralysis/Semi-paralysis respectively.
Regarding sensory abilities, physical activity of elderly people associates with their quality of life [16]. As aging people’s physical function is decreasing, their sensory abilities will be the obstacles of saving their lives when earthquake happens. In order to save elders, who suffer chronic diseases, from the quake, the government sectors as well as community sectors should plan the strategy of earthquake preparedness for aging people to include young generations or youths who can also help the elderly during the quake situation [17]. In terms of autonomy, the elders who have had chronic diseases may lose their autonomy rather than healthy elders. The findings of this research reflect that autonomy correlates with quality of life, as it was also found in Vagetti G. and et al.,’s study [16].
During earthquake situation, death is a matter that everybody must be scared of. However, the level of death and dying among the aging people’s subjective in this study was good. This means that although they had chronic diseases, they were fearless of dying in earthquake. As they were Buddhists, their religion could decrease death anxiety [18]. Similarly, da Rocha A., and Ciosak S. found that religion could improve fear of death among aging people with chronic diseases [19].
With regard to intimacy in elders, the intimacy measures the ability of an ageing individual in accordance with other people. As 57.7% of aging people in this study lived with spouse, they might share their feelings towards earthquake with their spouse and they could provide emotional support to each other during earthquake.
In regard to level of attitudes towards earthquake, the correlation of variables in this study illustrates that the attitude level towards earthquake improved elders’ QOL (Quality of Life) and this attitudes could encourage them to prepare how to survive from the quake. Also, Cha, E.J. and B.R. Ellingwood found that risk attitudes towards natural hazards led to risk acceptance and disaster preparedness [20]. In addition, fatalistic attitudes towards earthquake can be reduced by disaster risk education [21]. Disaster awareness and attitude can mitigate earthquake hazards [22-24]. These dangers can impact on physical health as well as mental health that lead to low level of QOL [25].
With reference to past present and future of elders, even though this aging people who had chronic diseases were the survivors from earthquake, they had to face with two threatening issues which were 1) chronic diseases, and 2) earthquake. As a result of those two issues, they might not have satisfaction of past present and future. Furthermore, the survivors from earthquake with chronic diseases might be at risk of PTSD (post-traumatic stress disorder) rather than others who had not chronic diseases [26].
Paralysis/Semi-paralysis impacts on QOL among senior people with chronic diseases. In earthquake situation, senior people, who have paralysis/semi-paralysis, need to be the first priority for rescue.
Implications and Future Directions
In order to improve aging people’s QOL in earthquake situation, chronic diseases among senior people in areas of tectonic plates should be evaluated. Earthquake always happen in tectonic plates, therefore if quake preparedness for these elderly people is coordinated by government sectors, community networks included youths, these seniors’ lives will be safe and their QOL will be improved. The earthquake preparedness should also cover physical and mental health. The first group to be rescued should be paralysis/semi-paralysis elders because they cannot survive themselves as healthy elders do. In addition, health care providers and health volunteers should be trained for earthquake preparedness and PTSD (post-traumatic stress disorder) assessments in order to screen psychological effect among elders from the quake. Hence, both physical and mental health among elders should be assessed for assistance. For future research, qualitative methods should be employed for exploring elderly people’s perspectives towards how to save life from the quake. Earthquake preparedness for paralyzed/semi-paralyzed aging people in areas of tectonic plates should be examined by quasiexperimental study.
Conclusion
Summary, the findings of the study found that the quality of life among seniors who had chronic diseases and survived from earthquake was at a medium level. The quality of life among those elderly people was affected by the variables such as Marital status, Years of formal education, Living with spouse, Paralysis/Semiparalysis, Employment status, Total Barthel ADL (Activities of Daily Living), Family support, Level of earthquake knowledge, Level of attitudes towards earthquake, Sensory abilities, Autonomy, Past Present and Future, Death and Dying, and Intimacy. However, of those variables, only seven variables were the determinants to predict the quality of life for these elderly people. Those seven variables were Sensory abilities, Autonomy, Death and Dying, Intimacy, Level of attitudes towards earthquake, Past Present and Future, and Paralysis/Semi-paralysis.
Acknowledgements
I acknowledge the elderly in Mae Lao district, Chiang Rai province, Thailand for sharing their experiences. Also, I kindly thank a community leader, health volunteers and health care providers in Mae Lao district, Chiang Rai province for welcoming me sincerely to access to the research area and providing me the useful information. Without funding, I would not be able to reach the research area. I have to thank the Office of the Higher Education Commission, Ministry of Education in Thailand for providing me a research grant.
References
- United Nations. World Population Ageing. 2015 [cited 2018 Sep 27]. Available from: http://www.un.org/en/development/desa/population/publications/ pdf/ageing/WPA2015_Report.pdf
- United Nations Population Fund (UNFPA). Ageing. [cited 2018 Sep 27]. Available from: http://www.unfpa.org/ageing
- World Health Organization. Global health and aging. Geneva: World Health Organization; 2011 Oct. p. 1-32.
- Women’s Refugee Commission. Community Preparedness: Reproductive Health and Gender. Green Communication Design inc: New York; 2015.
- Fredrickson T. Big earthquake shakes Thailand's North. [cited 2018 Sep 27]. Available from: https://www.bangkokpost.com/learning/learningnews/ 408301/big-earthquake-shakes-thailand-north.
- InterRisk Asia (Thailand) Co., Ltd. Earthquake in Thailand. 2014 May 5.
- Vervaeck A. Very strong deadly earthquake close to Chiang Rai, Thailand - At least 1 dead and 32 injuries and huge number of aftershocks. [cited 2018 Sep 27]. Available from: https://earthquake-report.com/2014/05/05/strongearthquake-thailand-on-may-5-2014/.
- Prasatkul P. The Situation of the Thai Elderly 2014. The Foundation of Thai Gerontology Research and Development Institute (TGRI) and Institute for Population and Social Researh, Mahidol University, Amarin Printing & Publishing: Bangkok; 2015.
- Senanarong V, Harnphadungkit K, Prayoonwiwat N, Poungvarin N, Sivasariyanonds N, Printarakul T, et al. A new measurement of activities of daily living for Thai elderly with dementia. Int Psychogeriatr. 2003 Jun;15(2):135-48. PubMed PMID: 14620072.
- Assesment form of Barthel Activities of Daily Living: ADL. Department of Health, Ministry of Public Health. Nonthaburi province: Thailand; 2016.
- Sudnongbua S. Feelings of abandonment among elderly people in rural Thailand. Massey University, Palmerston North: New Zealand; 2011.
- Sudnongbua S, LaGrow S, Boddy J. Feelings of abandonment and quality of life among older persons in rural northeast Thailand. J Cross Cult Gerontol. 2010 Sep;25(3):257-69. doi: 10.1007/s10823-010-9126-6. PubMed PMID: 20820896.
- LaGrow S, Sudnongbua S, Boddy J. The impact of self-reported visual disability on quality of life among older persons in a rural area of Northest Thailand. J Vis Impair Blind. 2011;105:361-369.
- Power M, Quinn K, Schmidt S. Development of the WHOQOL-old module. Qual Life Res. 2005 Dec;14(10):2197-214. PubMed PMID: 16328900.
- Pallant J. SPSS survival manual: A step by step guide to data analysis using IBM SPSS. 5th ed. Open University Press: New York; 2013.
- Vagetti GC, Barbosa Filho VC, Moreira NB, Oliveira VD, Mazzardo O, et al. Association between physical activity and quality of life in the elderly: a systematic review, 2000-2012. Rev Bras Psiquiatr. 2014 Jan-Mar;36(1):76-88. PubMed PMID: 24554274.
- Uchida Y, Takahashi Y, Kawahara K. Changes in hedonic and eudaimonic well-being after a severe nationwide disaster: The case of the Great East Japan Earthquake. J Happiness Stud. 2014 Feb 1;15(1):207-21.
- Clements R. Intrinsic Religious Motivation and Attitudes toward Death among the Elderly. 1st ed. Pallone N, editor. Taylor & Francis CRC Press: New York; 2018.
- Rocha AC, Ciosak SI. Chronic disease in the elderly: spirituality and coping. Rev Esc Enferm USP. 2014 Dec;48 Spec No. 2:87-93. doi: 10.1590/S0080- 623420140000800014. PubMed PMID: 25830741.
- Cha EJ, Ellingwood BR. Attitudes towards acceptance of risk to buildings from extreme winds. Struct Infrastruct E. 2014 Jun 3;10(6):697-707.
- Baytiyeh H, Naja MK. Can education reduce Middle Eastern fatalistic attitude regarding earthquake disasters?. Disaster Prev Manag. 2014 Jul 29;23(4):343-55.
- Gerdan S. Determination of Disaster Awareness, Attitude Levels and Individual Priorities at Kocaeli University. Eurasian J Educ Res. 2014;55:159-76.
- Topkaya Y, Şimşek U. The Effect of Educational Comics on the Academic Achievement and Attitude towards Earthquake. Int J Educ Sci. 2016 Sep 1;8(3):46-54.
- Suryani I, Sari SA, Milfayetty S, Dirhamsyah M. Increasing Knowledge Of The Earthquake Preparedness Through. Quantum Teaching Model On State Primary School 19 Banda Aceh. Int J Soc Sci. 2014;19:39-44.
- Der-Martirosian C, Riopelle D, Naranjo D, Yano EM, Rubenstein LV, Dobalian A. Pre-earthquake burden of illness and postearthquake health and preparedness in veterans. Prehosp Disaster Med. 2014 Jun;29(3):223-9. doi: 10.1017/S1049023X14000272. PubMed PMID: 24721119.
- Kun P, Tong X, Liu Y, Pei X, Luo H. What are the determinants of posttraumatic stress disorder: age, gender, ethnicity or other? Evidence from 2008 Wenchuan earthquake. Public Health. 2013 Jul;127(7):644-52. doi: 10.1016/j.puhe.2013.04.018. PubMed PMID: 23806187.





