Prevalence of HPV in Oesophageal Biopsies and its Correlation with Expression Of P16INK4A
Misra V1*, Singh A1, Misra SP2, Dwivedi M2, Verma K1, Dhingra V1, Trivedi P1
1 Department of Pathology, Moti Lal Nehru Medical College, Allahabad, UP, India.
2 Department of Gastroenterology, Moti Lal Nehru Medical College, Allahabad, UP, India.
*Corresponding Author
Dr. Vatsala Misra M.D., F.I.C. Path, M.A.M.S., M.N.A.Sc.,,
Professor, Department of Pathology, Moti Lal Nehru Medical College,
Allahabad, UP, India.
Tel. : +91 9415214308
E-mail: drvatsalamisra@gmail.com
Received: August 29, 2016; Accepted: September 26, 2016; Published: September 29, 2016
Citation: Misra V, Singh A, Misra SP, Dwivedi M, Verma K, et al., (2016) Prevalence of HPV in Oesophageal Biopsies and its Correlation with Expression Of P16INK4A. Int J Virol Stud Res. 4(4), 48-54.dx.doi.org/10.19070/2330-0027-160008
Copyright: Vatsala Misra© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The association of Human papillomavirus (HPV ) and P16INK4A is well established with cervical malignancies and has been studied in oral mucosa also. Koilocytosis, that is considered to be a hallmark of HPV infection is also seen in oesophageal mucosa.
Aims: This study was designed to determine the prevalence of HPV in biopsies from inflammatory and neoplastic lesions of oesophagus and correlate it with expression of P16INK4A. Materials and Methods: The study included 102 oesophageal biopsies. Haematoxylin & Eosin stained sections were examined for morphological details including koilocytosis. Immunohistochemistry for HPV and P16INK4A were done on 50 biopsies. HPV positivity was graded and scoring for P16INK4A was done.
Results: Various grades of koilocytosis was noted in 68.75%, 94.73% and 72.91% controls, inflammatory and neoplastic lesions respectively. IHC for HPV was positive in 80% control, 75% inflammatory and 100% cases of neoplastic lesion. Complete score for P16INK4A was 0.60, 0.59 and 3.63 in control, inflammatory and neoplastic lesion. The difference in expression of P16INK4A between neoplastic and inflammatory lesion was statistically significant.
Conclusion: Expression of P16INK4A protein showed good correlation with HPV infection in inflammatory and neoplastic lesions. Thus IHC for P16INK4A which is easily available can be used as an indirect evidence of HPV infection in neoplastic lesion where expensive molecular technique for HPV DNA measurement is not feasible.
2.Introduction
3.Materials and Methods
3.1 Results
4.Results
4.1 Control
4.2 Patients
5.Discussion
6.Conclusion
7.References
Keywords
Oesophageal Squamous Cell Carcinoma; Oesophagus; Koilocytosis.
Introduction
Cancer of the oesophagus is currently the eighth most common human cancer and the sixth most common cause of cancer-related death [1]. Globally, squamous cell carcinoma (SCC) is the most common subtype of oesophageal cancer [2]. Human OSCC is believed to develop through a multi-step process. Understanding of the molecular mechanisms in this process will not only provide biomarkers for early detection, but also enable us to improve treatment modalities. The role of HPV in the etiology of OSCC has been debated for the past 30 years.
Human papillomavirus (HPV) are small encapsulated, non-enveloped double stranded DNA viruses classified as belonging to the Papovaridae family, and more than 70 papillomavirus types have been identified on the basis of sequence divergence. The association of human papillomavirus (HPV) infections and squamous cell precancer lesions of the uterine cervix has been established since the late 1970s. The squamous cell lining of the oral mucosa is in direct continuity with the oesophagus, and the first descriptions on HPV lesions in the oral mucosa were slightly preceded by
reports suggesting that this virus might be involved in the development of both benign and malignant squamous cell lesions of the oesophagus also. A long-recognized, pathognomonic feature of human papillomavirus (HPV) infection is the appearance of halo or koilocytotic cells in the differentiated layers of the squamous epithelium.
The p16 protein (p16) is a Cyclin-dependent kinase inhibitor 2A, (CDKN2A, p16INKa) also known as multiple tumor suppressor 1 (MTS-1), a tumor suppressor protein, that in humans is encoded by the CDKN2A gene [3]. The p16 tumor suppressor gene, located on chromosome 9p21, is a member of the INK4 class of cell-cycle inhibitors that includes p15INK4a, p18INK4C, and p19INKd. The binding of the p16 tumor suppressor gene product with the cyclin-dependent kinases 4 and 6 blocks its interaction with the D-type cyclins, maintains the retinoblastoma (Rb) gene in its hypophosphorylated state that binds the E2F transcription factor, and, in turn, prevents cell-cycle progression [4]. Overexpression of p16 has been demonstrated to be strongly related to the presence of HPV16, 18 [5]. Overexpression of p16 in cervical cancers is believed to be due to the inactivation of Rb by the HPV E7 oncoprotein [6]. Homozygous deletion of p16 are frequently found in oesophageal cancer and gastric cancer cell lines [7].
HPV is considered to be a recognized agent for having potential in carcinoma cervix. The association of HPV infection with oesophageal cancer in India has been studied by some authors but no well documented data is there [8-10]. Some studies have shown lack of significant association between the high risk HPV 16 and 18 and oesophageal carcinoma and suggest further research [11-13].
As correlation between HPV and oesophageal carcinoma has shown variable results, therefore the present study was undertaken to do immunohistochemistry for Human papilloma virus and P16INK4A in oesophageal biopsies in various groups and to correlate the prevalence of HPV with expression of P16INK4A antigen.
Materials and Methods
The study was conducted on 102 oesophageal biopsies. Out of these, 31 prospective biopsies were from patients presenting with inflammatory and neoplastic lesion of oesophagus and 16 biopsies were taken as control from patients who did not have any oesophageal lesions but underwent upper GI endoscopy for gastric or duodenal lesion. Remaining 55 biopsies were collected retrospectively from the records of department of pathology. This study has been performed in accordance with the ethical standards after taking approval of institutional ethical committee. Three to four micron thick sections were cut and stained with Haematoxylin & Eosin (H&E) stain for histopathological details. H&E stained sections were examined thoroughly to note the histopathological details. Sections were grouped in Normal, Inflammatory and Neoplastic group based on histopathological features. Koilocytes were counted by pin hole method, randomly in ten high power fields moving from a field with highest no. of koilocytes towards field with lowest no. of koilocytes and percentage was calculated. Accordingly they were graded as: - Negative<1%, traces =1-10%, mild =11-30%, moderate =31-60%, severe =>60%. (Figure 1)
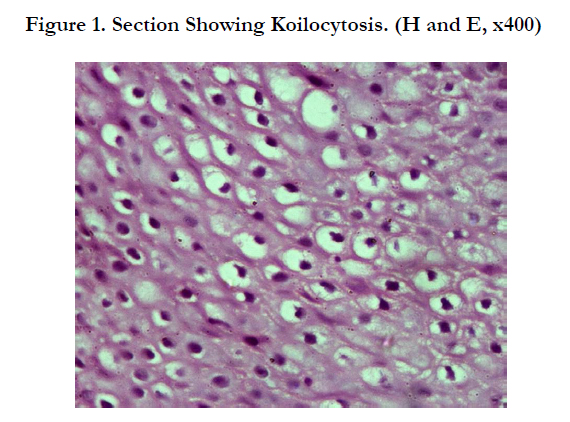
Figure 1. Section Showing Koilocytosis. (H and E, x400)
IHC for HPV and P16INK4A could only be performed on 50 cases out of 102 cases that had evidence of koilocytosis on histological examination due to technical and financial reasons. Immunohistochemistry was done for HPV localization and expression of P16INK4A as follows-Five micron thick sections were cut from paraffin block and mounted on super frost slide. Sections were dewaxed, washed in alcohol and antigen retrieval carried out in microwave with EZ antigen retrieval solution-I (Biogenex, Fremont CA) for 15 minutes. Endogenous peroxidase was blocked by using 0.3% hydrogen peroxide in distilled water at room temperature for 10 minutes. Slides were washed by PBS briefly and incubated with Mouse monoclonal primary antibody for 60 min. Slides were then extensively washed in PBS and incubated with secondary antibody for 20 min. Sections were washed with PBS and incubated with label (ABC) for 30 min. Sections were washed with PBS. Diaminobenzidine (DAB) was used as the chromogen in hydrogen peroxide for 10 min. Sections were then counterstained with haematoxylin and mounted.
A case was considered positive when brown colouration of the nucleus and/or cytoplasm was observed.Primary antibody used for HPV was Monoclonal Mouse Anti HPV clone K1H8 (DAKO Denmark). Anti HPV clone K1H8 reacts with a non-conformational internal linear epitope of a major capsid protein of HPV-1 which is broadly expressed among different HPV subtypes. The antibody was diluted 1:50 with PBS. Cells showing positive expression for HPV antigen on IHC in the form of brown colouration of nucleus were counted randomly in 10 high power fields by pin hole method and then percentage was calculated against the total number of nuclei recorded. Accordingly, they were graded as: - Negative<1%, traces =1-10%, mild =11-30%, moderate =31-60%, severe =>60%. (Figure 2)
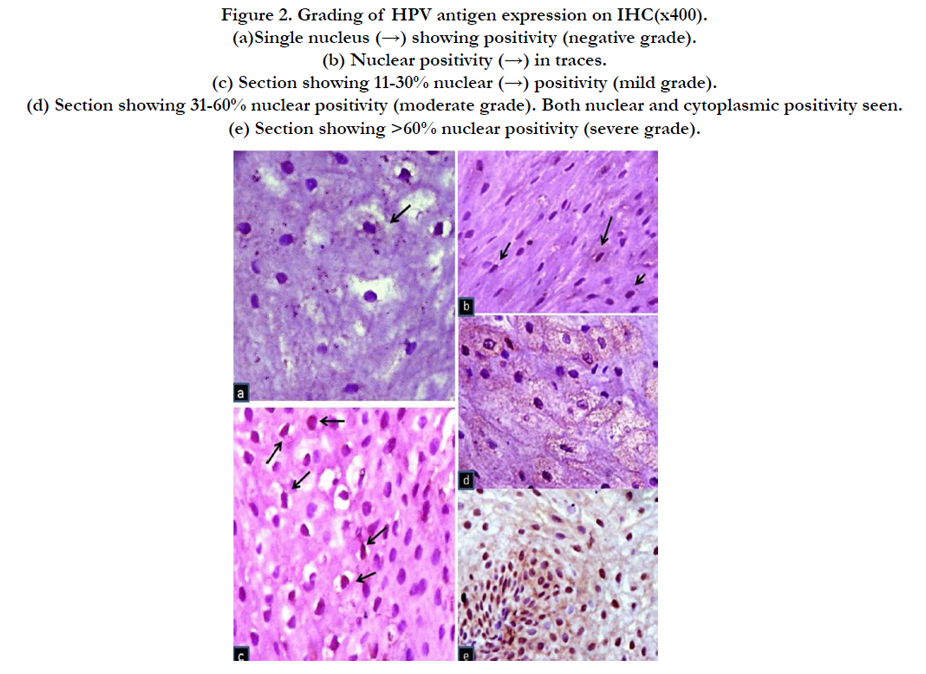
Figure 2. Grading of HPV antigen expression on IHC(x400).
(a)Single nucleus (→) showing positivity (negative grade).
(b) Nuclear positivity (→) in traces.
(c) Section showing 11-30% nuclear (→) positivity (mild grade).
(d) Section showing 31-60% nuclear positivity (moderate grade). Both nuclear and cytoplasmic positivity seen.
(e) Section showing >60% nuclear positivity (severe grade).
Primary antibody used for P16INK4A was Anti P16INK4A clone G175- 405 (BioGenex, Fremont CA). A case of uterine cervix squamous cell carcinoma was used as a positive control.The scoring criteria for P16INK4A immunoreactivity (P16INK4A expression) were based on previous scoring method used by Sargolzaei et al(2014) [14]. Expression score (ES) was given as: 0- <5% cells positive, 1- <20% cells positive and 2- >20% cells positive. The staining intensity was compared with the positive control slide and graded as Intensity score (IS):1for weak, 2 for moderate and 3 for severe staining. Localization score (LS) were noted as 1 for nuclear or cytoplasmic positivity and 2 for both. Finally a Complete score (CS) was calculated using the formula: CS=ESxISxLS. Mean (S.D.) of CS was calculated for various lesions. (Figure 3)
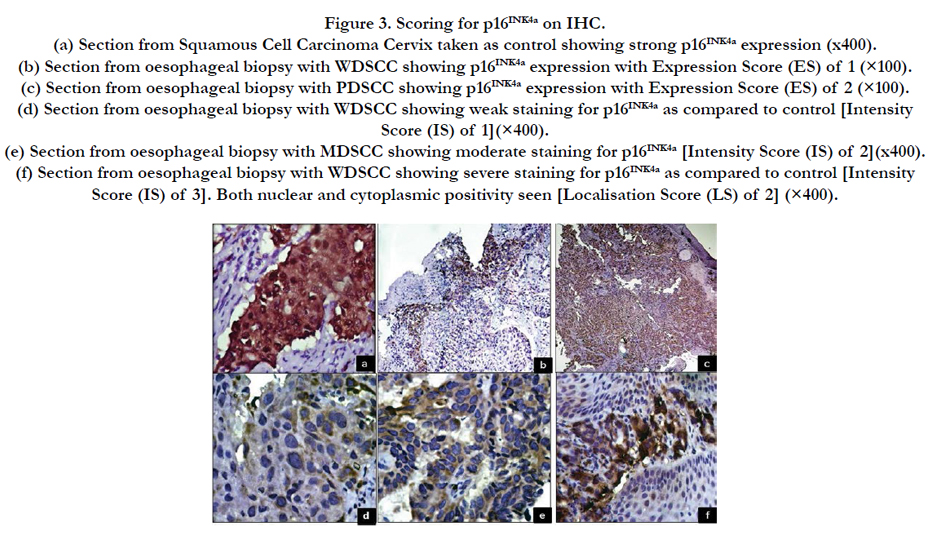

Figure 3. Scoring for P16INK4A on IHC.
(a) Section from Squamous Cell Carcinoma Cervix taken as control showing strong P16INK4A expression (x400).
(b) Section from oesophageal biopsy with WDSCC showing P16INK4A expression with Expression Score (ES) of 1 (×100).
(c) Section from oesophageal biopsy with PDSCC showing P16INK4A expression with Expression Score (ES) of 2 (×100).
(d) Section from oesophageal biopsy with WDSCC showing weak staining for P16INK4A as compared to control [Intensity
Score (IS) of 1](×400).
(e) Section from oesophageal biopsy with MDSCC showing moderate staining for P16INK4A [Intensity Score (IS) of 2](x400).
(f) Section from oesophageal biopsy with WDSCC showing severe staining for P16INK4A as compared to control [Intensity
Score (IS) of 3]. Both nuclear and cytoplasmic positivity seen [Localisation Score (LS) of 2] (×400).
Data obtained from the analysis were finally transported to the excel sheet. Unpaired student‘t’ test and chi square test with and without Yates’ correction was used to compare various parameters. Sensitivity, specificity, positive predictive value and negative predictive value for koilocytosis and P16INK4A as an indicator for presence of HPV infection were also calculated taking positive HPV antigen expression on IHC as gold standard.
Results
Of 102 cases included in the study, 16 were from control group. Remaining 86 included inflammatory 38/86 (44.18%) and neoplastic 48/86 (55.81%) cases.
11/16 (68.75%) showed evidence of koilocytosis of varying grades. It was predominantly in traces (43.75%) and mild (18.75%) grade. IHC for HPV done for 5 controls showed 4 cases with evidence of HPV positivity out of which 3/5 (60%) were of mild grade. Similarly IHC for P16INK4A done in the 5 controls showed a mean CS (S.D.) of 0.60 (0.89).
Koilocytosis was noted in 36/38 (94.73%) inflammatory lesions. Out of that 18/38 (47.36%) and 13/38 (34.21%) showed mild and moderate grade koilocytosis respectively. The difference in the presence of koilocytes between normal group and inflammatory lesion was statistically significant (P<0.02). IHC for HPV was done in 8 inflammatory cases out of which 3/8 (37.5%) showed mild and 3/8(37.5%) showed moderate grade expression. Similarly IHC for P16INK4A done in 8 inflammatory casesshowed a mean CS (SD) of 0.59 (1.06).
Out of 48 neoplastic cases 39 cases were of OSCC and 9 cases had adenocarcinoma. Koilocytosis was observed in 35/48 (72.91%). Out of these 14/48 (29.16%) had mild grade and 12/48 (25.0%) of moderate grade koilocytosis. Koilocytosis was mostly associated with OSCC cases. On further grading of OSCC cases, 18 were well differentiated, 14 were moderately differentiated and 7 were poorly differentiated OSCC. The distribution of koilocytosis was seen to be mostly associated with well differentiated cases 13/18 (72.22%).
IHC for HPV was positive in all 36 neoplastic cases which included 31 cases of OSCC and 6 cases of adenocarcinoma. 21/36 (58.33%) neoplastic cases showed moderate grade of HPV antigen expression. Distribution of HPV in different grades of OSCC shows majority of positive cases in moderately differentiated OSCC13/30(43.33%), most of which are of moderate grade 6/13(46.15%).
P16INK4A expression was observed to be strongly associated with neoplastic cases. Mean (S.D) CS calculated in neoplastic lesion was 3.63(2.62). A greater range of variation was noted in neoplastic cases when compared with the inflammatory group and this difference was found to be statistically significant (P≤0.05).
However, among neoplastic lesions, we found a mean (S.D) CS of 3.45(2.63) in OSCC cases and 4.37(3.24) in Adenocarcinoma cases. On further sub grouping the OSCC cases into well, moderately and poorly differentiated forms, mean (S.D) CS of 1.95(1.15), 4.11(1.95) and 5.21(3.98) was recorded respectively.
On comparing HPV antigen expresion with koilocytosis, we found a slight variation in inflammatory group with 14% showing koilocytosis and 16% showing HPV antigen expression. However a great difference was noted in the neoplastic lesions, with 52% showing koilocytosis and 74% showing antigen expression.
Sensitivity, specificity, positive predictive value and negative predictive value of koilocytosis taking HPV antigen expression on IHC as gold standard was found to be 30.77%, 79.17%, 61.54% and 51.25% respectively.
On comparing the mean (S.D.) CS among the well differentiated OSCC cases with the poorly differentiated OSCC cases, a greater difference was observed and this difference was statistically significant (P ≤ 0.008).
Analysis of HPV antigen expression with P16INK4A reveals that majority of the neoplastic cases having moderate grade of HPV antigen expression showed a higher mean(S.D.) complete score .56.75% of neoplastic cases were observed to have a CS of 4.07(2.92).
Sensitivity, specificity, positive predictive value and negative predictive value of P16INK4A taking HPV antigen expression as gold standard was found to be 96.43%, 31.82% , 64.29% and 87.50% respectively
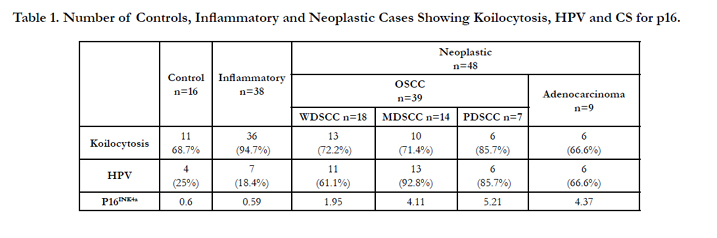

Table 1. Number of Controls, Inflammatory and Neoplastic Cases Showing Koilocytosis, HPV and CS for p16.
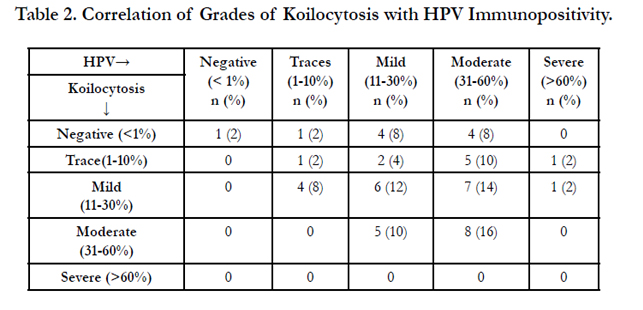
Table 2. Correlation of Grades of Koilocytosis with HPV Immunopositivity.
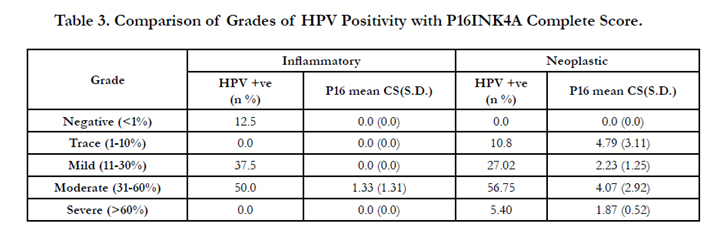
Table 3. Comparison of Grades of HPV Positivity with P16INK4A Complete Score.
Discussion
The role of HPV in squamous cell carcinoma of uterine cervix is well established since the late 1970 and substantial evidence has been provided during the past few years indicating an etiologic role of HPV infection in anogenital and upper aerodigestive lesions [15-18]. The etiological role of human papillomavirus (HPV) in oesophageal squamous cell carcinoma (OSCC) has been widely researched for more than three decades, with conflicting findings. HPV infection in the squamous cell lining induces koilocytosis formation. Diagnostically, the koilocyte is considered to be an excellent indicator of HPV infection [19]. In present study we have tried to correlate it with HPV detection by IHC.
The choice of a suitable method for detection of HPV DNA has become increasingly complex [16]. In 1986 Hille et al., were the first to use IHC for HPV antigen demonstration in oesophageal carcinoma [20]. Only10 % of their cases showed positivity for HPV antigen. Elizabeth et al., used IHC for HPV detection and p16 expression in 16 cases of HNSCC. They found 73% of cases positive for HR-HPV by PCR method. HPV detection by IHC was negative in all the samples but p16 strongly correlated with HR-HPV [21].
To confirm the presence of HPV in our study, detection of HPV capsid protein was done with the help of immunohistochemistry. Due to non-availability of tissue and some technical errors IHC could only be applied on 50 cases which were exhibiting koilocytosis too. Out of the 50 cases, 10% were from normal controls, 16% were from inflammatory and 74% were from neoplastic lesion. Total no. of cases that were positive for HPV were 98%, out of which 8.16% were from normal group, 16.32% were from inflammatory lesion and 75.51% were from neoplastic group.
No well documented study could be found with reference to any scoring method for the percentage of cells demonstrating positivity for HPV antigenic expression on IHC. In our study, we recorded the percentage of cells showing nuclear positivity for HPV antigen and the sections were graded into negative, traces, mild, moderate and severe grade. The grades of positivity were compared in normal, inflammatory and neoplastic group.
When the HPV antigen expression was compared with koilocytosis, 8% of normal control group showed koilocytosis and HPV positivity. A slight variation was observed in the inflammatory group showing 14 % with koilocytosis and 16% expressing HPV antigen. However, a marked variation was noted in neoplastic cases (52% showed koilocytosis and 74% showed HPV antigen expression). It was also observed that as we moved from well differentiated OSCC to poorly differentiated OSCC, the expression of koilocytosis decreased. Taking HPV antigen expression as gold standard, the sensitivity of koilocytosis was found to be 30.77%. It signifies that koilocytosis may be taken as indicator of HPV infection in inflammatory lesions but it is not uniformly seen in neoplastic lesion. This may be due to alteration in cell morphology, lack of differentiation and increased pleomorphism.
In the present study, detection of HPV by IHC was high as compared to some previous studies [26, 27]. This may probably be due to the low number of cases and inclusion of cases with evidence of koilocytosis on histology. Another factor was improvement in the technique used for antigen retrieval and the procedure of IHC.
The role of IHC in detecting HPV infection is more consistent for the inflammatory lesion as compared to neoplastic group. This was comparable with the study of Nakamura et al., They investigated the relation between squamous tumours of the conjunctiva and lacrimal sac and HPV infection in 17 cases [22]. 8 cases showed positive immunohistochemical staining with antibodies to HPV and koilocytosis was detected in 7 of these 8 cases. However they concluded that koilocytosis is a more reliable indicator of HPV infection in benign lesion as compared to neoplastic lesions. On the other hand IHC staining was superior to assessment of koilocytosis and in situ hybridization for detection of HPV infection in dysplastic lesions and carcinomas.
Changes in gene INK4a (p16) have been studied in several tumors such as squamous cell carcinoma of the head, neck and oesophagus, adenocarcinoma of the pancreas and gastrointestinal stromal tumors. HPV-positive tumors are characterized by high expression of p16 and p16 is widely considered a surrogate marker for HPV infection in the context of squamous cell carcinoma [23, 24].
In the present study, P16INK4A expression was recorded on the basis of scoring method used by Sargolzaei et al.,, [14] A detailed examination of the cells expressing P16INK4A was done. Expression score (ES), Intensity score (IS) and Localization score (LS) were noted and finally a complete score (CS) was calculated in all the cells positive for P16INK4A.
CS of 0.60 was recorded in normal group while 0.59 in inflammatory group where as neoplastic group showed a CS of 3.63 that was significantly high (P <0.00073) as compared to inflammatory group indicating that higher expression of p16 is a definite marker of neoplastic changes. Similar results were obtained by Busatto et al., [25]. On comparing malignant and normal tissues, they found neoplastic nuclei showed a higher percentage of immunoreaction for p16.However, results of Busatto et al., indicated that p16/ CDKN2 mutations occur infrequently in oesophageal squamous carcinoma [25].
A good association was found between HPV infection and expression of P16INK4A in earlier studies on OSCC by Ding et al who detected HPV 16 in 47% cases of OSCC by PCR method and 41% cases of OSCC showed positivity for P16INK4A [26]. In a study by Deng et al., HPV DNA was detected in 31.3 % samples but P16INK4A expression was seen in 26.7% HNSCC cases [27]. The sensitivity of P16INK4A staining for detection of HPV DNA in HNSCC was 61.7%, while the specificity was 89.3% for all HNSCC cases. In the present study, it was observed that the sensitivity of P16INK4A taking HPV as gold standard was 96.43% Our sensitivity results for P16INK4A correlated well with the study of Deng et al., [27]
Murthy et al conducted a study to correlate levels of p16 expression in different grades of Oral cancer [28]. They inferred that high p16 expression levels is associated with well differentiated oral SCC (low grade). However, there existed no significant difference in the expression range for the different grades of tumors. On contrary, Patil et al correlated the association of HPV in histological grades of Oral SCC using p16 (P16INK4A) immunohistochemistry (IHC) [29]. p16 positivity was noted in 26/30 (86.66%) oral SCC cases .Out of 26 oral SCC cases, p16 positivity was seen in 70% of WDOSCC, 90% of MDOSCC and, 100% PDOSCC.
Diffuse staining pattern was noted in PDOSCC, which in turn depicts the increase viral overload, which might have an influence on its aggressive behaviour.
Sargolzaei et al tried to correlate P16INK4A expression in different grades and stages of oral squamous cell carcinoma [14]. However, they found 33.3%, 31.6% and 33.3% of well differentiated, moderately differentiated and poorly differentiated oral SCC cases respectively were positive for P16INK4A, the difference was not statistically significant.
In present study CS was 1.95 for WDSCC while in MDSCC CS was 4.11 and in PDSCC CS was 5.21. Here a greater difference was noted between CS of WDSCC and PDSCC which was statistically significant (P<0.008). The difference between CS of WDSCC and MDSCC was also statistically significant (P<0.0014) but no significant difference was observed between CS of MDSCC and PDSCC.
Conclusion
To conclude, the prevalence of koilocytosis on H&E stained section is a good indicator of HPV infection in inflammatory lesions. However in neoplastic lesions, the sensitivity was found to be less, probably due to dedifferentiation of cells and lack of identification of koilocytosis.
Expression of P16INK4A protein showed good correlation with HPV infection in inflammatory and neoplastic lesions. The CS for expression of P16INK4A was maximum in MDSCC thus IHC for P16INK4A which is easily available can be used as an indirect evidence of HPV infection in neoplastic lesion where expensive molecular technique for HPV DNA measurement is not feasible.
References
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C et al., (2010) Estimates of worldwide burden of cancer in 2008. Int J Cancer. 127(12): 2893–2917.
- Parkin DM, Bray F, Ferlay J, Pisani P ( 2005) Global cancer statistics, 2002. CA Cancer J Clin. 55(2): 74–108.
- Nobori T, Miura K, Wu DJ, Lois A, Takabayashi K, et al., (1994) Deletions of the cyclin-dependent kinase-4 inhibitor gene in multiple human cancers. Nature. 368(6473): 753–756.
- Kim WY, Sharpless NE (2006) The regulation of INK4/ARF in cancer and aging. Cell. 127: 265–275.
- Frank König, Gisbert Krekeler, Johannes F Hönig, Carlos Cordon-Cardo, Gösta Fischer et al., (2007) Relation between Human Papillomavirus Positivity and p16 Expression in Head and Neck Carcinomas – A Tissue Microarray Study. Anticancer Res. 27(1): 283-288.
- Duensing S, Munger K (2002) The human papillomavirus type 16 e6 and e7 oncoproteins independently induce numerical and structural chromosome instability. Cancer Res. 62(23): 7075-7082.
- Igaki H, Sasaki H, Kishi T, Sakamoto H, Tachimori Y, et al., (1994) Highly frequent homozygous deletion of the p16 gene in esophageal cancer cell lines. Biochem Biophys Res Commun. 203 (2): 1090–1095.
- Agarwal SK, Chatterji A, Bhambhani S, Sharma BK (1998) Immunohistochemical co-expression of human papillomavirus type 16/18 transforming (E6) oncoprotein and p53 tumour suppressor gene proteins in oesophageal cancer. Indian J Exp Biol. 36(6): 559-563.
- Sobti RC, Kochar J, Singh K, Bhasin D, Capalash N (2001) Telomerase activation and incidence of HPV in human gastrointestinal tumors in North Indian population. Mol Cell Biochem. 217: 51-56.
- Katiyar S, Hedau S, Jain N, Kar P, Khuroo MS, et al., (2005) p53 gene mutation and human papillomavirus (HPV) infection in esophageal carcinoma from three different endemic geographic regions of India. Cancer Lett.218(1): 69-79.
- JS Koh, SS Lee, HJ Baek, YI Kim (2008) No association of high-risk human papillomavirus with esophageal squamous cell carcinomas among Koreans, as determined by polymerase chain reaction. Dis Esophagus. 21(2): 114-7.
- Kok TC, Nooter K, Tjong-A-Hung SP, Smits HL, Ter Schegget JT (1997) No evidence of known types of human papillomavirus in squamous cell cancer of the oesophagus in a low-risk area. Rotterdam Oesophageal Tumour Study Group. Eur J Cancer. 33(11): 1865-1868.
- Morgan RJ, Perry AC, Newcomb PV, Hardwick RH, Alderson D (1997) Human papillomavirus and oesophageal squamous cell carcinoma in the UK. Eur J Surg Oncol. 23(6): 513-7.
- Sargolzaei S, Farhadi S, Kazemi B, Bandehpour M, Kharazifard MJ (2014) The correlation between p16 expression and INK4a locus mutation with grades and stages in oral squamous cell carcinoma. Indian J Pathol Microbiol. 57(1): 24-30.
- Syrjänen K, Gissmann L, Koss LG (1987) Papillomaviruses and human disease. Springer Verlag-Berlin Heidelberg.
- de Villiers, K Gundt, H Stien, H Scherubl (2004) Esophageal squamous cell cancer in patients with head and neck cancer: Prevalence of human papillomavirus DNA sequences. Int J Cancer. 109(2): 253-258.
- Chang F, Syrjänen SM, Wang L, Syrjanen K (1992) Infectious agents in the etiology of esophageal cancer. Gastroenterology. 103(4): 1336–48.
- Zur Hausen H (1996) Papillomavirus infections: a major cause of human cancers. Biochim Biophys Acta. 1288(2): F55-F78.
- Mellin Dahistrand H, Lindquist D, Bjornestal L, Ohisson A, Dalians T, et al., (2005) P16(INK4A) corrlates to human papillomavirus presence, response to radiotherapy and clinical outcome in tonsillar carcinoma. Anticancer Res. 25(6c): 4374-4383.
- Hille J, Margolius K, Markowitz S, Isaacson C (1986) Human papillomavirus infection related to oesophageal carcinoma in black South Africans. A preliminary study. S Afr Med J. 69: 417–420.
- Kerr E, Helwick C (2009) High p16 Antibody Levels May Signal HPV Infection in Head and Neck Cancer. American Society for Clinical Pathology (ASCP) Annual Meeting: Abstract 84.
- Yu N, Mashima Y, Kameyama K, Mukai M, Oguchi Y (1997) Detection of human papillomavirus infection in squamous tumours of the conjunctiva and lacrimal sac by immunohistochemistry, in situ hybridisation, and polymerase chain reaction. Br J Ophthalmol. 81(4): 308–313.
- Reimers N, Kasper HU, Weissenborn SJ, Stutzer H, Preuss SF et al., (2007) Combined analysis of HPV-DNA, p16 and EGFR expression to predict prognosis in oropharyngeal cancer. Int J Cancer. 120(8): 1731–1738.
- Missaoui N, Hmissa S, Frappart L, Trabelsi A, Traore C, et al., (2006) P16(INK4a) overexpression and HPV infection in uterine cervix adenocarcinoma.Virchows Arch. 448(5): 597-603.
- Busatto G, Y-H Shiao, Parenti AR, Baffa R, Ruol A et al., (1998) p16/ CDKN2 alterations and pRb expression in oesophageal squamous carcinoma. J Clin Pathol: Mol Pathol. 51: 80–84.
- Guang-Cheng D, Jing-Li R, Chang FB, Ji-Lin Li, Yuan L, et al., (2010) Human papillomavirus DNA and P16INK4A expression in concurrent esophageal and gastric cardia cancers. World J Gastroenterol. 16(46): 5901-5906.
- Deng Z, Hasegawa M, Aoki K, Matayoshi S, Kiyuna A, et al., (2014) A comprehensive evaluation of human papilloma virus positive status and P16INK4A overexpression as a prognostic biomarker in head and neck squamous cellcarcinoma. Int J Oncol. 45(1): 67-76.
- Murthy S. Sudha, Sharma A, Aaditya JV, Sarada J (2014) The role and significance of immunohistochemical method in oral neoplasia. IJRSR. 5(6): 1108-1111.
- Patil S, Rao RS, Amrutha N, Sanketh DS (2014) Analysis of human papilloma virus in oral squamous cell carcinoma using p16: An immunohistochemical study. J Int Soc Prev Community Dent. 4(1): 61-66.





