Craving and Food Choices in Patients Under Treatment for Smoking Cessation
Aline Silva de Aguiar Nemer2*, Marcela Melquíades de Melo1, Sheila Cristina Potente Dutra Luquetti2, Ana Lúcia de Almeida Vargas1, Gláucia Renata Sousa Rodrigues1, Maria Alvim Leite2, Maíra Barros Louro2
1 Universidade Federal de Juiz de Fora, Hospital Universitario (HU/UFJF), Juiz de Fora, Minas Gerais, Brasil.
2* Departamento de Nutricao, Universidade Federal de Juiz de Fora (UFJF), Juiz de Fora, Minas Gerais, Brasil.
*Corresponding Author
line Silva de Aguiar Nemer,
Departamento de Nutricao, Universidade Federal de Juiz de Fora (UFJF),
Juiz de Fora, Minas Gerais, Brasil.
Tel: + 55 32 2102-3234.
E-mail: aline.nemer@ufjf.edu.br
Received: March 08, 2013; Accepted: April 12, 2013; Published: April 15, 2013
Citation: Aline Silva de Aguiar Nemer, et al. (2013), Craving and Food
Choices in Patients Under Treatment for Smoking Cessation. Int J Food Sci Nutr Diet. 2(3), 35-39. doi: dx.doi.org/10.19070/2326-3350-130007
Copyright: Aline Silva de Aguiar Nemer© 2013. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: The fissure, described as a strong desire to use the substance, and fear of weight gain affect the motivation of the individual to quit smoking.
Aims: The aim of this study was to evaluate the influence of abstinence and craving in food choices and nutritional status (NS) of patients after
one month of treatment for smoking cessation.
Methods: Longitudinal study where we applied questionnaires to asses craving, dependence, alcohol consumption and food intake to decrease
craving. The NS was assessed by BMI, waist circumference (WC) and abdominal circumference (AC). Evaluations were performed at baseline
and after one month of treatment.
Results: Among 23 participants who started treatment, 17 completed one month follow-up with 41.2% (n = 7) abstinent. After a month of treatment, the craving was lower among those abstinent compared to smokers. The most consumed foods to reduce the craving were, firstly, fruits followed by coffee, water and candies. Most subjects presented overweight (mean BMI 27.9 ± 6.9 kg/m²), and increased cardiovascular risk (WC: 89.0 ± 14.2; AC: 96.4 ± 15.0). After one month of monitoring, these parameters have not changed significantly. Reducing cravings and maintenance anthropometric parameters are aspects that can positively influence in the treatment success.
Conclusion: Smokers in treatment for one month for smoking cessation showed a decrease in nicotine craving. Abstinence did not change the
anthropometric parameters. The fruits were the most consumed foods to reduce the craving.
2.Introduction
3.Material and Methods
3.1.Statistical analysis
4.Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.References
Keywords
Smoking; Dependency; Food; Nutritional Status; Tobacco Use Cessation.
Introduction
Craving, described as a strong desire to use the substance, is the factors that influences the maintenance of smoking and may interfere with lapses and relapses [1,2].
Nicotine acts stimulating the liberation of neurotransmitters such as serotonin (5-HT) and dopamine (DA), important for food intake regulation [3]. The decrease in levels or changes in the signaling of 5-HT receptors are associated with the increased desire for sweets and carbohydrates [4]. These foods contribute to the increase in brain levels of tryptophan and also for the synthesis and liberation of the neurotransmitter serotonin, improving mood and irritability [5]. The same neurotransmitters, neuromodulators, neuropeptides and hormones that regulate the sensitivity to the reward of the drug at the brain also controls food intake and body weight [6].
Smokers have lower body mass index than non-smokers. Moreover, the smoking abstinence causes increase in body weight, resulting in a gain of approximately 5-6 kg [7]. The mechanism of weight gain after smoking cessation include decreased in basal metabolic rate, decreased activity of lipoprotein lipase enzyme and improves the taste and smell and increased appetite, contributing to changes in eating habits [7-9].
In this context, the study hypothesis is that during the process of smoking cessation, there is a higher consumption of foods, particularly with highest caloric density and low nutritional value to compensate the cigarette craving. This behavior can promote significant changes at the nutritional state and at the health of smokers in treatment. The aim of this study was to evaluate the influence of abstinence and craving in food choices and nutritional status of patients under treatment for smoking cessation.
Material and Methods
The study was a longitudinal analysis of 23 patients on treatment for smoking cessation at a public hospital in Minas Gerais, Brazil (University Hospital/ Juiz de Fora Federal University, HU/UFJF). The study was conducted between September and November 2011 and was approved by the committee of ethics in research with humans of the University Hospital from UFJF, Minas Gerais State, Brazil (Official no. 0067.180.420-11).
The smokers were evaluated at baseline and after 1month of treatment to smoking cessation, period that includes the first phase of treatment with structured group sessions [10].
Smokers of both sexes were evaluated, older than 18 years, with educational support for reading, understanding, providing answers to the questionnaires and provided a written informed consent. Patients with severe psychiatric and diseases that interfere with dietary intake and nutritional status (infectious, kidney, cardiac, endocrine or liver diseases) were excluded. In the first day of follow-up, clinical history, and anthropometric measurements were assessed by trained professionals. Was used the Fagerström Nicotine Dependence Test (FNDT) to measure the degree of nicotine dependenc [11,12].
Anthropometric nutritional assessment was performed at the beginning of the and after 1 month of treatment. Body weight (BW), height, waist circumference (WC) and abdominal circumference (AC) were measured in private rooms and with standardized protocols [13].
To assess the nutritional status, Body Mass Index (BMI) was calculated by the formula: BMI = weight (kg) / height (m2). Classification was performed as proposed by World Health Organization13, for adults, or Lipschitz (1994) [14], for the elderly patients.
The interpretation of the results of WC followed the cutoffs WC ≥ 90 cm for men and WC ≥ 80cm for women, indicating risk of cardiovascular disease measures that exceeded these values. At the end of each session the participants answered the Questionnaire of Smoking Urges-Brief - Brazil Version (QSU-Brief) [15].
Participants also completed a questionnaire to evaluate the choice of some foods to hold the cigarette craving (sweets, chocolates, sweet an salty biscuits, fruits, vegetables, soft drinks, water, coffee and diet candies and chewing gum) attributing a score from 0 to 7 for a sense of well-being after consuming the food or drink.
Statistical analysis was performed in SPSS software 12.0. P < 0.05 was considered statistically significant. Wilcoxon test was used to examine the difference between initial and final mean of QSU-Brief. To compare the difference of the final QSU-Brief of abstinent and smokers and initial and final anthropometric parameters it was used the Mann Whitney U test. The initial and final variables refer to the first and last week of follow-up (after 1 month of treatment).
Results
Participants were initially 23 volunteers with a mean age of 45.4 ± 13.0 years, mostly female (65.2%). Patients smoked a mean of 21.8 ± 14.6 cigarettes perday and mean duration of regular use of cigarettes was 26 ± 12.2 years. Following the FNDT classification, the high degree of dependence was more frequent among men (n = 6, 75%). At baseline, the nicotine craving ranged from moderate to severe in most men (75%), as well as most of the women (86.7%) (Table 1).
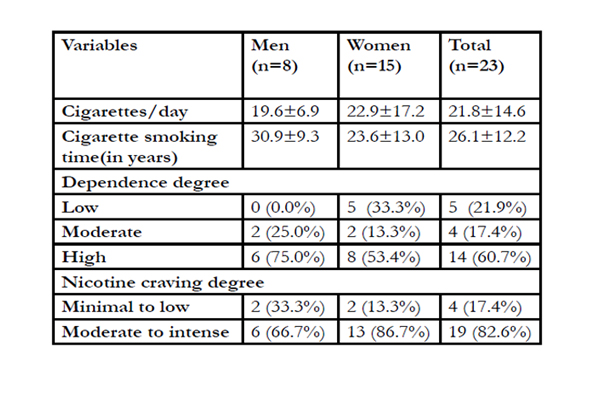

Table 1: Baseline characteristics of smokers (n=23)
About food consumption to reduce the craving to smoke, 30% (n=7) of patients reported eating something. The most frequently cited foods were water (n=4) and candies (n=2) (Figure 1).
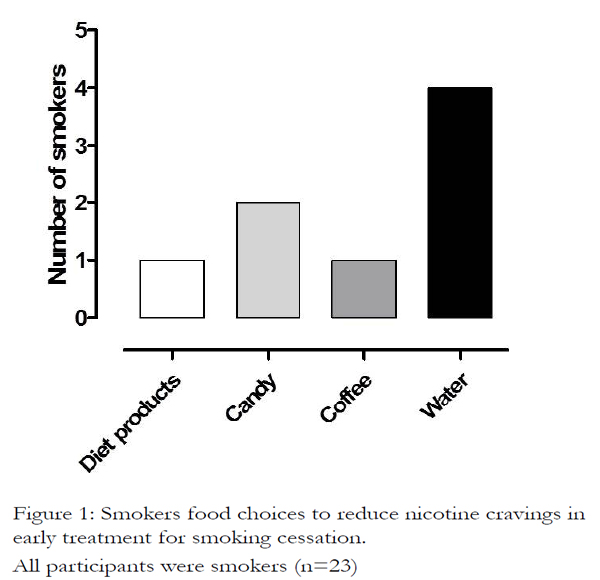
Figure 1. Smokers food choices to reduce nicotine cravings in early treatment for smoking cessation. All participants were smokers (n=23)
Of the 23 participants who started treatment, 17 completed follow-up for one month, and 41.2% (n = 7) reported being abstinent, with a mean of 9 days without smoking. Among patients who continued to smoke (n = 10, 58.8%), the mean number of cigarettes decreased to the 16/ day, which represents a reduction of 26.7% compared with the mean of the number of cigarettes reported initially.
For most patients (74.0%, n = 17) was prescribed some medication to help in the cessation process. Among those, 76.5% (n = 13) used NRT and 23.5% (n = 4)the bupropion.
After a month of treatment, the craving decreased among participants. However, the craving was lower among abstinent individuals compared to smokers (Figure 2).
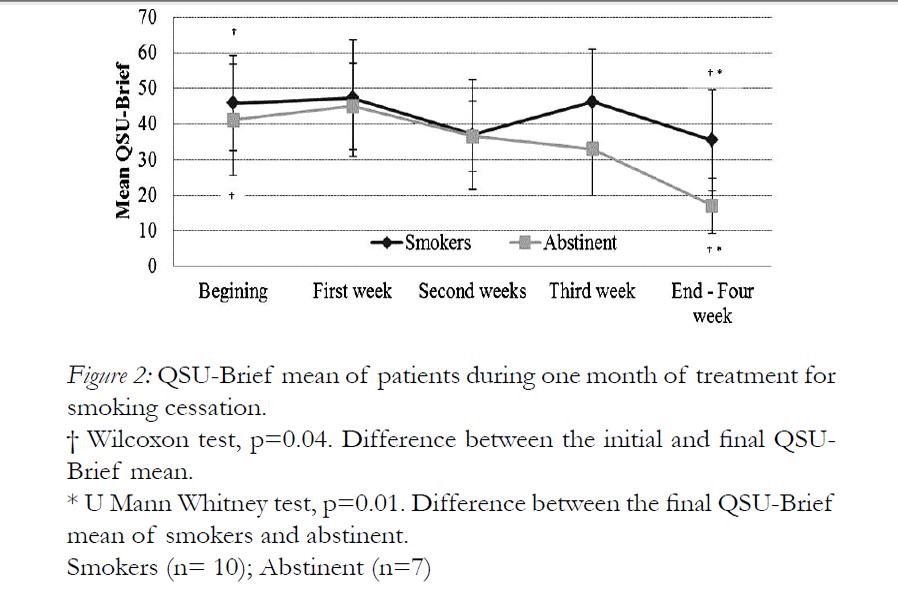
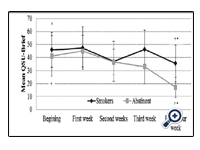
Figure 2: QSU-Brief mean of patients during one month of treatment for smoking cessation.
† Wilcoxon test, p=0.04. Difference between the initial and final QSUBrief mean.
* U Mann Whitney test, p=0.01. Difference between the final QSU-Brief mean of smokers and abstinent.Smokers (n= 10); Abstinent (n=7)
Most abstinent (n = 5) reported consuming foods to reduce the craving to smoke. Among smokers, the opposite was observed, the majority reported no consumption of food to control the craving (n= 6; 75%). Abstinent (n=5, 55.6%) and some smokers (n=4; 66.6%) related to eat fruits at the end of treatment for craving control. The foods most frequently cited by abstinents were fruits, followed by coffee and candies, which were reported as the food that has generated a greater sense of wellbeing (Figure 3).
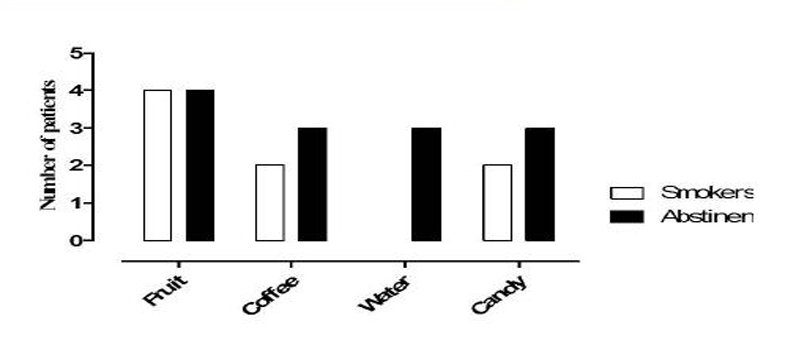
Figure 3: Food choices to reduce nicotine craving at the end of treatment (1 month follow-up) for smoking cessation. Smokers (n= 10); Abstinent (n=7)
Regarding anthropometric parameters at the beginning of treatment for smoking cessation, most individuals presented overweight and increased cardiovascular risk. Although smokers still have higher measures than the abstinent after one month of treatment, no significant changes between groups in such anthropometric variables was detected (Table 2).
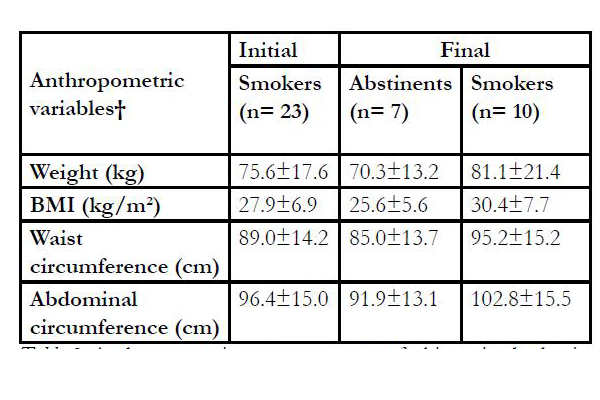
Table 2: Anthropometric measurements of sbjects in the beginning and after 1mo of follow-up for smoking cessation
* Comparison between groups was not significant (p>0.05).
†Values are presented as mean±SD
Discussion
In this study, over a third of patients (41.1%) who completed one month of treatment achieved smoking abstinence. There was a decrease in nicotine craving and changes in food choices, without changes in anthropometric parameters. These results do not support our initial hypothesis. The patients chose, principally, the fruit to contain the smoking craving. This may have reflected in the no anthropometric change after one month of treatment.
The abstinence rate in the present study was similar to that found by Costa et al (2006) [16]. However, in evaluation after one year follow up the authors identified a reduction from 43% to 17% of abstinence maintenance. Dawkins et al (2009) [17] described that 31% of patients were in abstinence after 3 months of treatment. According to Guerra (2004) [18], relapses happen mainly during the first 12 months of cessation, with rates ranging from 70 to 80% of smokers. Therefore, probably the number of abstinent of this study will be reduced especially in the first year of abstinence. One of the limitations of this study was to have only the patient report to be abstinent, information that was not confirmed by validation by measurement of expired carbon monoxide.
The standard treatment for this study followed the protocol proposed by INCA (2012) [10], which is structured in four weekly group sessions in the first month of treatment for smoking cessation.
It was observed that most patients (75.9%, n = 17) adhered to the treatment and concluded one month under attendance. Costa et al (2006) [16] conducted an intervention consisting of individual and group psychotherapy,besides medician, nutritionist and physical trainer appointments. Just like this study models, the groups meetings in the study by Costa et al (2006) had weekly adherence rate of 74% after three months of treatment [16].
In addition to participating in structured sessions, most patients needed to use NRT to assist in the smoking cessation. Studies show that NRT reduces tobacco withdrawal symptoms [19,20]. The craving may too be held by different physiological pathways, and only selected components of cigarette craving are influenced by NRT [21]. In this study, after one month of treatment, smokers and abstinent showed a craving reduction and this result was more intense among those who managed to abstain. Due to the small number of participants in this study, we cannot identify the influence of pharmacological treatment in changing the craving. We have no news about studies relating food choices during pharmacological treatment for smoking cessation.
Smokers who started treatment for smoking cessation was with overweight and risk profile for metabolic disorders, as evidenced by anthropometric measurements. Studies put smoking as a risk factor for major diseases such as obesity and cardiovascular disease [22]. Although at the end of a month of treatment, this risk profile has not changed in both the abstinent and not abstinent. Although the weight gain is commonly observed in the process of smoking abstinence [23], in this study body weight gain and an increase in abdominal fat were not observed. The role of the nutritionist at the ambulatory, the short time for the revaluation and the mean period of nine days of abstinence may have influenced the maintenance of nutritional status of participants.
Decreased craving appears as a favorable aspect to the maintenance of abstinence. Smoking cessation is a complex process that requires intense involvement of the patient. Reducing cravings and maintenance anthropometric parameters are aspects that can positively influence in the treatment success.
Changes in food choices, checked at the end of the study, may have helped in weight control, because most individuals have chosen mainly fruits to help control craving. The neurobiology of smoking and food consumption involves the dopaminergic and serotonergic systems [4]. However, the feeling of well-being was higher after consumption of candies, which can be in part explained by the fact that these foods contribute to the synthesis and release of serotonin, a neurotransmitter related to mood. The sugars present in fruits may increase dopamine levels and to reduce the tobacco craving, controlling the nicotine dependence [24].
Recent study showed that consumption of fruit and vegetables was inversely associated with indicators of nicotine dependence and predicted abstinence at follow- up among baseline cigarette smokers. Higher fruit and vegetable consumption was associated with fewer cigarettes smoked per day, longer time to first cigarette, and lower nicotine dependence score [24]. Thus, it can be suggested that higher consumption of fruits observed after one month of treatment, can contribute not only to control the weight but also to reduce the fissure and maintaining abstinence. In our study did not evaluate the amount of fruit consumed to assess whether there are differences between the abstinent and non.
Regular consumption of fruits helps in maintaining body weight due to its low caloric density and its high fiber content, which assists in bowel function, reduces levels of postprandial blood glucose and increase satiety, which helps in the weight loss and control [25].
Furthermore, among patients in abstinence was verified a higher consumption of water to help control cravings, another important aspect that may have contributed to weight control of individuals. Water contains no calories and helps to eliminate cigarette toxic substances.
Discussions about food choices among dependents were limited due to scarcity of studies. It was identified only one study that assessed the influence of craving on food choice and in body weight change among alcohol-dependent patients in treatment [26]. It becomes clear the importance of further studies to understand the food consumption during withdrawal and smoking cessation.
In this study, group sessions had the constant presence of the nutritionist may have contributed to the best food choices from patients. In another study with smokers in treatment for smoking cessation, the role of nutritionist resulted in healthier eating habits in 41% of the participants [16]. These results reinforce the importance of nutritionist in treatment strategy,contributing to the prevention of excessive weight gain and thus preventing relapses.
Conclusion
Smokers under for smoking cessation presented nicotine craving remission, in addition to changes in alimentary choices, with special increment of fruits consumption to hold nicotine cravings. This fact may have influenced the maintenance of anthropometric parameters after one month of treatment. The major consumption of high carbohydrates rate and low nutritional quality foods was not detected, however, these foods were mentioned by some patients as those which most caused welfare.
Acknowledgements
To staffs of the Prevention, Treatment and Tobacco Control Ambulatory and Multidisciplinary Program for Residence in Adult Health (HU/UFJF). Thanks to PROPESQ/UFJF and CNPq for the financial support (Process 471642/2011-8).
References
- Beck AT, Wrigth FD, Newman CF, Liese BS. Cognitive therapy of substance abuse. New York: Gulford Press; 1993.
- Marques AC, Seibel SD. O craving. In: Seibel SD, Toscano JR. Dependência de drogas. São Paulo: Atheneu; 2001. p. 239-48.
- Jo YH, Talmage DA, Role LW. Nicotinic receptor-mediated effects on appetite and food intake. J Neurobiol. 2002;53:618-32.
- Feijó FM, Bertoluci MC, Reis. Serotonina e controle hipotalâmico da fome: uma revisão. Rev Assoc Med Bras. 2011;57(1): 74-77.
- Wurtman RJ, Wurtman J.J. Brain serotonin, carbohydrate-craving, obesity and depression. Obes Res. 1995;3(4):477-80.
- Volkow ND, Wise RA. How can drug addiction help us understand obesity? Nature Neurosc. 2005;8(5):555-60.
- Chatkin R, Chatkin JM. Tabagismo e variação ponderal: a fisiopatologia e genética podem explicar esta associação? J Bras Pneumologia.2007;33(6):712-19.
- Filozof C, Fernández Pinilla MC, Fernández-Cruz, A. Smokingcessation and weight gain. Obes Rev. 2004;5(2):95-103.
- Saules KK, Pomerleau CS, Snedecor SM, Brouwer RN, RosenbergEEM. Effects of disordered eating and obesity on weight, cravingand food intake during and ad libitum smoking and abstinence. Eat Behav.2004;5:353-363.
- Instituto Nacional do Câncer (INCA). Plano de Implantaçãoda Abordagem e Tratamento do Tabagismo na Rede SUS Portaria GM/ MS 1.035/04 Portaria SAS/MS 442/04. Fluxos de Informação e Instrumentosde Avaliação Manual de Operação. Available from: http://www.inca.gov.br/tabagismo/publicacoes/plano_abordagem_sus.pdf.>.
- Heartherton TF, Kozlowski LT, Frecker RC, Fagerstrom, KO.The Fargerstrom Test for Nicotine Dependence: a revision of the FargerstromTolerance Questionnaire. Br J Addiction. 1991;86:1119 – 127.
- Halty LS, Huttner MD, Oliveira Netto IC, Santos VA, MartinsG. Análise da utilização do Questionário de Tolerância de Fagerström(QTF) como instrumento de medida da dependência nicotínica. J Pneumology.2002;28(4):180-86.
- World Health Organization. Obesity. Presenting and managingthe global epidemic. Report of a WHO consultation on obesity. Genebra; 1998.
- Lipschitz DA. Screening for nutritional status in the elderly. Primary Care. 1994;21(1): 55-67.
- Araújo RB, Oliveira MS, Moraes JFD, Pedroso RS, Port F, CastroMGT. Validação da versão brasileira do Questionnaire of SmokingUrges-Brief. Rev Psiq Clin. 2007;34(4):166-75.
- Costa AA, Elabras Filho J, Araújo ML, Ferreira JES, MeirellesLR, Magalhães CK. Programa Multiprofissional de Controle do Tabagismo:aspectos relacionados à abstinência de longo prazo. Rev SOCERJ.2006; 19(5):397-403.
- Dawkins L, Powell JH, Pickering A, Powell J, West R. Patternsof change in withdrawal symptoms, desire to smoke, reward motivationand response inhibition across 3 months of smoking abstinence. Addiction.2009;104:850–58.
- Guerra MP. A abstenção tabágica: reflexões sobre a recaída.Aná Psicológica. 2004;3(22):507-18.
- Leischow SJ, Valente SN, Hill AL, Otte PS, Aickin, M, Holden,T, Kligman E, Cook G. Effects of nicotine dose and administrationmethod on withdrawal symptoms and side effects during short-termsmoking abstinence. Exp Clin Psychopharmacol. 1997;5:54–64.
- Jones TE, Williams J. Craving control using nicotine replacementtherapy in a teaching hospital. Int Med J. 2012;42(3):317-22.
- Teneggi V, Tiffany ST, Squassante L, Milleri S, Ziviani L, ByeA. (2002). Smokers deprived of cigarettes for 72 h: Effect of nicotinepatches on craving and withdrawal. Psychopharmacol. 2002; 164:177-87.
- Balhara YPS. Tabacco and metabolic syndrome. Indian J EndocrinolMetab. 2012; 16(1): 81–87.
- Nerín I, Assunción B, Gargallo P, Jiménez-Muro A, MarquetaA. Weight gain and anxiety levels in recent ex-smokers. Arch Bronconeumol.2007;43(1):9-15.
- Haibach JP, Homish GG, Giovino GA. A longitudinal evaluationof fruit and vegetable consumption and cigarette smoking. NicotineTob Res. 2012; Jul 5; [Epub ahead of print]. doi: 10.1093/ntr/nts130
- Hall SM, Tunstall C.D, Vila KL, Duffy JB. Weight gain preventionand smoking cessation: Cautionary Findings. Am J Pub Health.1992;82(6):799-803.
- Toffolo MCF, Pereira IS, Silva KAL, Marliére CA, NemerASA. Escolha de alimentos durante a abstinência alcoólica: influência nafissura e no peso corporal. J Bras Psiquiatr. 2011;60(4):341-46.





