Premature Puberty in Obese Female Children Aged 5-17 in the United States for 2013-2014
Pichainarongk S1, Bidaisee S2*
1 Kasetsart University, Sakon Nakhon, Thailand.
2 St. George’s University, Grenada, West Indies.
*Corresponding Author
Dr. Satesh Bidaisee,
St. George’s University, Grenada, West Indies.
E-mail: sbidaisee@sgu.edu
Received: March 07, 2018; Accepted: April 10, 2018; Published: April 11, 2018
Citation: Pichainarongk S, Bidaisee S. Premature Puberty in Obese Female Children aged 5-17 in the United States for 2013-2014. Int J Chronic Dis Ther. 2018;4(2):70-74. doi: dx.doi.org/10.19070/2572-7613-1800014
Copyright: Bidaisee S© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
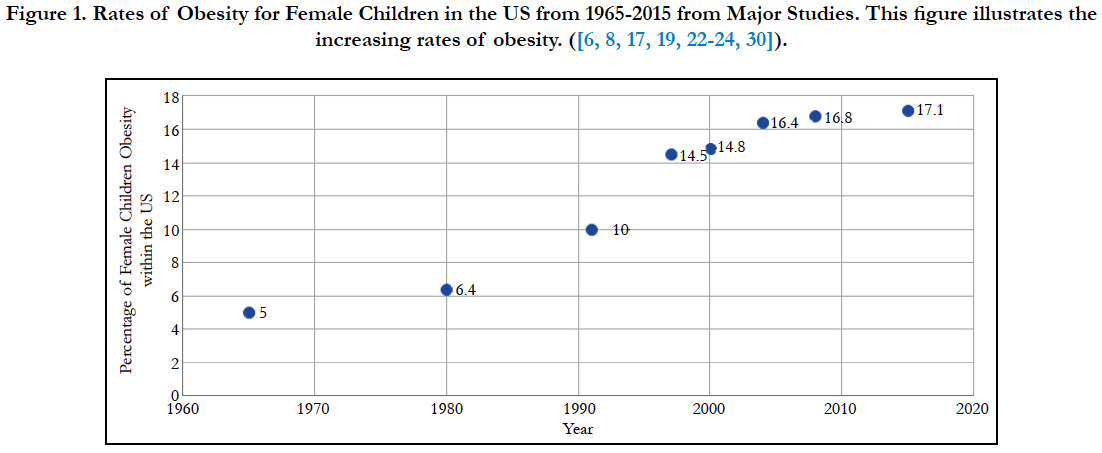
The prevalence of obesity in female children in the Unites States has increased from 5% to 17.1% from 1965 to 2015 and the prevalence of premature puberty has increased as well. Increased weight is correlated with premature puberty in females and interestingly, different studies have shown that there has been a gradual decline of age for onset of puberty. Early sexual maturation in female children are associated with many negative consequences such as increased risk of adult obesity, type 2 diabetes, increased aggression, increased adolescent risk taking behaviors, increased sexual activity, and breast cancer. The target population for this study is obese female children in the United States in the past 5 years. Using the primary data from the National Health and Nutrition Examination Survey (NHANES), the specific study population of obese females aged 5 through 17 years in the United States recorded during the period January 2013 - December 2014. The results of this study also showed a mean BMI of 21.1 which was higher than the 2015 average of 17.1 while a mean age of puberty was found to be 11.3 which is higher than the 2015 average of 9. The strength of correlation was found with Spearman’s Rho. In this study, the results have shown a contrasting view and have shown a negative weak association between the two variables with a rho value of -.089. Efforts towards a reduction of obesity is expected to yield a lowered incidence of premature puberty.
2.Introduction
3.Methodology
3.1 Study Population
3.2 Instrumentation/Materials
3.3 Data Analysis
4.Results
5.Discussion
6.Conclusion
7.Appendices
7.1 Outcomes/Outputs
8.References
Keywords
Premature Puberty; Obesity; Adolescent Health; Female Health.
Introduction
There are several factors that contribute to obesity in children. Some of these elements are unhealthy diets, social/economic issues, and physical inactivity [28]. Unhealthy diets and physical inactivity are instrumental in weight gain by creating a situation where there is an increase caloric intake with a decrease caloric expenditure. In addition, social and economic factors such as amount of money, environment, and lifestyles have been linked to higher rates of obesity [3]. It is worth noting that the negative health impacts of obesity include an increase incidence of type 2 diabetes, osteoarthritis, cardiovascular disease, cancer, and polycystic ovarian syndrome (PCOS) [29].
A significant impact of obesity in female children is the influence on puberty onset. Puberty is the “transition from sexual immaturity to sexual maturity” [6]. There are several physical features that occur in females that represent milestones in normal puberty that are easy to track. Thelarche - the development of breasts and menarche - the first menstrual period is the indicators of female puberty. Several studies, such as [6, 22] have utilized thelarche or menarche to mark the age of puberty onset within females.
Studies such as [6, 8] have shown that increased weight is correlated with premature puberty in females; however, the mechanism is unknown. Furthermore, the prevalence of obesity in female children in the Unites States has increased from 5% to 17.1% from 1965 to 2015 [6, 17, 22-24]. As such, there is a high possibility that the prevalence of premature puberty may have increased as well. The trend of obesity for female children in the United States from 1965-2015 can be found in Figure 1.

In fact, this correlation between obesity and puberty onset was proposed as early as 1960. In 1971, Frisch and Revelle suggested the critical weight hypothesis which suggested that weight of 48kg was required to initiate puberty. Frisch and Revelle’s study supported the idea that weight was associated with early puberty [16]. Other studies supported this trend with the use of data from the Pediatric Research Office Setting (PROS), National Health and Nutrition Examination Survey (NHANES) I, II, III, 1999, 2004, 2008 [5, 6, 17, 19, 24].
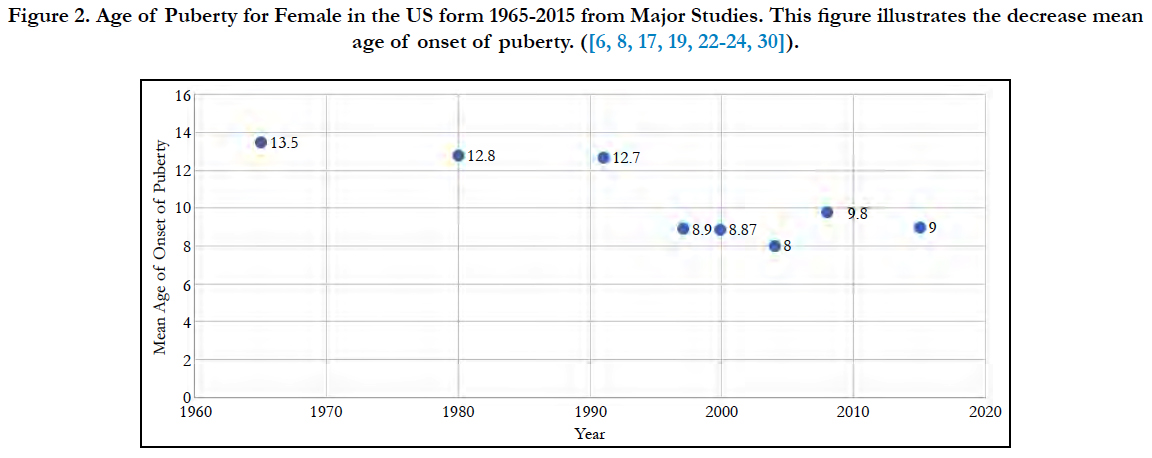
Interestingly, different studies have shown that there has been a gradual decline of age for onset of puberty [8]. In 1963, the average age of puberty in females in the U.S. was 13.5 [24]. Numerous studies have tracked the decrease of age which, in 2015, reached 9.95 [30]. Other countries such as China, Korea, Caribbean, and Sweden reported similar trends of premature puberty [1, 4, 7, 20]. The trend of puberty onset within the United States for females from 1965-2015 can be found in Figure 2.
With increased rates of obesity and early onset of puberty, female children and adolescent suffer from many adverse effects. The adverse effects from obesity and premature puberty have a large economic impact [9]. One common condition seen in both obesity and premature puberty is diabetes. In the United States, diabetes related costs were estimated to be 176 billion in 2012 [2]. These costs were incurred during visits to the emergency department for treatment and medications, and for treatment of complications such as amputations due to narrowing of blood vessels and reduction of blood flow to limbs. These costs were for diabetes alone; however, females with obesity and premature puberty will go through life potentially paying for associated conditions such as diabetes, osteoarthritis, cardiovascular disease, cancer, and PCOS.
Early sexual maturation in female children are associated with many negative consequences such as increased risk of adult obesity, type 2 diabetes, increased aggression, increased adolescent risk taking behaviors, increased sexual activity, and breast cancer [5, 26]. According to [26], females that experience premature puberty were two times more likely to engage in sexual intercourse and give birth by the age of eighteen. In 2010, teen pregnancy was estimated to account for 9.4 billion dollars of U.S. taxpayers’ money [10]. This estimate can be accounted for by the cost of increased healthcare, foster care, and increased incarceration of the children born to these teen parents.
In addition, females who had premature puberty were more likely to have delinquent behaviors such as “fighting, shoplifting, and weapon possession” [26]. One study [25], found a positive correlation between premature puberty and increased delinquency. In the United States, the estimated cost of incarceration of youths is 21 billion dollars which represents the cost of confinement and care of these individuals [21]. This situation demonstrates the need for public health interventions to be implemented to reduce the prevalence of obesity and premature puberty as well as to avoid the adverse short and long term health consequences and crippling costs of these diseases.
Although historically the connection has been made that increased obesity influences early onset puberty, little action has been taken by the public health sector to reduce this issue. Moreover, given the far-reaching health and economic effects of premature obese females, adequate and effective public health interventions need to be implemented. However, to do so, current trends need to be established. Based on the relationship between obesity and puberty, a high rate of obesity among children will coincide with high rates of premature puberty.
The target population for this study is obese female children in the United States in the past 5 years. Using the primary data from the National Health and Nutrition Examination Survey (NHANES), the specific study population of obese females aged 5 through 17 years in the United States recorded during the period January 2013 - December 2014 were selected. The NHANES study population came from 15 counties which included the four major regions of the U.S. (North, South, West, and East inclusive of metropolitan and non-metropolitan areas). The study population had a range of races (Black, Hispanic, Asian, Caucasian) and different economic background (low and non-low income).
For this study, the inclusion criteria are all female participants age 5-17 between January 2013 - December 2014 who had all three variables (height, weight, and age of puberty). The age of 5 was set as a minimum to make sure any outliers would be included in the study since the mean age of puberty in the U.S. in 2012 was 9 [5, 18]. The maximum age of 17 was set, since the age of 18 is considered an adult in the U.S. [30]. The time range was chosen due to the availability of the most recent data. The criteria that all data must be present was done to provide simplicity and avoid statistical issues that exist with other methods that deal with missing data; such as, the decrease of correlation estimate when using the mean/mode substitution [15].
The exclusion criteria for this study included all male participants, all individuals greater than 17 years, all female participants less than 5 years, and any participant with missing data. The age cutoff was set due to the same reasoning mentioned in the inclusion criteria. Males were excluded since the focus of the study is only females. The removal of any participant with missing data was done for simplicity and avoidance of statistical problems.
This study is a secondary data analysis of data collected from the National Health and Nutrition Examination Survey (NHANES), which was conducted by the CDC for the period between 2013- 2014. As such, no instrument was needed. The NHANES is a survey comprised of physical examination, interview, and laboratory testing done at mobile testing centers. The survey included questions relating to demographic background, health, and nutrition such as, “How many of those meals {did you/did SP} get from a fast-food or pizza place?” [11]. Part of the survey can be seen in Appendix A. In the CDC’s data collection, the question this study is most concerned with is, “How old {were you/was SP} when {you/she} had {your/her} first menstrual period” [11, 12]. This survey can be seen in Appendix B. With the use of this question and the palpation of breast buds by trained physicians, the age of puberty was determined.
Another two variables within the CDC’s data collection that are important are height and weight [12, 16]. These were collected using calibrated scales and measuring tape at each mobile center. Details on how NHANES collected can be found below. The NHANES collects data from 5,000 participants from 15 different counties per year (10,000 participants for the selected period), who were selected from the four major regions of the US including metropolitan and non-metropolitan areas. Participants included males, females, children, and adults aged 0 - 85+ of all races. The selection of participants was done with a stratified clustered random sampling. The first step was the random selection of primary sampling units (counties). Within the counties, a random selection segment was chosen containing clusters of households. Participants were then selected from these households.
Within this study, there is one dependent and independent variable. The dependent variable is the age of puberty measured in years. The independent variable is BMI which is calculated from weight (kg) and height (cm) with the following equation: weight (kg) divided by height (cm) squared (BMI= (kg/[cm]2)*10,000). These variables will be the ones used in statistical analysis.
Before the analysis of the secondary data, it is important to establish the procedures for recording, storing, handling of missing data, and reducing data. The original data was taken from the CDC website and stored as a XPT file. The data was manual reduced using the inclusion and exclusion criteria stated above. The reduced data was then used to determine the descriptive statistics to examine the distribution of obesity (BMI) and age of puberty, which included range, mean, and standard deviation. In addition, standard error was also calculated to determine how well a sample mean represents the true population mean. Since the Shapiro-wilk test showed a significance of < .000 for both calculated BMI and age of puberty, the data was considered nonparametric and thus a Spearman’s correlation was used to measure the strength of association. A p-value of less than 0.05 will be considered statistically significant [27]. This level was chosen based on statistical standards. In addition, the confidence interval will be at 95% [28]. This interval was chosen based on statistical standard and since the study is not a clinical trial, a confidence interval of 99% is not required.
Results
The original NHANES data set contained 10,175 male and female participants. After applying the female criteria, only 5,171 participants were left. Selecting participants in the age range of 5-17 resulted in 388 participants being left. Finally, after excluding all missing data points, the final sample size was n=156.
The descriptive statistics of the two variables of calculated BMI and age of puberty (age when first menstrual period occurred) were calculated which entails standard error, mean, range and standard deviation. The minimum and maximum of calculated BMI was 12.10 and 45.20 respectively with a range of 33.10. The mean BMI was 21.1218 with a standard error of .51545 and a standard deviation of 6.43803. The confidence interval was found to be 20.1036 - 22.1400. The minimum and maximum of age of puberty was 8 and 15, respectively. The range of this variable was found to be 7. The mean age of puberty was 11.97 with a standard error of .110 and standard deviation of 1.377. The confidence interval was 11.76 - 12.19. The descriptive statistics for both calculated BMI and age of puberty variables can be found in Table 1.
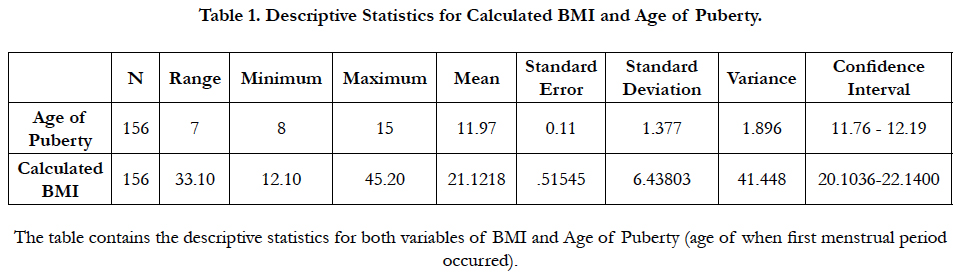

Table 1. Descriptive Statistics for Calculated BMI and Age of Puberty.
The strength of correlation was found with Spearman’s Rho. The value was -.089 which represents a very weak negative strength of correlation between age of puberty and BMI. These results were not statically significant since the p value was .271. The results for the spearman correlation can be found in Table 2.
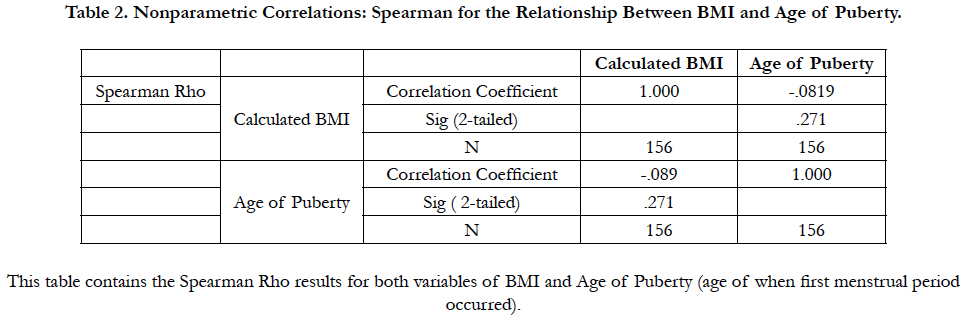
Table 2. Nonparametric Correlations: Spearman for the Relationship Between BMI and Age of Puberty.
Discussion
There have been multiple studies that have connected obesity with an early onset of puberty in females such as [6, 8, 13]. In these studies, there was a negative association between the two variables with an earlier onset of puberty as BMI increased. In this study, the results have shown a contrasting view and have shown a negative weak association between the two variables with a rho value of -.089. However, these results were not statistically significant since the p value was .271, well above our standard p value of .05.
In addition, the mean age of puberty and BMI are different from previous studies. The mean age of puberty was found to be 11.3 which are higher than the 2015 average of 9 [5]. The results of this study also showed a mean BMI of 21.1 which was higher than the 2015 average of 17.1 [5]. Despite the weak association found in this study, the mean BMI has followed the increasing trend found in other studies. However, the mean age of puberty has not followed the trend and has increased when compared to other studies.
Some weaknesses of this study are the effects of race as a confounder and recall bias for the age of first menstrual period. Race as a confounder could have made an impact on the results is of age of puberty. There have been multiple studies that have documented an early onset of puberty for African American girls when compared to white [7, 31, 32]. However, this study did not separate the two due to the original data not containing information regarding the race of participants. This confounder could have led to the difference found in the mean age of puberty when compared to other studies. Another potential problem is recall bias for the determination of first menstrual period. This age was used to indicate the initiation of puberty. Recall could have impacted the results to be either higher or lower and may have led to the difference of mean age of puberty.
Generally, the negative health impacts of obesity include increased incidence of type 2 diabetes, osteoarthritis, cardiovascular disease, cancer, and polycystic ovarian syndrome (PCOS) [14, 29]. However, a significant impact of obesity in female children is the influence on puberty onset. Studies such as [6, 8, 31, 32] have shown that increased weight is correlated with premature puberty in females. Development of earlier sexual maturation is associated with many negative effects such as increased aggression, increased sexual activity, increased risk of adult obesity, increased adolescent risk taking behavior, type 2 diabetes, and breast cancer [5, 26].
There are numerous negative health consequences of increased obesity and early onset of puberty as discussed above. In addition to the negative health consequences there are negative economic consequences associated with these health problems. Due to these negative consequences, despite the weak association and different results for obesity and age of puberty, it is its essential for public health to become involve and try to decrease the prevalence of obesity and thus eventually prevent the decrease age of onset of puberty. Therefore, it’s important for other studies to be performed to continue examines the association of obesity and premature puberty and also the effects of interventions targeting obesity reduction.
Conclusion
One important public health issue that the world faces is obesity. The prevalence of obesity has amplified. Along with this, the rates of health problems associated with obesity is increased. Diseases such as diabetes, osteoarthritis, cardiovascular disease, cancer, premature puberty, and PCOS. With premature puberty, there are other adverse effects associated such as breast cancers, increased adolescent risk behavior, obesity, and type 2 diabetes. These all have negative consequences such as increased economic costs, morbidity, and mortality. It is extremely important that public health find ways to reduce obesity. With a reduction of obesity, a lowered incidence of premature puberty should follow and allow patients and society to avoid these adverse health consequences and crippling costs.
From the results of this study, there are multiple anticipated outcomes. The expectation is to use these findings to increase awareness of the relationship between obesity and premature puberty. From the increased awareness of this relationship, interventions can be formed to reduce premature puberty with the most obvious intervention being ways to reduce rates of obesity. In addition, more studies can be done to examine the effectiveness of these different interventions.
There are many outputs that will be used to demonstrate the findings of this study. Some examples of outputs are as follows: publication in a journal, capstone presentation, and conference presentation. It is important to have outputs in academic schools, journals, and conferences to help raise interest and knowledge of the relationship of obesity and premature puberty to help find ways to reduce rates of premature puberty.
References
- Aksglaede L, Juul A, Olsen LW, Sorensen TI. Age at puberty and the emerging obesity epidemic. PloS one. 2009 Dec 24;4(12):e8450. PubMed PMID: 20041184.
- American Diabetes Association. The 10-year cost-effectiveness of lifestyle intervention or metformin for diabetes prevention: an intent-to-treat analysis of the DPP/DPPOS. Diabetes care. 2012 Apr 1;35(4):723-30. PubMed PMID: 22442395.
- Ball K, Crawford D. Socio-economic factors in obesity: a case of slim chance in a fat world?. Asia Pac J Clin Nutr. 2006;15 Suppl:15-20. PubMed PMID: 16928657.
- Benedet J, Adami F, de Fragas Hinnig P, de Vasconcelos FD. Association of sexual maturation with excess body weight and height in children and adolescents. BMC Pediatr. 2014 Dec;14(1):72.
- Biro FM, Greenspan LC, Galvez MP. Puberty in girls of the 21st century. J Pediatr Adolesc Gynecol. 2012 Oct;25(5):289-94. PubMed PMID: 22841372.
- Biro FM, Khoury P, Morrison JA. Influence of obesity on timing of puberty. Int J Androl. 2006 Feb;29(1):272-7. PubMed PMID: 16371114.
- Boyne MS, Thame M, Osmond C, et al. Growth, body composition, and the onset of puberty: longitudinal observations in Afro-Caribbean children. J Clin Endocrinol Metab. 2010 Jul;95(7):3194-200. PubMed PMID: 20427487.
- Burt Solorzano CM, McCartney CR. Obesity and the pubertal transition in girls and boys. Reproduction. 2010 Sep;140(3):399-410. PubMed PMID: 20802107.
- Cawley J, Meyerhoefer C. The medical care costs of obesity: an instrumental variables approach. J Health Econ. 2012 Jan;31(1):219-30. PubMed PMID: 22094013.
- Centers for Disease Control and Prevention. Reproductive Health: Teen Pregnancy. 2017 May.
- Centers for Disease Control and Prevention. National health and nutrition examination survey. 2017 March 14.
- Centers for Disease Control and Prevention. BMI. 2017 March 3.
- Cheng HG, Phillips MR. Secondary analysis of existing data: opportunities and implementation. Shanghai Arch Psychiatry. 2014 Dec;26(6):371-5. PubMed PMID: 25642115.
- Chitnis T, Graves J, Weinstock‐Guttman B, et al. Distinct effects of obesity and puberty on risk and age at onset of pediatric MS. Ann Clin Transl Neurol. 2016 Nov 4;3(12):897-907. PubMed PMID: 28097202.
- Enders CK. Applied missing data analysis. Guilford Press; 2010 Apr 23.
- Frisch RE, Revelle R. Height and weight at menarche and a hypothesis of menarche. Arch Dis Child. 1971 Oct;46(249):695-701. PubMed PMID: 5118059.
- Foster DL, Yellon SM, Olster DH. Internal and external determinants of the timing of puberty in the female. J Reprod Fertil. 1985 Sep;75(1):327-44. PubMed PMID: 4040975.
- Gregory KE, Radovinsky L. Research strategies that result in optimal data collection from the patient medical record. Appl Nurs Res. 2012 May;25(2):108-16. PubMed PMID: 20974093.
- Herman-Giddens ME, Slora EJ, Wasserman RC, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics. 1997 Apr;99(4):505-12. PubMed PMID: 9093289.
- Heo JS, Moon HS, Kim MK. A Study on Dietary Habits and Lifestyle of Girls with Precocious Puberty. Pediatr Gastroenterol Hepatol Nutr. 2016 Jun;19(2):130-8. PubMed PMID: 27437190.
- Justice Policy Institute. Calculating the Full Price Tag for Youth Incarceration. 2017 May 31.
- Kaplowitz, Kaplowitz PB. Link between body fat and the timing of puberty. Pediatrics. 2008 Feb;121 Suppl 3:S208-17. PubMed PMID: 18245513.
- Kaplowitz PB, Slora EJ, Wasserman RC, Pedlow SE, Herman-Giddens ME. Earlier onset of puberty in girls: relation to increased body mass index and race. Pediatrics. 2001 Aug;108(2):347-53. PubMed PMID: 11483799.
- Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls. Arch Dis Child. 1969 Jun;44(235):291-303. PubMed PMID: 5785179.
- Mrug S, Elliott MN, Davies S, et al. Early puberty, negative peer influence, and problem behaviors in adolescent girls. Pediatrics. 2014 Jan 1;133(1):7-14. PubMed PMID: 24324002.
- Mendle J, Turkheimer E, Emery RE. Detrimental psychological outcomes associated with early pubertal timing in adolescent girls. Dev Rev. 2007 Jun;27(2):151-171. PubMed PMID: 20740062.
- Ogden CL, Carroll MD. Prevalence of overweight, obesity, and extreme obesity among adults: United States, trends 1960–1962 through 2007–2008. National Center for Health Statistics. 2010 Jun;6(1):1-6.
- du Prel JB, Hommel G, Röhrig B, Blettner M. Confidence interval or p-value?: part 4 of a series on evaluation of scientific publications. Dtsch Arztebl Int. 2009 May;106(19):335-9. PubMed PMID: 19547734.
- Sandhu J, Ben-Shlomo Y, Cole TJ, et al. The impact of childhood body mass index on timing of puberty, adult stature and obesity: a follow-up study based on adolescent anthropometry recorded at Christ's Hospital (1936–1964). Int J Obes (Lond). 2006 Jan;30(1):14-22. PubMed PMID: 16344844.
- Shalitin S, Phillip M. Role of obesity and leptin in the pubertal process and pubertal growth-a review. Int J Obes Relat Metab Disord. 2003 Aug;27(8):869-74. PubMed PMID: 12861226.
- U.S. Department of State. When a child becomes an adult. 2017 March 3.
- Wohlfahrt-Veje C, Mouritsen A, et al. Pubertal onset in boys and girls is influenced by pubertal timing of both parents. J Clin Endocrinol Metab. 2016 Jul;101(7):2667-74. PubMed PMID: 27014950.





