Lymphangiomatosis – A Rare Disease in Pediatrics
Tuan DM1, Lien DM1* , Hoan NTM1, Tran NTN1, Chuong LT1, Oanh HTK2
1 Respiratory Department of Vietnam National Hospital of Pediatrics, Vietnam.
2 Resident Doctor of Vietnam National Hospital of Pediatrics, Vietnam.
*Corresponding Author
Dang Mai Lien,
Respiratory Department of the Vietnam National Hospital of Pediatrics, Hanoi, Vietnam.
E-mail: dia_lan_lys@yahoo.com
Received: May 26, 2016; Accepted: June 23, 2016; Published: June 25, 2016
Citation: Lien DM, Tuan DM, Hoan NTM, Tran NTN, Chuong LT, Oanh HTK (2016) Lymphangiomatosis – A Rare Disease in Pediatrics. Int J Resp Dis Care Med.. 1(1), 1-3.doi:dx.doi.org/10.19070/2577-4409-160001
\
Copyright: Lien DM© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Lymphangiomatosis is rare in both adults and children. We present an 11 year old boy with right chylothorax. The formation of chylothorax was a result of diffuse lymphangioma in the mediastinum spreading to the pleura. In addition, this patient suffered from cystic bone lesions. The child was finally diagnosed as having lymphangiomatosis based on pleural biopsy and bone lesions found on CTs and MRI. He was treated by pleurectomy and propranol as well as control of anemia and infection.
2.Case Presentation
3.Pre-medical history
4.Examinination
5.Investigations
5.1.Chest – Xray
5.2.Further investigation
5.3.Pleural biopsy showed
5.4.Final diagnosis
6.Treatment
7.Discussion
8.Conclusion
9.References
KeyWords
Lymphangiomatosis; Chylothorax.
Case Presentation
An 11 year old boy was detected with a right hemothorax.
Pre-medical history
Normal delivery. When he was 3 years old, he was diagnosed with a pleural effusion. Six months before admission he was diagnosed with lymphangioma in the right armpit and was then operated on in a provincial hospital.
Examinination
He had diminished breath sounds in the lower lobe of the right lung with no rales and no dyspnea but had a mild cough. Chest tube output was 3 liters of blood per day. He suffered from severe anaemia. A cardiovascular examination was normal. Infectious status was unremarkable.
Investigations
Table 1.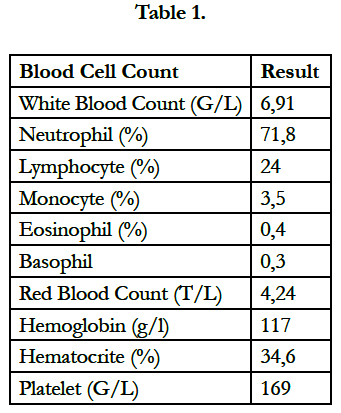

Table 1.
Right pleural effusion (Figure 1).
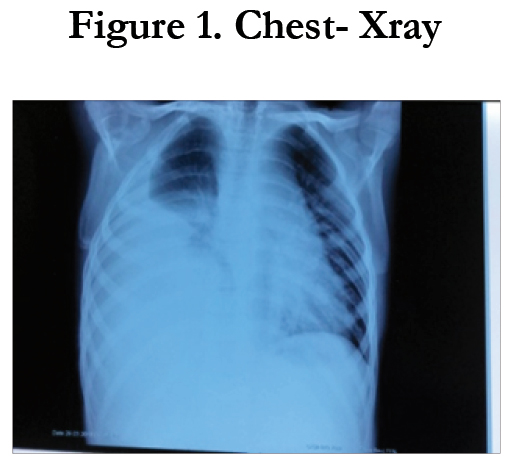
Figure 1. Chest- Xray.
Figure 1 showed a homogenous opacification in the right lower zone with the opacity seen to track along the lateral chest wall. The right costophrenic angle is obliterated. Findings are suggestive of a right side pleural effusion. Table 2.
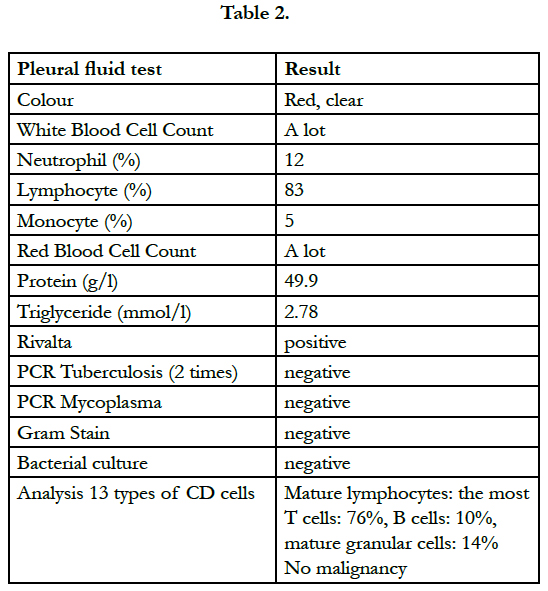
Table 2.
CTs (Figure 2) and MRI (Figure 3) suggested lymphangioma in the anterior mediastinum and bone lesions.
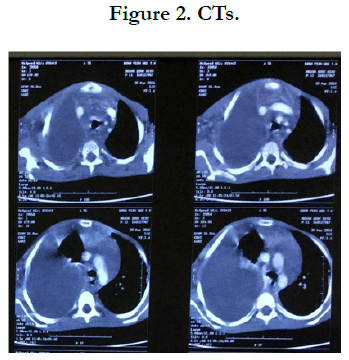
Figure 2. CTs.


Figure 3. MRI.
CTs showed diffuse lymphangioma in the anterior mediastinum and right pleura, and cystic bone lesions.
Lymphangioma (Figure 4).
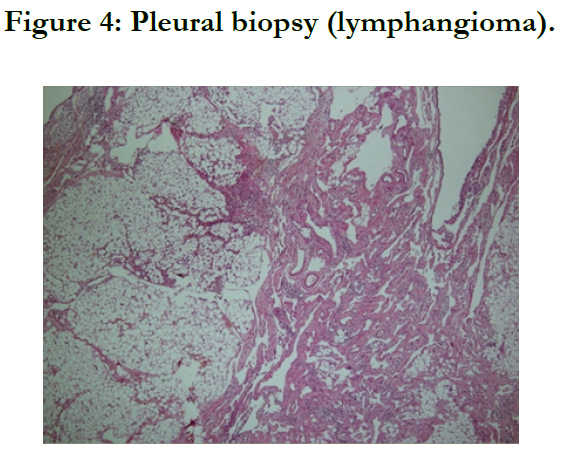
Figure 4: Pleural biopsy (lymphangioma).
The histopathological examination of the specimen showed the structure of tumor tissue which is characterized by large dilated, irregular vascular spaces lined by flattened, bland epithelial cells, with fibroblastic stroma and without red blood cells in the lumen. There is also the presence of moderate lymphocyte infiltration in the stroma. No malignant cell is identified (Figure 4).
Lymphangiomatosis.
Treatment
The patient was treated with pleural drainage, then pleurectomy, propranolol, antibiotics and blood transfusion.
Discussion
Lymphangiomatosis is a rare disease characterized by diffuse infiltration of lymphangiomas in the lung, bone and other tissues [1]. Within the thorax, lymphangiomas may be found in the mediastinum, heart, thoracic duct, lung, and pleura [2]. CTs and MRI helps to show the diffuse infiltration fluid in the mediastinum, pleural effusion and cystic bone lesions [7,8]. Gold standard is biopsy. Surgical removal and sclerotherapy have been effective in some cases when the disease is more localized. On the other hand, for treating diffuse lymphangioma, several drugs have been noted in the medical literature; for example, interferon alfa 2b, glucocorticoid and recently, propranolol [3-6,9]. Propranolol reduces the levels of vascular endothelial growth factor (VEGF) and the amount of chylous effusions [6].
In this patient, the diagnosis was more difficult as, on admission, signs of chylothorax were not clear due to its conjunction with a hemothorax which was attributable to lymphatico – venous malformation [10].
Diagnosing chylothorax was confirmed by increased Triglyceride in the pleural fluid. Although the diagnosis was confirmed by pathology, the results of treatment and management were nevertheless poor due to diffuse lymphangioma in mediastinum adjacent to big vessels and the heart where surgical removal and sclerotherapy could not be applied. The child was therefore treated with pleurectomy to control hemothorax, blood transfusion to control anemia and propranolol. Finally, he was discharged home.
Conclusion
In pediatrics, lymphangiomatosis is a rare condition of which the origin and pathogenesis are unknown. The spectrum of clinical symptoms varies depend on the affected tissues. Biopsy is the gold standard for diagnosis. Drug treatment by drugs is currently being researched so the management and the long term prognosis of this child are poor.
References
- Satria MN, Pacheco-Rodriguez G, Moss J (2011) Pulmonary Lymphangiomatosis. Lymphat Res Biol 9(4): 191–193.
- Faul JL, Berry GJ, Colby TV, Ruoss SJ, Walter MB, Rosen GD, et al., (2000) Thoracic lymphangiomas, lymphangiectasis, lymphangiomatosis, and lymphatic dysplasia syndrome. Am J Respir Crit Care Med 161(1): 1037–1046.
- Alvarez OA, Kjellin I, Zuppan CW (2004) Thoracic lymphangiomatosis in a child. J Pediatr Hematol Oncol 26(2): 136–141.
- Brodszki N, Länsberg JK, Dictor M, Gyllstedt E, Ewers SB, Larsson MK, et al., (2011) A novel treatment approach for paediatric Gorham-Stout syndrome with chylothorax. Acta Paediatr 100(11): 1448–1453.
- Fontanesi J (2003) Radiation therapy in the treatment of Gorham disease. J Pediatr Hematol Oncol 25(10): 816–817.
- Ozeki M, Fukao T, Kondo N (2011) Propranolol for intractable diffuse lymphangiomatosis. N Engl J Med 364(12): 1380–1382.
- DU MH, Ye RJ, Sun KK, Li JF, Shen DH, Wang J, et al., (2011) Diffuse pulmonary lymphangiomatosis: A case report with literature review. Chin Med J (Engl) 124(5): 797–800.
- Radhakrishnan K, Rockson SG (2008) The clinical spectrum of lymphatic disease. Ann NY Acad Sci 1131: 155–184.
- Henry D. Tazelaar (2016) Diffuse Pulmonary Lymphangiomatosis. National Organation for Rare Diseases.
- Meir Cohen, Gregory Gary Caputy (2015) Lymphatic Vascular Malformations.





