Molecular Characterization of Human Adenoviruses in Children Suffered From Acute Gastroenteritis By Partial Hexon Region
Rambha Tripathi1, 2, Vani Gupta2, Divya Gupta1, 2, Dharam Veer Singh1, Pooja Gaur1, Ravish Katiyar1, Shally Awasthi2, Piyali Bhattacharya1, Tapan N Dhole1*
1 Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
2 King George’s Medical University, Lucknow, Uttar Pradesh, India.
*Corresponding Author
Dr. Tapan N Dhole,
Professor and Head, Department of Microbiology,
Sanjay Gandhi Postgraduate Institute of Medical Sciences, Raebareli Road,
Lucknow -226014, Uttar Pradesh, India.
Tel. : +91-522-2494263
Fax : +91-522-2668100
E-mail: tndhole@sgpgi.ac.in
Received: June 24, 2016; Accepted: August 09, 2016; Published: September 01, 2016
Citation: Tapan N Dhole, et al., (2016) Molecular Characterization of Human Adenoviruses in Children Suffered From Acute Gastroenteritis By Partial Hexon Region. Int J Virol Stud Res. 4(4), 42-47.dx.doi.org/10.19070/2330-0027-160007
Copyright: Tapan N Dhole© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Viral gastroenteritis is an important cause of childhood morbidity and mortality, in developing countries. Human adenovirus (HAdV) poses a major risk in children, elderly people and immunocompromised persons, causes acute diarrhea at irregular intervals as well as in outbreaks.
Aim: The study was aimed to investigate the molecular characterization and associated clinical features of HAdV infection in North Indian children affected with acute gastroenteritis (AGI) infection.
Materials and Methods: HAdV has been identified by PCR, targeting partial hexon gene from fecal specimen of 250 AGI affected children.
Results: A total 14 (5.6%) HAdV positives were confirmed by PCR, among them 8 males (3.2%) and 6 (2.4%) were females. Maximum positivity was 57.14% in the age group of 0-5 years AGI affected children. HAdV-B was the most prevalent followed by C, D, F and A in North Indian children, out of them serotype B3 (28.57%) was prevalent, followed by C2, C5 and F41 (14.29% each); A12, B34, D63 and D28 (7.14% each).
Conclusion: This study contributes to a better understanding about HAdV that might involve in AGI illnesses in young children, prognosis helps in planning and prevention from HAdV infection. HAdV-B3 was the most common adenovirus serotypes circulating in the North India. To the best of our knowledge, this is the first study on genetic molecular characterization of HAdV strains from North Indian AGI children.
2.Introduction
3.Materials and Methods
3.1 Sample collections
3.2 Processing of Gastroenteritis Samples
3.4 DNA Extraction
3.5 PCR for Detection of Adenovirus
3.6 Sequence and Phylogenetic Analysis
4.Results
4.1 Serotyping
5.Discussion
6.Acknowledgements
7.References
Keywords
AGI; HAdV; PCR; Hexon Gene; Phylogenetic Analysis.
Abbreviations
AGI: Acute Gastroenteritis; HAdV: Human Adenovirus; KGMU: King George Medical University; PCR: Polymerase Chain Reaction; SGPGIMS: Sanjay Gandhi Post Graduate Institute of Medical Sciences; WHO: World Health Organization.
Introduction
Viral gastroenteritis is an important cause of childhood morbidity and mortality, in developing countries [1]. Every year 2.5 million deaths are estimated to occur due to enteric infections, greatly impacting children younger than five years of age [2]. Human adenovirus (HAdV) creates a major risk in children, elderly people and immunocompromised persons [3]. It causes acute diarrhea at irregular intervals as well as in outbreaks [4]. HAdV can cause a broad range of human diseases such as acute respiratory tract infection (ARTI), pneumonia, bronchitis, conjunctivitis, hepatitis, ocular infection, hemorrhagic cystitis,Gastroenteritis, GI and urinary tract infection (UTI). HAdV infectivity is transmitted by inhalation and direct contact with small droplet aerosols or the fecal-oral route [5]. HAdV discovered in 1953 and its prevalence is approximately 4-12% in acute gastroenteritis (AGI) and ARTI [6]. It belongs to the family Adenoviridae and genus Mastadenovirus and these are non-enveloped, icosahedral viruses. Adenoviruses have linear double-stranded DNA that generally range from 26 to 45 kb and are encapsulated in an icosahedral protein shell, particles ranges from 70-90 nm in size. Based on genomic studies, 68 types of HAdV have been recently classified, which can be divided into seven different species (A-G) [7, 8]. Virus was detected by PCR using degenerate primers targeting highly conserved region of partial hexon gene [9] and characterized by sequencing and phylogenetic analysis.
So, the present study planned for molecular characterization of HAdV in children suffering from AGI by PCR method of hexon gene and also to determine species and serotypes of HAdV that are circulating in North Indian children.
Casas et al., (2005), developed and validated a novel methods for species and serotypes by phylogenetic analysis using multiple sequence alignment with some reference sequences represents each known serotypes in data base [9]. We also use some reference sequence and method to assign species and serotypes of our unknown sequence.
A total 250 clinically diagnosed cases of AGI in children of age group less than 15 years were recruited in the study. Fecal specimens were collected after obtaining informed consent from Department of Microbiology, SGPGIMS Lucknow and Department of Pediatrics, KGMU, Lucknow, Uttar Pradesh, India, during the March 2012 to September 2013. In 2012, we have collected 123 stool specimen and 127 fecal specimens in 2013. The study protocol was approved by the Ethics Committee of SGPGIMS and KGMU Lucknow. We have collected 15-20 ml liquid of watery stool and one sample per patient in a clean and dry screw capped, wide mouth plastic container. Samples were immediately transported (maintaining the cold chain) and stored at -20°C for further analysis.
For viral detection stools were processed as per WHO guidelines [10]. Briefly, Stool suspension (10%) was prepared in 0.01 M phosphate buffered saline (PBS) (PH 7.2) in a biosafety cabinet level II and vortex at 300 rpm for 20 minutes followed by centrifugation at 3000 rpm for 30 minutes at 4°C. Leaved for 10 minutes at room temperature (RT) and supernatant was stored at -20°C for further analysis.
Viral DNA extracted from 200 μl stool supernatant using the QIAmp, DNA extraction mini kit (Qiagen, Valencia, CA), according to manufacturer's instructions. DNA was stored at -80°C for further identification.
For the amplification and detection of HAdV, we used 5μl of DNA in 45μl of reaction mixture containing 10 mM Tris-HCL (pH8.3), 50 mM KCL, 500 mM (each) dNTPs, 4 mM MgCl2, 0.5 μl of Taq polymerase (5U/μl) and 20 pmol of the generate forward 5’-CAACACCTAYGASTACATGAA-3’ and reverse primer 5’-KATGGGGTARAGCATGTT-3’ with PCR having initial denaturation step at 94°C for 5minutes, denaturation at 94°C for 1 minute, annealing at 50°C for 1 minute, extension at 68°C for 1 minute for 30 cycles and a final extension at 68°C for 5 minutes [9]. The amplified product of 475 bp was visualized on 2% agarose gel pre-stained with ethidium bromide along with molecular weight marker VIII (Sigma-Aldrich) under ultraviolet light, imaged with Gel Doc XR System (Bio-Rad, Hercules, CA). The PCR products were commercially sequenced by Sanger sequencing method.
Molecular identification of each serotype was done by pair-wise comparison of the partial hexon amplicon sequence with database of all HAdV serotypes using the BLAST program (blast.ncbi.nlm.nih.gov/Blast.cgi) from Gene bank. The sequence data were aligned by Clustal W multiple sequence alignment tool. The evolutionary history was inferred by the neighbour-joining method, based on the Kimura 2-parameter model and 1000 bootstrap replications using the MEGA 6 software program (www.megasoftware.net) showed in Figure 4.
Results
In this study, we have analyzed 250 AGI fecal specimens (Males =117; Females=133), median age was 84 months (minimum 3 months, max. 180 months). A total 14 (5.6%) specimens were found positive for HAdV (adeno positive band showed in Figure 1), among them 8 male (3.2%) and 6 (2.4%) were female pediatric patients with median age was 38 months (minimum 3 months, max. 158 months), showed in Table 1. Maximum positivity was 57.14% in the age group of 0-5 years, while equal numbers of positivity (21.43%) were observed in each age group; 5-10 years and 10-15 years. HAdV-C (37.5%) was the most common species in the age group of 0-5 years followed by B (25%), A, D and F (12.5%), whereas in age group 5-10 years the HAdV-B (25%) were frequent followed by species D (12.5%). In higher age group of 10-15 years species B, C and F (12.5%) were equally represented (Figure 2). HAdV-B was the most prevalent followed by C, D, F and A in North Indian children.
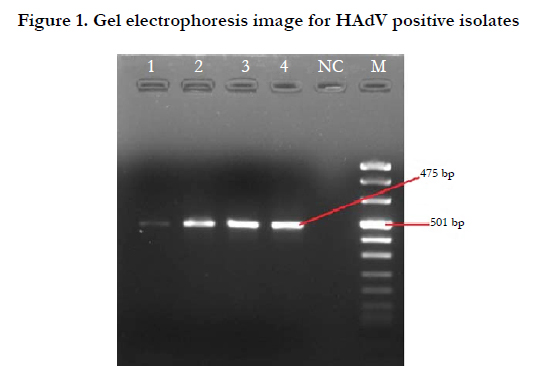
Figure 1. Gel electrophoresis image for HAdV positive isolates
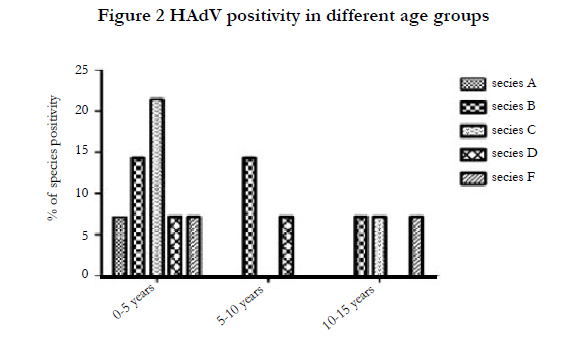
Figure 2. HAdV positivity in different age groups
Serotyping has been done by phylogenetic analysis taking reference sequences representing each serotype [9]. HAdV-B3 (28.57%) was prominent serotype, followed by C2, C5, F41 (14.29% each), A12, B34, D63 and D28 (7.14 % each) showed in Figure 3. The percentage of HAdV infection per year calculated in 2012 and 2013 was 71.43% and 28.57% respectively. The HAdV infection was most prevalent in 2012. Overall, HAdV infection was recorded higher during the spring season peak in month February to March and in rainy season May to September. General clinical features of gastroenteritis AGI in the study participants were; watery stool, high fever, vomiting, abdominal pains and dehydration. Among the participants that tested positive for adenovirus, the recorded clinical manifestations are presented in Table 2. HAdV positive patient’s details, including age/gender, main clinical symptoms and identified serotypes are showed in Table 3.
Phylogenetic analysis identified 97 to 99% similarities of strains with other circulating strains in different parts of India as well as
in other countries showed in Table 4 (and Figure 4).
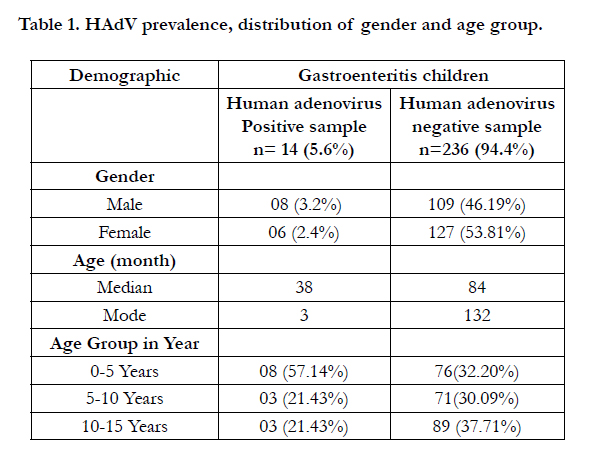

Table 1. HAdV prevalence, distribution of gender and age group.
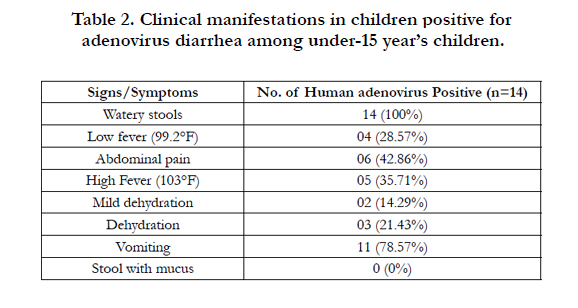
Table 2. Clinical manifestations in children positive for adenovirus diarrhea among under-15 year’s children.
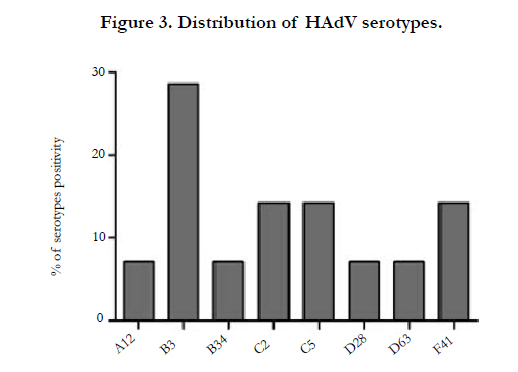
Figure 3. Distribution of HAdV serotypes.
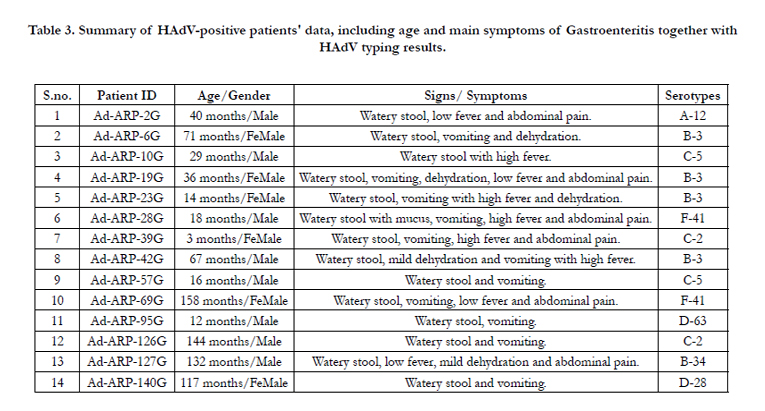
Table 3. Summary of HAdV-positive patients' data, including age and main symptoms of Gastroenteritis together with HAdV typing results.
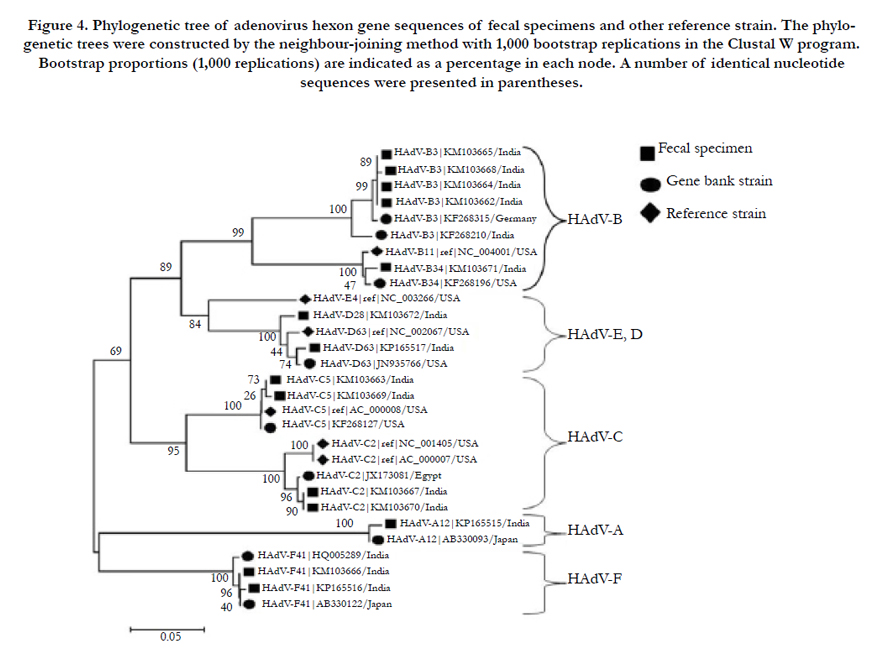
Figure 4. Phylogenetic tree of adenovirus hexon gene sequences of fecal specimens and other reference strain. The phylogenetic trees were constructed by the neighbour-joining method with 1,000 bootstrap replications in the Clustal W program. Bootstrap proportions (1,000 replications) are indicated as a percentage in each node. A number of identical nucleotide sequences were presented in parentheses.
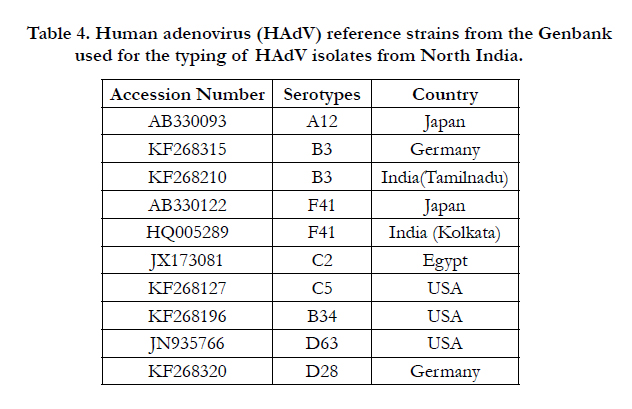
Table 4. Human adenovirus (HAdV) reference strains from the Genbank used for the typing of HAdV isolates from North India.
Discussion
HAdV is most commonly associated with AGI illnesses. Young children and immunocompromised patients are especially vulnerable to severe complications of HAdV infection [11, 12]. Our data shows that, during the study period (March 2012 to September 2013), the highest rate of HAdV infection occurred in 2012. The seasonal distribution of HAdV infection shows a higher prevalence in spring season (42.86%; February and March) and in rainy season (57.14%; May to September), which is similar to Dhaka city, Bangladesh 2009 [13].
In the present study the rate of HAdV infection was found 5.6% which is higher than previous similar studies, 3.1% in Tunisia [14], 1.9% in Dhaka city, Bangladesh [13] and lower than Egypt; 10.4% [15], Ghana; 19.8% [16], in northwest Nigeria; 23% [17], Albania 23.2% [3], and 37.4% in Kenya [18]. Male/female ratio (M/F) of HAdV infected pediatric children were 1.33:1, similar to Taiwan 1.30:1 [19], where as HAdV infection is higher in Israel 1.48:1 [20].
According to their age group, 0-5 years of infants and children the higher rates of HAdV infection was 57.14% which is similar to other studies of HAdV infections worldwide [20]. Cooper et al., demonstrated that, children had been infected early in life, had acquired immunity to this infection [21]. Species B shows the consistent results 25% positivity in age groups 0-5 years and 5-10 years of HAdV affected children, but the result varies in the age group 10-15 years children, species B shows the low positivity 12.5%.
The sequence based analysis of the partial hexon gene showed the presence of HAdV serotypes A12, B3, B34, C2, C5, D28, D63 and F41 in AGI infected children [22-25]. HAdV-B and C species shows higher prevalence followed by species D, F and A respectively. We have investigated the HAdV-B3 predominant genotype prevalent in the year 2012, and our findings was supported by China published in 2012 [26, 27]. HAdV-B3 genotype was most prevalent and the results is supported by previous study by Yeung R et al., [28] in Canadian Population. Very few studies have been published from India in which they have mostly found the A12,B3, C2, C5, F40 and F41 HAdV serotypes [29, 30]. A study from Chennai, India found the HAdV B3 serotypes [29]. A study from Chicago shows the diarrhea causing HAdV are known to be associated with AGI in children [31]. As seen in our study fever, vomiting, watery stools and dehydration are usually associated features of AGI more so of viral GI.
Phylogenetic analysis reveals that, 97-99% similar strains are found in India and across the other countries. C5, B34, D63 are most common strains circulating in USA where as B3, D28 strains are common in Germany and B3, F41 are common strains in Tamilnadu and Kolkata (India) respectively. By the phylogenetic analysis we can conclude that, the source country of particular strains are A12 Japan; B3, D28 Germany; B3 Tamilnadu; F41 Japan, Kolkata; C2 Egypt; C5, B34, D63 USA. Further studies are needed to validate our results with long samples sizes in AGI children affected with HAdV infection.
The resulting data is very useful to understand the molecular characterization and seasonal distribution of HAdV infection in North Indian children and this information can be used to take preventive actions for controlling future outbreaks of HAdV.
In conclusion, this study indicates that HAdV-B was the most common adenovirus species circulating in the North Indian children. To the best of our knowledge, this is the first study on molecular characterization of HAdV strains from North Indian AGI children.
Acknowledgements
This study was supported by an ICMR-SRF fellowship awarded to Mrs. Rambha Tripathi from Indian Council of Medical Research, Government of India, New Delhi (Ref. no. 80/840/2013-ECDI). I acknowledge Ms. Ankita Pandey for technical assistance.
References
- Hart C, N Cunliffe, O Nakagomi (2009) Diarrhoea caused by viruses. Manson’s tropical diseases. (22nd ed.), Philadelphia: Saunders Elsevier, 815-24.
- Girard MP (2006) A review of vaccine research and development: human enteric infections. Vaccine 24(15): 2732-2750.
- La Rosa G (2015) Genetic diversity of human adenovirus in children with acute gastroenteritis, Albania, 2013–2015. BioMed research international, 2015.
- Van R (1992) Outbreaks of human enteric adenovirus types 40 and 41 in Houston day care centers. The Journal of pediatrics 120(4): 516-521.
- Sriwanna, P.( 2013) Molecular characterization of human adenovirus infection in Thailand, 2009–2012. Virology journal. 10(1):1.
- Echavarría M ( 2009) Adenoviruses. eLS,
- Davison, A.J., M. Benkő,B. Harrach ( 2003) Genetic content and evolution of adenoviruses. Journal of General Virology 84(11): 2895-2908.
- Wold W, M Horwitz ( 2007) Adenoviruses. Fields virology 2: 2395-2436.
- Casas I (2005) Molecular identification of adenoviruses in clinical samples by analyzing a partial hexon genomic region. Journal of clinical microbiology 43(12): 6176-6182.
- World Health Organization.(2004 ) Polio laboratory manual.( 4th edition), Department of Immunization, Vaccines and Biologicals. Geneva, Switzerland.
- Kojaoghlanian T, P Flomenberg, MS Horwitz (2003) The impact of adenovirus infection on the immunocompromised host. Reviews in medical virology 13(3):155-171.
- Walls T, A Shankar, D Shingadia (2003) Adenovirus: an increasingly important pathogen in paediatric bone marrow transplant patients. The Lancet infectious diseases 3(2): 79-86.
- Dey SK (2009) Molecular epidemiology of adenovirus infection among infants and children with acute gastroenteritis in Dhaka City, Bangladesh.Infection, Genetics and Evolution 9(4): 518-522.
- Fodha I (2006) Identification of viral agents causing diarrhea among children in the Eastern Center of Tunisia. Journal of medical virology 78(9):1198-1203.
- Kamel AH (2009) Predominance and circulation of enteric viruses in the region of Greater Cairo, Egypt. Journal of clinical microbiology 47(4): 1037-1045.
- Silva PA (2008) Molecular characterization of enteric viral agents from children in northern region of Ghana. Journal of medical virology 80(10):1790-1798.
- Aminu M (2007) Adenovirus infection in children with diarrhea disease in Northwestern Nigeria. Annals of African medicine 6(4): 168-73.
- Magwalivha M (2010) High prevalence of species D human adenoviruses in fecal specimens from Urban Kenyan children with diarrhea. Journal of medical virology 82(1): 77-84.
- Tsou TP ( 2012) Community outbreak of adenovirus, Taiwan, 2011. Emerg Infect Dis 18(11):1825-1832.
- Mandelboim M (2011) Adenovirus infections in hospitalized patients in Israel: epidemiology and molecular characterization. Journal of clinical microbiology49(2): 597-601.
- Cooper R (2000) The epidemiology of adenovirus infections in Greater Manchester, UK 1982–96. Epidemiology and infection 125(2): 333-345.
- Ishiko H (2008) Novel human adenovirus causing nosocomial epidemic keratoconjunctivitis. Journal of clinical microbiology 46(6): 2002-2008.
- Sirena D (2005) The nucleotide sequence and a first generation gene transfer vector of species B human adenovirus serotype 3. Virology 343(2): 283-298.
- Pauly M (2015) Adenovirus in Rural Côte DIvoire: High Diversity and Cross-Species Detection. Ecohealth 12(3): 441-452.
- Singh G (2012) Overreliance on the hexon gene, leading to misclassification of human adenoviruses. Journal of virology 86(8): 4693-4695.
- Zou L (2012) Human adenovirus infection in children with acute respiratory tract disease in Guangzhou, China. Apmis 120(8): 683-688.
- Xie L (2012) Two adenovirus serotype 3 outbreaks associated with febrile respiratory disease and pharyngoconjunctival fever in children under 15 years of age in Hangzhou, China, during 2011. Journal of clinical microbiology 50(6): 1879-1888.
- Yeung R (2009) Characterization of culture-positive adenovirus serotypes from respiratory specimens in Toronto, Ontario, Canada: September 2007–June 2008. Virology journal 6(1): 1.
- Janani M, J Malathi, H Madhavan (2012) Isolation of a variant human adenovirus identified based on phylogenetic analysis during an outbreak of acute keratoconjunctivitis in Chennai. The Indian journal of medical research.136(2): 260-4.
- Dey RS (2011) Circulation of a novel pattern of infections by enteric adenovirus serotype 41 among children below 5 years of age in Kolkata, India. Journal of clinical microbiology 49(2): 500-505.
- Christensen ML ( 1989) Human viral gastroenteritis. Clinical microbiology reviews 2(1): 51-89.





