A Decisive Role of [18F] Fdg PET/CT for Diagnosis of Neoplastic Vascular Thrombosis:
Report of A Case
Travaini LL1*, Chiappa A2, Monteleone M2, Orecchia R3,4, Grana CM1
1 Division of Nuclear Medicine, European Institute of Oncology, Milano, Italy.
2 Department of General Surgery-Laparoscopic Surgery, European Institute of Oncology and University of Milano, Italy.
3 Scientific Directorate, European Institute of Oncology, Italy.
4 Chair of Radiation Therapy, University of Milan, Scientific Directorate, European Institute of Oncology-Milano, Italy.
*Corresponding Author
Laura Lavinia Travaini, MD,
Division of Nuclear Medicine,
European Institute of Oncology, Via Ripamonti, 435, 20141- MILANO, Italy.
Tel: ++39/ 02.5748.9043
Fax: ++39/ 02.5748.9040
E-mail: laura.travaini@ieo.it
Received: August 12, 2016; Accepted: August 24, 2016; Published: August 29, 2016
Citation: Travaini LL, Chiappa A, Monteleone M, Orecchia R, Grana CM (2016) A Decisive Role of [18F] Fdg PET/CT for Diagnosis of Neoplastic Vascular Thrombosis: Report of A Case. Int J Surg Res. 3(4), 52-54.
doi: dx.doi.org/10.19070/2379-156X-1600011
Copyright: Travaini LL© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The combined use of PET scan with CT and fluorodeoxyglucose ([18F]FDG) can modify, in selected oncologic patients, the clinical management and care. We report here the case of a 63-year old female who showed increase serum level of CEA 3 years following left colectomy for cancer. Ultrasound and CT (computed tomography) of the abdomen showed a single lesion in the segment II of the liver with portal thrombosis. [18F] FDG PET/CT revealed two lesions (the first area was histologically proven to be a colorectal carcinoma metastasis, the second one corresponded to the portal thrombosis). No antithrombotic drugs were administered and patient underwent chemotherapy for 4 courses (eloxatin plus 5-fluorouracil anf leucovorin). Liver resection was performed 2 weeks after the end of chemotherapy, and intraoperative ultrasound revealed a normal portal flow.
2.Abbreviations
3.Introduction
4.Case Report
5.Discussion
6.References
Keywords
Neoplastic Vascular Thrombosis; Fluorodeoxyglucose; Liver Metastasis; PET/CT.
Abbreviations
PET: Positron Emission Tomography; CT: Computed Tomography; FDG: Fluorodeoxyglucose; CEA: Carcinoembryonic antigen; MD-CT: Multi Detector Computed Tomography; IOUS: Intraoperative Ultrasound.
Introduction
Positron emission tomography (PET) is a useful diagnostic procedure in cancer patients [1]. In particular, the combined use of PET and Computed Tomography (CT) (PET/CT) led to a change in the clinical management of 36% of patients with recurrent or metastatic colorectal cancer [2]. In oncological patients, serum tumor markers increasing, is highly suspected for presence of disease and PET/CT with fluorodeoxyglucose ([18F] FDG) can modify patient’s management revealing the precise site of neoplastic foci.
Case Report
A 63-year-old female with clinical history of colon cancer was referred to our Institute for a mild increase of carcino-embryonic antigen (CEA) serum level. In 1997 the patient was submitted to left colectomy for adenocarcinoma (pT3; pN0). Adjuvant chemotherapy was carried out without significant effects. In the follow-up the patient performed abdomen ultrasound every two years and laboratory tests every year. In the last six months a slow and persistent CEA serum level increasing was evident. On physical examination, she was asymptomatic. Abdominal ultrasound showed a single liver lesion in the segment II, and portal thrombosis (Figure 1). Multi-detector CT (MDCT) revealed a liver nodule suggestive for metastatic lesion and portal thrombosis with no enhancement (Figure 2). The undetermined nature of the portal thrombosis pointed out the indication of completing the patient’s staging with [18F] FDG PET/CT. In fasting conditions and euglicemic state, 370 MBq of [18F] FDG were intravenously injected and after 50 minutes a PET/CT scan was carried out. Total body scan revealed two areas of intense [18F] FDG uptake in liver parenchyma (Figure 3).
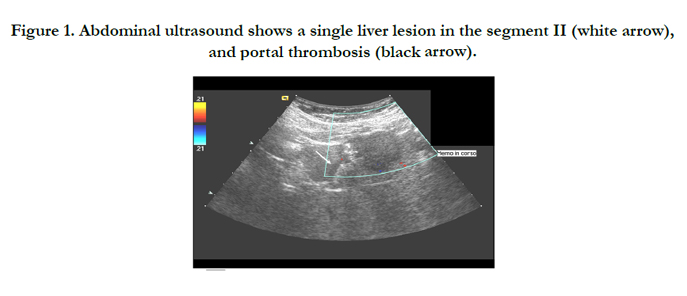
Figure 1. Abdominal ultrasound shows a single liver lesion in the segment II (white arrow), and portal thrombosis (black arrow).
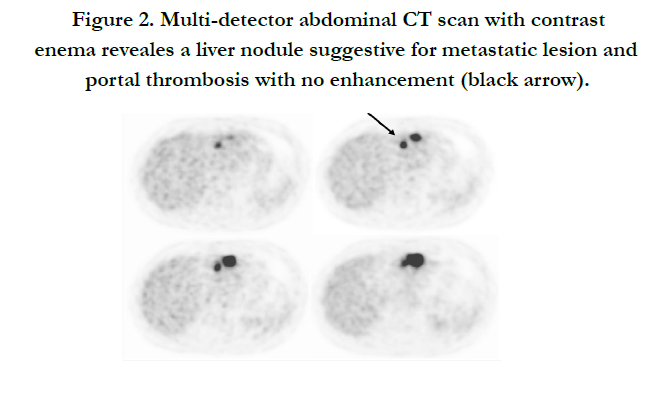
Figure 2. Multi-detector abdominal CT scan with contrast enema reveales a liver nodule suggestive for metastatic lesion and portal thrombosis with no enhancement (black arrow).
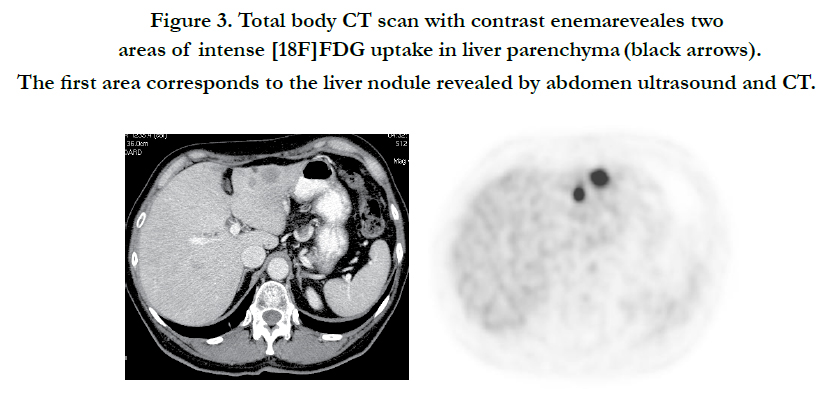
Figure 3. Total body CT scan with contrast enemareveales two areas of intense [18F]FDG uptake in liver parenchyma (black arrows). The first area corresponds to the liver nodule revealed by abdomen ultrasound and CT.
The first area corresponded to the liver nodule revealed by abdomen ultrasound and MDCT. This lesion was later histologically confirmed to be neoplastic through an US-guided liver biopsy. The second report, analyzing MDCT and PET/CT imaging, corresponded to the portal thrombosis (Figure 4). No other abnormal areas of [18F] FDG uptake were revealed in the scan.
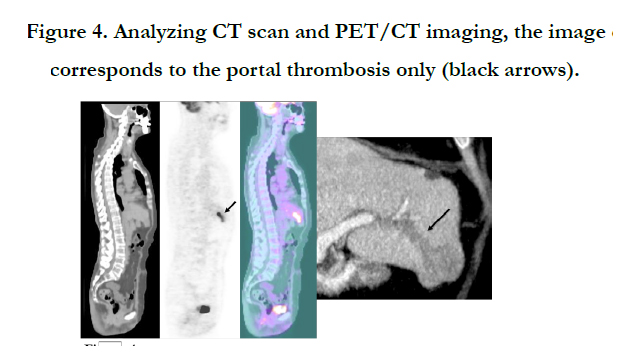
Figure 4. Analyzing CT scan and PET/CT imaging, the image corresponds to the portal thrombosis only (black arrows).
Because of intense [18F] FDG uptake, no signs and/or symptoms of acute thrombosis, its upstream location, no enhancement on MDCT and no vascolarization on color-Doppler ultrasound we interpreted the thrombosis as neoplastic.
Based on this consideration, no anti-thrombotic drugs were administered. Patient underwent four courses of chemotherapy (eloxatin combined with 5-Fluorouracil and leucovorin) without significant collateral effects.
At the end of chemotherapy an evaluation through abdomen ultrasound and CT documented significant reduction of dimension of liver lesion and disappearance of portal thrombosis. Two weeks following chemotherapy patient underwent surgery for liver metastasectomy. The intraoperative ultrasound of portal thrombosis resulted completely normal in the remnant liver.
Discussion
In this case conventional imaging findings were not pathognomic for the neoplastic nature of thrombosis but the characteristics of each diagnostic procedures and the disappearance after chemotherapy without administration of anti-thrombotic drugs resulted harmonious.
[18F] FDG PET/CT and CT, sometimes, are complementary techniques in staging and restaging patients with colorectal cancer. The combination of these two modalities may significantly impacts upon patient management.
Some 50% of patients with colorectal cancer develop liver metastases and die of their disease [3]. Surgical resection of colorectal metastases improves 5-year survival between 25 and 40%. Surgical failure and recurrent disease may be due to inadequate initial evaluation of metastatic disease [4-6].
Likely, [18F]FDG PET/CT can detect neoplastic foci in the vascular district, helping morphological imaging in a more specific diagnosis.
This finding support the use of [18F] FDG PET in the followup of patients with suspected colorectal liver metastases and equivocal findings on conventional diagnostic investigation.
References
- Gambhir SS, Czernin J, Schwimmer J, et al. (2001) A Tabulated summary of the FDG PET Literature. J Nucl Med 42(5Suppl):1S-93S.
- Staib L, Schirrmeister H, reske SN, et al. (2000) Is (18)F-fluorodeoxyglucose positron emission tomography in recurrent colorectal cancer a contribution to surgical decision making? Am, J Surg 180(1):1-5.
- Rosa F, Meimarakis G, Stahl A, BummR, Hahn K, tatsch K, Dresel S (2004) Colorectal cancer patients before resection of hepatic metastases. Impact of (18)F-FDG PET on detecting extrahepatic disease. Nuklearmedizin 43(4):135-40.
- Arulampalam TH, Francis DL, Visvikis D, Taylor I, Ell PJ. (2004) FDGPET for the preoperative evaluation of colorectal liver metastases. Eur J Surg Oncol 30(3): 286-91.
- Chiappa A, Bertani E, Makuuchi M, et al.(2009) Neoadjuvant chemotherapy followed by hepatectomy for primarily resectable colorectal cancer liver metastases. Hepatogastroenteroloy 56(91-92): 829-834.
- Chiappa A, Makuuchi M, Lygdakis NJ, Zbar AP, et al.(2009) The management of colorectal liver metastases: Expanding the role of hepatic resection in the age of multimodal therapy. Crit rev Oncol Hematol. 72(1): 65-75.





