Gallstone Coleus: A Rare Relation of Gallstone Ileus
Howells L1, Liasis L2, Demosthenous M3*
1 Foundation Year Doctor, Northwick Park Hospital, London, UK.
2 Consultant Surgeon, Hon Clinical Senior Lecturer, Imperial College School of Medicine, Northwick Park Hospital, London, UK.
3 Department of Cardiac Surgery, Hippocration General Hospital, Athens, Greece.
*Corresponding Author
Michael Demosthenous MD, PhD,
Department of Cardiac Surgery,
Hippokration Hospital, 114 Vasilissis Sofias Ave,
11527, Athens, Greece.
Tel: 00302132088543
Fax: 00302132088595
E-mail: drmikedemosthenous@gmail.com
Article Type: Review Article
Received: May 25, 2015; Accepted: June 25, 2015; Published: June 30, 2015
Citation: Howells L, Liasis L, Demosthenous M (2015) Gallstone Coleus: A Rare Relation of Gallstone Ileus. Int J Surg Res 2(4) 28-31. doi: dx.doi.org/10.19070/2379-156X-150006
Copyright: Demosthenous M© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Intestinal obstruction due to gallstones is a rare condition accounting for 1-4% of cases of a mechanical small bowel obstruction. Gallstone coleus (gallstone obstruction of the large bowel) is an even more uncommon cause of a mechanical bowel obstruction.
Methods: We performed a search of the PubMed database in December 2014. To the best of our knowledge all available case reports and case series were included. Reference sections were searched manually for additional potential cases. Search terms for gallstone coleus were used in all possible combinations. Our exclusion criteria embraced reports of gallstone obstruction of the small bowel, and duplicate cases. We found 57 publications that together produced a total of 63 case reports of gallstone coleus.
Conclusion: Gallstone coleus is a rare entity that carries a high mortality. It usually occurs in the elderly, who frequently suffer a wide variety of comorbidities. To lower mortality, it is advocated that in the elderly co-morbid patient, non-invasive options of stone extraction should be trialled as the treatment option of first choice.
2.Introduction
3.Methods
4.Results
4.1 Presentation & Pathogenesis
4.2 Patient demographics
4.3 Diagnosis
4.4 Treatment Options
5.Discussion
6.Conclusion
7.References
Keywords
Gallstones; Gallstone Coleus; Gallstone Ileus; Intestinal Perforation.
Introduction
Intestinal obstruction due to gallstones (gallstone ileus) is rare. The condition has, however, been widely documented with one review reporting as many as 1001 cases [1]. Gallstone obstruction of the large bowel (gallstone coleus) is much more rarely reported, and accounts for less than 8% of gallstone related intestinal obstruction [2]. Grey Turner first described the condition in 1932. His patient was a rotund man of 81 years, who had suffered bouts of absolute constipation associated with intermittent abdominal pain. A large gallstone, wedged at the level of the sigmoid colon, was extracted [3].
Methods
A search of the PubMed database was conducted in December 2014. To the best of our knowledge all available case reports and case series were included, without restriction on language. Reference sections were searched manually for additional potential cases. Search terms for gallstone coleus were used in all possible combinations. Our exclusion criteria embraced reports of gallstone obstruction of the small bowel, and duplicate cases. We found fifty-seven publications that together produced a total of sixty-three case reports of gallstone coleus.
Results
The presentation of gallstone coleus resembles that of large bowel obstruction from other causes. Typically, the patient will complain of abdominal pain, constipation, bloating, and nausea. Rarer presentations such as diarrhoea or ascending cholangitis can occur [4]. The right side of the transverse colon is in such close proximity to the gallbladder that it is often found to be bile stained after death. In some cases large gallstones may ulcerate through the wall of the gallbladder and into the transverse colon (autocholecystotransversecolostomy) [5]. This usually results from episodes of cholecystitis. Once inside the bowel lumen, the usual site of stone impaction is the sigmoid colon. A pathological process, such as diverticulitis, often narrows this location [6, 7].
Gallstone ileus causes less than 5% of cases of intestinal obstruction, but accounts for up to 25% of cases of small bowel obstruction in elderly patients [8]. The prevalence of gallstones is two or three times higher in women than in men, but this difference is less marked beyond the sixth decade. Our literature review showed that 58% of cases of gallstone coleus were women. The mean age of all patients reported was eighty-one years (Figure 1).
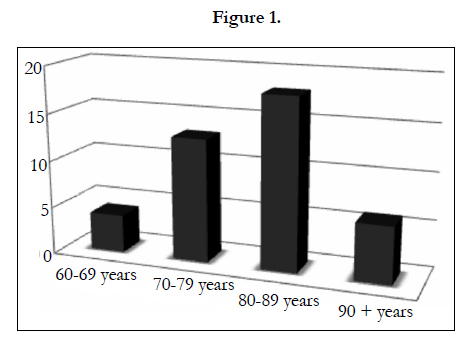
Figure 1.
Three findings in gallstone ileus – pneumobilia, small bowel obstruction and an ectopic gallstone seen on plain abdominal x-ray – comprise Rigler’s triad. The combination, however, is seen in less than 50% of cases [9]. This classic triad is sometimes, but not always seen in gallstone coleus, featuring large bowel obstruction rather than that of the small bowel [10]. In this review, plain abdominal x-ray demonstrated gallstones in thirteen cases (21%). Calcification aids identification of a gallstone on plain x-ray. Computed tomography (CT) scanning was frequently used and in our review supported diagnosis in forty cases (65%) of gallstone coleus. CT is recognised to be the gold standard imaging modality in the diagnosis of gallstone coleus [11].
There was only one published case of the spontaneous resolution of gallstone coleus. It was thought that a failed endoscopic attempt at removal had facilitated passage of the gallstone through the bowel [7]. The chances are that spontaneous outcome, when it occurs, is simply an event that passes unnoticed. Definitive surgical intervention appeared necessary in the remainder of cases. The literature demonstrated, however, an absence of consensus about what constitutes the most appropriate treatment.
In just over one third of reported cases, endoscopic methods of stone retrieval were first trialled (Figure 2). Such techniques require the use of a colonoscope, with a snare or basket attachment, or a mechanical or laser lithotripter. The use of ultra-sound guided extracorporeal shock wave lithotripsy has, in addition, been described. Of these non-invasive treatment options, the failure rate slightly exceeds that of success; 55% and 45% respectively.
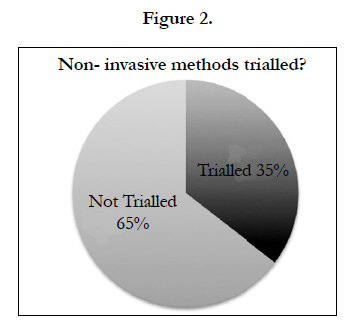
Figure 2.
Eighty percent of patients diagnosed with gallstone coleus in published cases were subjected to definitive surgical stone extraction, via laparotomy (75%) or laparoscopy (5%). Seventeen (27%) underwent a Hartmann’s procedure, four (6%) underwent colonic resection and primary anastomosis, whilst the creation of a defunctioning loop colostomy was chosen in five (8%). Colotomy also appeared to be widely used; an open colotomy with primary closure in twenty-one cases (34%), and a laparoscopic colotomy in three (5%). Conservative management was successful in just two cases (Figure 3).
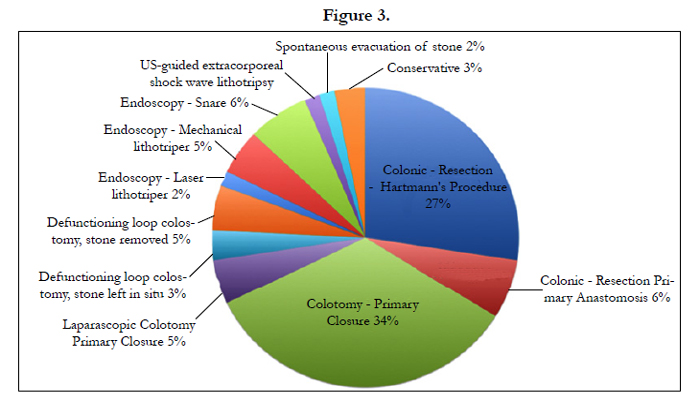
Figure 3.
Discussion
Patients who are diagnosed with gallstone coleus are usually elderly and co-morbid – so-called ‘high-risk surgical patients’. It is recognised that this minority contribute to the vast majority of postoperative deaths [12]. The mortality of a patient undergoing emergency laparotomy is around 25% [13]. To improve the situation it has become good practice to apply physiological scoring systems such as the P-POSSUM score, to predict the risks of mortality and morbidity, and guide appropriate clinical decisionmaking [14]. The 30-day mortality of patients who presented with gallstone coleus in this review of published cases reaches 21%. Of those who died, 77% had undergone laparotomy (Figure 4).
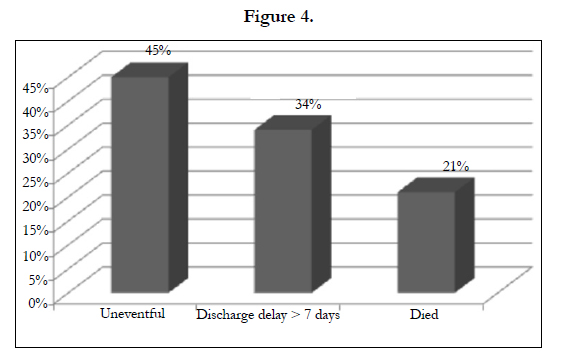
Figure 4.
Patients with gallstone coleus can be stratified into two groups based on the presence or absence of intestinal perforation. In the first group, there is clinical or radiological evidence of intestinal perforation and definitive surgical intervention offers the best prospect of reducing mortality. If CT scan confirms perforation, with free air and minimal local contamination, then laparoscopic attempts could be applied if the expertise is available. This would involve laparoscopic washout of the collection, plus segmental colonic resection with primary anastomosis, and proximal diverting ileostomy. Laparoscopic washout with laparoscopic segmental colonic resection and end colostomy provides an alternative.
When a laparoscopic surgeon is unavailable, emergency laparotomy should be performed. Patients undergoing emergency laparotomy have been the subject of ongoing quality improvement work [13]. Traditionally, Hartmann’s procedure would be the operation of choice. This entails resection of the affected segment of bowel together with the gallstone, and formation of an end colostomy. In the unstable surgical patient, a diverting proximal loop colostomy is an option. Where there is deemed to be reversal potential, a primary anastomosis with a diverting loop ileostomy provides a suitable alternative.
In the second group of patients, there is no evidence of intestinal perforation. Recognising the high mortality and morbidity rates of surgery, a conservative approach should be adopted whenever feasible. The first steps may consist of only the avoidance of anything by mouth, the correction of fluid and electrolyte imbalances, and nasogastric decompression if the patient is vomiting. Faecal softening enemas containing arachis oil can promote bowel movement, and offer the possibility of spontaneous passage of the gallstone.
When expectant treatment proves ineffective, non-invasive endoscopic stone retrieval, in techniques previously listed, can be trialled. The treatment of gallstone coleus differs appreciably from that of intestinal obstruction due to other causes, including that of gallstone ileus. Firstly, the obstructing gallstone may represent an accessible intraluminal foreign body. Secondly, when the stone is lodged distally, in the sigmoid colon, it may be removable by means of non-invasive surgical techniques. Gallstones can be crushed, fragmented, or lasered prior to transanal extraction of debris. The risks of colonoscopic retrieval compared with those of surgery, are lower, and patients are likely to require shorter periods of rehabilitation [15].
When non-invasive techniques fail in the patient without intestinal perforation, an attempt at laparoscopic stone extraction should be made. This is dependent on the availability of laparoscopic expertise. In cases where endoscopic retrieval has been attempted but failed, the endoscopist may have achieved proximal bowel deflation. In this situation, laparoscopic colotomy with stone removal and primary closure is more achievable.
Definitive surgical management may include enterolithotomy, cholecystectomy and fistula closure in one operation or as separate procedures [7]. In this review, however, the chosen method of stone extraction was combined with another surgical procedure in just ten reports (16%). The recurrence rate for gallstone ileus is reported to be less than 5% [16]. Moreover, the cholecystocolic fistula is usually symptomless. This would serve to negate the requirement for fistulectomy. The combined treatment choice with cholecystectomy may be viewed as superior, as it provides definitive treatment. It is, however, complex, prone to complication, and unsuitable in elderly patients [17]. Although the cholecystocolic fistula is usually symptomless, its repair serves to prevent recurrence [18]. The primary objective of treatment in this group of patients is to reverse the colonic obstruction to reduce mortality.
Conclusion
Gallstone coleus is a rare entity that carries a high mortality. It usually occurs in the elderly, who frequently suffer a wide variety of comorbid conditions. To lower mortality, it is advocated that in the elderly co-morbid patient, non-invasive options of stone extraction should be trialled as the treatment option of first choice. Currently there is no consensus on optimal management. Figure 5 shows a flowchart which summarises our proposed systematic approach to the treatment of patients with gallstone coleus.
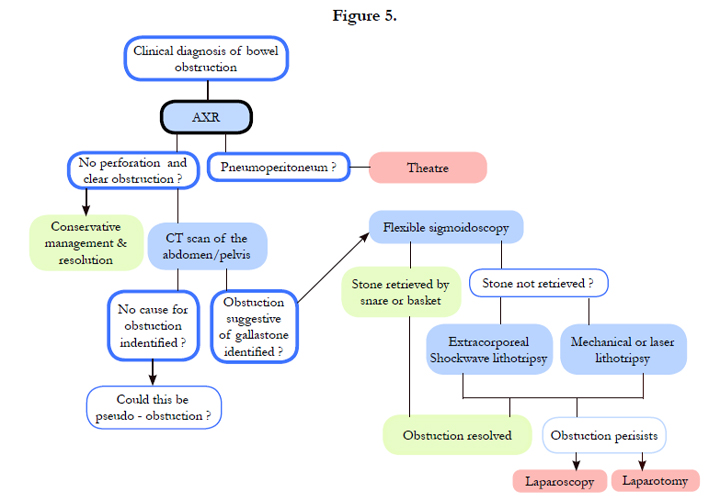
Figure 5.
References
- RM Reisner, JR Cohen (1994) Gallstone ileus: A review of 1001 reported cases. Am Surg 60(6): 441-446.
- P Anesline (1981) Colonic gallstone ileus. Postgrad Med J 57(663): 62–65.
- G Turner (1932) A giant gall-stone impacted in the colon and causing acute obstruction. Br J Surg 20(77): 28-33.
- RI Goldberg, RS Phillips, JS Barkin (1998) Spontaneous cholecystocolonic fistula treated by endoscopic sphincterotomy. Gastrointestinal Endoscopy 34(1): 55-56.
- P Thorek (1951) Anatomy in Surgery, J B Lippincott Company, Philadelphia. 474.
- S Doddi, NN Basu, T Kamal, TW Hennigan, P Sinha (2007) Large bowel obstruction due to gallstone: gallstone coleus. Grand Rounds 7: 36-38.
- GK Anagnostopoulos, G Sakorafas, T Kolettis, N Kotsifopoulos , G Kassaras (2004) A case of gallstone ileus with an unusual impaction site and spontaneous evacuation. J Postgrad Med 50(1): 55-56.
- Niloy Das, Nicholas R, Plummer, Hassan Raja, Ashok Vashist (2014) What to do with a non-rolling stone? Surgical on-table dilemma in large bowel obstruction due to an impacted gallstone. J surg case rep 7: 1-3.
- F Lassandro, N Gagliardi, M Scuderi, A Pinto, G Gatt, et al. (2004) Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol 50(1):23-29.
- LG Rigler, CN Borman, JF Noble (1941) Gallstone obstruction: pathogenesis and roentgen manifestation. JAMA 117(21): 1753-1759.
- CY Yu, CC Lin, RY Shyu, CB Hsieh, HS Wu, et al. (2005) Value of CT in the diagnosis and management of gallstone ileus. World J Gastroenterol 11(14): 2142-2147.
- GP Findlay, AP Goodwin, K Protopapa, M Mason, (2011) NCEPOD - POC: Knowing the risk: A review of the peri-operative care of surgical patients. Available from: http://www.ncepod.org.uk/2011report2/downloads/POC_fullreport.pdf
- R Pearse (2014) Enhanced peri-operative care for high-risk patients (EPOCH) Trial. A stepped wedge cluster randomised trial of a quality improvement intervention for patients undergoing emergency laparotomy. Lancet 1-28.
- DR Prytherch, MS Whiteley, B Higgins,PC Weaver, WG Prout, et al. (1998) POSSUM and Portsmouth POSSUM for predicting mortality. Physiological and Operative Severity Score for the enumeration of Mortality and morbidity. Br J Surg 85(9): 1217–1220.
- E Murray, M Collie, DW Hamer-Hodges (2006) Colonoscopic treatment of gallstone ileus. Endoscopy 38(2): 197.
- B Helou, TR Gadacz (2004) Gallstone ileus. Current Surgical Therapy. (8th edtn), Philadelphia, PA, Mosby. 426-428.
- AL Warshaw, MK Bartlett (1966) Choice of operation for gallstone intestinal obstruction. Ann Surg 164(6): 1051–1055.
- S Garcia-Lopez, JJ Sebastian, R Uribarrena, P Solanilla, JM Artigas (1997) Successful endoscopic relief of large bowel obstruction in a case of sigmoid colon gallstone ileus. J Clin Gastroenterol 24(4): 291-292.





