A Brief Review for Managing Spasticity in Multiple Sclerosis
Najmi S1, Hormoz A2, Pourabolghasem S1*
1 Assistant Professor of Neurology, Tabriz university of Medical science, Iran.
2 Professor of Neurology, Tabriz University of Medical Science, Iran.
*Corresponding Author
Dr. Shabnam Pourabolghasem
Assistant Professor of Neurology,
Tabriz University of Medical Science,
Iran.
E-mail: ish_pour_gm@yahoo.com
Received: March 19, 2016; Accepted: April 20, 2016; Published: April 22, 2016
Citation: Najmi S, Hormoz A, Pourabolghasem S (2016) A Brief Review for Managing Spasticity in Multiple Sclerosis. Int J Chronic Dis Ther. 2(1), 17-20. doi: dx.doi.org/10.19070/2572-7613-160004
Copyright: Pourabolghasem S© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Spasticity is a common problem in MS. The stiffness often is minimal and not bothersome. Stiffness may become painful and may interfere with performing activities of daily living. Reducing spasticity produces greater freedom of movement and strength and frequently also lessens fatigue and increases coordination. The major ways in which spasticity is reduced include stretching exercises, physical therapy, and the use of medications. If spasticity does not respond to these measures and causes discomfort, a surgical procedure may be necessary. These management methods discussed in brief here.
Treat problems: The first management strategy is to alleviate associated problems that magnify spasticity. These include infection, pain, skin breakdown, and any similar process that may stimulate spasticity.
Stretching: A thorough stretching program includes a series of exercises that are performed in certain sitting or lying positions that allow gravity to aid in stretching specific muscles. Some kind of these methods has been discussed in details in main page.
Mechanical aids: Specific devices (orthose) sometimes are made for certain individuals to counteract spasticity and prevent what are termed contractures.
Medications: Spasticity often is managed most effectively by medications such as Baclofen, Tizanidine, Dopa-agonists and Levodopa, Diazepam, Dantrolene, Cyproheptadin, Gabapentine and others that have been discussed in details in main page.
BTX: A better, more modern technique is the use of botulinum toxin, made by bacteria. This paralytic agent causes a temporary blockage of the nerve and muscle.
Intratecal baclofen: A better approach to the management of severe spasticity involves the use of a pump that delivers baclofen directly into the spinal canal.
Surgical management : For those who have severe intractable spasticity, the kind that causes problems with all functions and is not responsive to exercise or medication, a spasticity-decreasing procedure may be necessary.
2.Introduction
2.1.Treat problems
2.2.Stretching
2.3.Mechanical aids
2.4.Medications
2.5.BTX
2.6.Intratecal baclofen
2.7.Surgical management
3.References
Keywords
Spasticity; Multiple sclerosis; Medication; Surgery.
Introduction
Spasticity means stiffness. It often occurs when demyelination occurs in the nerves that regulate muscle tone. Because many of the nerves in the brain and spinal cord regulate movement and any of them may be affected by demyelination, spasticity is a common problem in MS. The stiffness often is minimal and not bothersome. In fact, a person sometimes needs the stiffness provided by spasticity to stand or pivot. At other times stiffness may become painful and may interfere with performing activities of daily living. Spasticity tends to occur most frequently in a specific group of muscles that are responsible for maintaining upright posture. These muscles are called antigravity or postural muscles. They include the muscles of the calf (gastrocnemius), thigh (quadriceps), buttock (gluteus maximus), groin (adductor), and occasionally the back (erector spine).
When spasticity is present, the increased stiffness in the muscles means that a great deal of energy is required to perform daily activities. Reducing spasticity produces greater freedom of movement and strength and frequently also lessens fatigue and increases coordination.
The major ways in which spasticity is reduced include stretching exercises, physical therapy, and the use of medications. If spasticity does not respond to these measures and causes discomfort, a surgical procedure may be necessary (Table 1).
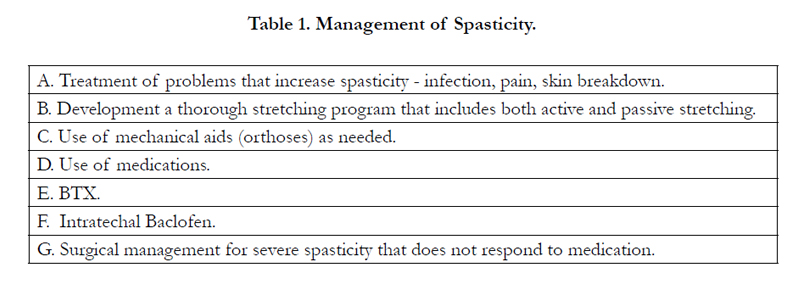

Table 1. Management of Spasticity.
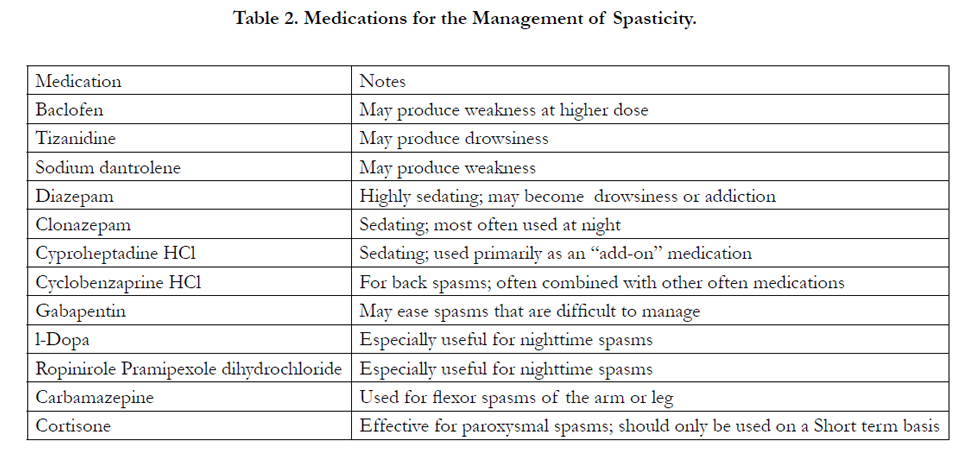
Table 2. Medications for the Management of Spasticity.
The first management strategy is to alleviate associated problems that magnify spasticity. Pain or discomfort anywhere in the body will magnify spasticity. These include infection, pain, skin breakdown, and any similar process that may stimulate spasticity.
The second management strategy is to develop a specific exercise program for stiffness. An independent stretching program based on some of the principles used in physical therapy may be used at home.
A thorough stretching program includes a series of exercises that are performed in certain sitting or lying positions that allow gravity to aid in stretching specific muscles.
While in the sitting position, a towel or long belt may be used to pull on the forefoot and ankle to stretch the calf, or to stretch the thigh muscles when one is lying on the stomach. Certain muscles may be relaxed more effectively while one is lying on the stomach or side or while lying on all fours over a beach ball, rocking rhythmically forward and backward.
The simplest and often most effective way to reduce spasticity is passive stretching, in which each affected joint is slowly moved into a position that stretches the spastic muscles. After each muscle reaches its stretched position, it is held there for approximately a minute to allow it to slowly relax and release the undesired tension.
This stretching program begins at the ankle to stretch the calf muscle, then proceeds upward to the muscles in the back of the thigh, the buttocks, the groin, and, after turning from the back to the stomach, the muscles on the front of the thigh.
Range-of-motion exercises differ from stretching exercises in that the movement about the joint is not held for any specific length of time. Although range of motion is important, holding the stretch is significant, and patience is essential when doing the stretches.
Exercising in a pool also may be extremely beneficial because the buoyancy of the water allows movements to be performed with less energy expenditure and more efficient use of many muscles. Somebody recommends using the pool for both stretching and range-of movement exercises. The pool temperature should be about 28-30 degrees; this may feel cold to some people, but warmer temperatures should be avoided because they produce fatigue. Colder temperatures can actually cause spasticity, thus the temperature of the pool is quite important.
Many people with MS have a limited range of movement in at least some joints and muscles, and the key to managing spasticity is to expand the number and kind of movements that can be performed.
Spasticity also may be reduced by relaxation techniques that involve a combination of progressive tensing and relaxing of individual muscles, accompanied by deep breathing techniques and imagery. Acupuncture may also decrease spasticity for some people, although the mechanism of action of this is not known.
Specific devices (orthose) sometimes are made for certain individuals to counteract spasticity and prevent what are termed contractures, in which the range of movement possible for a given joint becomes restricted as the result of spasticity. For example, a “toe spreader” or “finger spreader” is used to relax tightness in the feet and hands and to aid in mobility. Braces for the wrist, foot, and hand are used to maintain a natural position and to prevent limitations on movement and the development of deformities.
Spasticity often is managed most effectively by medications.
Sacts on the nerves that control the spastic muscles at their site of origin in the spinal cord. It is the most common antispasticity medication used in MS, and most people respond well to it. The dose must be carefully determined for each individual; too little will be ineffective, whereas too much produces fatigue and a feeling of weakness because it interferes with the proper degree of stiffness needed for balance and erect posture. Starting at a low level and slowly increasing the dose until a maximal beneficial effect is obtained usually determine the correct dose. The most common mistake when taking baclofen is to give up on it too soon, so that the dose never reaches the level necessary to attain proper relaxation. That dose may be as low as one half of a pill (5 mg) per day, but some people may need to take as much as 40 mg four times a day. Baclofen is only available as a generic and may be the least expensive medical treatment. Thus it is often the initial drug used. The metabolism of baclofen in the body is relatively quick, and frequent dosing is usually necessary. Allowing each person to understand how the medication affects his or her body and tailoring it individually best do this.
Acts on a different area of the spinal cord than baclofen. It appears to be effective in decreasing stiffness and muscle spasm, with less effect on strength than many other drugs. It must be used carefully and slowly because sleepiness inevitably results if the dose is increased too rapidly. The starting dose is 2 to 4 mg up to a maximum of 36 mg per day. It is quite effective and may be combined with baclofen in problem situations. It is especially useful for nighttime stiffness and spasms.
It is not uncommon for the night to be the worst time for stiffness and spasms. This appears to have something to do with the lack of outside stimulation to the nervous system, making it more sensitive to spasm. This nighttime exaggeration of muscle tone may manifest itself as restless legs. Medications that decrease restless legs may be very useful during the night. These include the medications used in Parkinson’s disease, including pramipexole and Ropirirole HCl (Requip®). L-Dopa (Sinemet®) is another Parkinson’s medication that also decreases spasms, especially the painful spasms that tend to occur at night and may become especially prominent and painful.
Also relieves spasms that occur at night. Its calming effect also helps to induce sleep, but its strong sedative effect limits its use during the daytime. Diazepam must be prescribed with caution because it may become addictive if used too frequently. Clonazepam (Klonopin®) is closely related to diazepam. Its main use has been to treat certain types of epilepsy. It produces significant relaxation, and thus may be used as an antispasticity medication. Like diazepam, it sedates and is best used at bedtime. When using diazepam or clonazepam, both the doctor and the person with MS must pay attention to the potential for chemical dependency. When properly used at appropriate doses, this is not a major problem. However, if the dose must be continually increased and the person is using the medication not for spasticity but as a crutch to escape the realities of the world, it should no longer be used.
Another medication that sometimes is used for spasticity is sodium Dantrolene (Dantrium®), which acts directly on muscles. It is a very potent medication that needs to be used carefully. It may be helpful, but it also may induce weakness, even at low doses.
Cyproheptadine is an antihistamine that has Antispasticity properties and may be a good add-on medication at certain times. Its sedating effect limits its use, but doses of 4 mg taken when needed may be helpful.
A drug that is commonly used for spasms in the muscles of the back is cyclobenzaprine HCl . It acts quite specifically on these spasms, but also may relieve limb spasms. It usually works best in combination with one of the other antispasticity medications.
(Neurontin®), lamotrigine (Lamictal®), topiramate (Topamax®), and pregabalin (Lyrica®) are examples of newer medications that have been approved for use in seizures. These medications also have antispasticity properties and when taken in appropriate doses often ease problematic spasms.
Any of these medications may become less effective when they are taken for a prolonged period (this is referred to as the development of tolerance), and it may be necessary to stop taking them for a period of time, after which they may again become effective.
A better, more modern technique is the use of botulinum toxin, made by bacteria. This paralytic agent causes a temporary blockage of the nerve and muscle. It is easier to control than phenol, but it may require more frequent injections into the muscle. It is practical for treating small muscle spasms, especially those about the eye or face, or single muscle spasms in the extremities; severe large muscle spasms may require too high a dose to be safe. Severe spasms also may be managed by a surgical procedure that involves cutting nerves or tendons to decrease the contraction of specific muscles that are producing stiffness.
A better approach to the management of severe spasticity involves the use of a pump that delivers baclofen directly into the spinal canal. A tube is placed in the canal and then connected (beneath the skin) to a pump implanted in the abdominal region. The pump contains baclofen, which is delivered into the spinal canal at prescribed levels. Computer via radio waves may program the pump so that the dose may be changed as needed.
For some patients this technique may provide relief for intractable spasticity. Because the baclofen is delivered directly into the spinal canal and the level in blood and tissues remains low, side effects also are very low, and there almost always is a significant decrease in fatigue and malaise. This treatment is aggressive and expensive and should be reserved for those with severe spasticity that cannot be adequately managed by oral medications.
For those who have severe intractable spasticity, the kind that causes problems with all functions and is not responsive to exercise or medication, a spasticity-decreasing procedure may be necessary.
Nerves that control specific muscles of the leg may be destroyed with phenol, a chemical that is injected into the muscle. This is called a motor point block. It is used only for the most severe spasms that do not respond to drug therapy. It may produce flaccidity in the muscles, a profound looseness that is the opposite of spasticity. This relaxation may be more comfortable, but it usually does not increase functional mobility. It becomes progressively more difficult to repeat this procedure because of technical problems.
References
- Lublin FD, Reingold SC (1996) Defining the clinical course of multiple sclerosis: results of an international survey. National Multiple Sclerosis Society (USA) Advisory Committee on Clinical Trials of New Agents in Multiple Sclerosis. Neurology 46(4): 907-911.
- Minderhoud JM, van der Hoeven JH, Prange AJ (1988) Course and prognosis of chronic progressive multiple sclerosis. Results of an epidemiological study. Acta Neurol Scand 78(1): 10-15.
- Weinshenker BG, Bass B, Rice GP, Noseworthy J, Carriere W, et al. (1989) The natural history of multiple sclerosis: a geographically based study. I. Clinical course and disability. Brain 112(Pt 1): 133-146.
- Runmarker B, Andersen O (1993) Prognostic factors in a multiple sclerosis incidence cohort with twenty-five years of follow-up. Brain 116(Pt 1): 117- 134.
- Thompson AJ, Polman CH, Miller DH, McDonald WI, Brochet B, et al. (1997) Primary progressive multiple sclerosis. Brain 120(6): 1085-1096.
- Trojano M, Avolio C, Manzari C, Calò A, De Robertis F, et al. (1995) Multivariate analysis of predictive factors of multiple sclerosis course with a validated method to assess clinical events. J Neurol Neurosurg Psychiatry 58(3): 300-306.
- McDonnell GV, Hawkins SA (1998) Clinical study of primary progressive multiple sclerosis in Northern Ireland, UK. J Neurol Neurosurg Psychiatry 64(4): 451-454.
- Poser CM, Paty DW, Scheinberg L, McDonald WI, Davis FA, et al. (1983) New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Ann Neurol 13(3): 227-231.
- Kurtzke JF (1983) Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33(11): 1444-1452.
- Goodkin DE (1996) Multiple sclerosis: clinical design for the future. Mult Scler 1(6): 393-399.
- Weinshenker BG, Bass B, Rice GPA, Noseworthy J, Carriere W, et al. (1989) The natural history of multiple sclerosis: A geographically based study. 2.Predictive value of the early clinical course. Brain 112: 1419-1428.
- Phadke JG (1990) Clinical aspects of multiple sclerosis in northeast Scotland with particular reference to its course and prognosis. Brain 113(Pt 6):1597-1628.
- Yazdchi M, Ghasemi Z, Moshayedi H, Rikhtegar R, Mostafayi S, et al. (2013) Comparing the efficacy of botulinum toxin with tizanidine in upper limb post stroke spasticity. Iran J Neurol 12(2): 47-50.
- Multiple Sclerosis Genetics Group (1998) Clinical demographics of multiplex families with multiple sclerosis. Ann Neurol 43(4): 530-534.
- Albright AL (1996) Intrathecal baclofen in palsy movement disorders. J Child Neurol 11(Suppl 1): S29-S35.
- Steenbeek D, Meester-Delver A, Becher JG, Lankhorst GJ (2005) The effect of botulinum toxin type A treatment of the lower extremity on the level of functional abilities in children with cerebral palsy: evaluation with goal attainment scaling. Clin Rehabil 19(3): 274-282.
- Revesz T, Kidd D, Thompson AJ, Barnaard RO, McDonald WI (1994) A comparison of the pathology of primary and secondary progressive multiple sclerosis. Brain 117(Pt 4): 759-765.
- Thompson AJ, Kermode AG, Wicks D, MacManus DG, Kendall BE, et al. (1991) Major differences in the dynamics of primary and secondary progressive multiple sclerosis. Ann Neurol 29(1): 53-62.
- Filippi M, Martinelli V, Locatelli T, Medaglini S, Poggi A, et al. (1990) Acute- and insidious-onset myelopathy of undetermined aetiology: contribution of paraclinical tests to the diagnosis of multiple sclerosis. J Neurol 237(3): 171-176.
- Najmi S (2015) Study of Prevalence of Martin-Gruber Anomaly in Patients with Carpal Tunnel Syndrome. Int J Chronic Dis Ther 1(2): 5-8.
- Najmi S, Pourabolghasem S (2015) Restless Legs Syndrome. Int J Chronic Dis Ther 1(1): 1-4.





