Burden of Care on Caregivers of Children infected with Human Immunodeficiency Virus in Calabar, Nigeria
Ochigbo SO1*, Oparah SK2, Torty C3
1 Faculty of Medical Sciences, Department of Paediatrics, University of Calabar, Calabar, Nigeria.
2 Faculty of Medical sciences, Department of Internal Medicine, University of Calabar, Calabar, Nigeria.
3 Department of Paediatrics, University of Calabar Teaching Hospital, Calabar, Nigeria.
*Corresponding Author
Dr. Sunday Oteikwu Ochigbo,
Faculty of Medical Sciences, Department of Paediatrics,
University of Calabar, Calabar, Nigeria.
Tel: +2347063930682
E-mail: ochigbosunny@gmail.com
Received: November 21, 2018; Accepted: December 18, 2018; Published: December 19, 2018
Citation: Ochigbo SO, Oparah SK, Torty C. Burden of Care on Caregivers of Children infected with Human Immunodeficiency Virus in Calabar, Nigeria. Int J AIDS Res.
2018;5(3):177-180. doi: dx.doi.org/10.19070/2379-1586-1800034
Copyright: Ochigbo SO© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
An estimated 13.4 million children and adolescents worldwide had lost one or both parents to AIDS as of 2015. Family members, relatives or foster parents and other caregivers who may have other challenges are left to care for the children. Caregivers burden is dependent on the caregiver’s overall health, financial, physical, psychosocial, and spiritual wellbeing. This study was therefore conducted to determine the effect of these burdens on caregivers of HIV infected children. This analytical cross-sectional study involved the interview of caregivers, which we defined as, any unpaid layperson willing to participate, whom the patient himself/herself identified as being close, share illness experience and play supportive role. Data was collected using the Zarit Burden instrument. The p-value <0.05 was considered to be significant.
One hundred and ten (110) caregivers were studied; their mean age was 35.92 (±10.18) years. Generally, 76.4% of the caregivers had minimal burden while 16.4% had mild to moderate burden. Approximately 5.4%, and 1.8% of the caregivers had moderate and severe burden respectively. The variables studied had some varied effect on the caregivers but none was statistically significant.
Routine screening by health care professionals dealing with HIV infected children would help to expose existing caregivers burden and promote the provision of appropriate need driven support. Establishment of caregivers counseling and support groups in healthcare facilities would mitigate some of the challenges.
2.Background
3.Subjects and Methods
4.Results
4.1 Socio-demography
4.2 Zarit burden interview
4.3 Relationship of Variables with Severity of Burden
5.Discussion
6.Conclusion
7.Recommendations
8.Acknowledgement
9.References
Keywords
Burden; Family; Well-Being; Health Care.
Background
Approximately 120,000 children died due to AIDS-related illnesses in 2016. This equates to 328 deaths every day [1]. An estimated 13.4 million children and adolescents (0-17 years) worldwide had lost one or both parents to AIDS as of 2015. More than 80% of these children (10.9 million) live in sub-Saharan Africa [2]. In addition, millions more children are indirectly affected by the impact of the HIV epidemic on their families and communities [3].
One of the most devastating impacts of HIV is the loss of whole generations of people in communities hardest hit by the epidemic. In this regard, it is often children who feel the greatest impact via the loss of parents or older relatives. The children are therefore at the mercy and care of relatives or foster parents who may have other challenges to handle in addition to caring for the ill HIV infected or affected child. While providing care and treatment, the entire focus is sometimes on these children the needs and demand of other family members are often overlooked and neglected. The vital role played by such family caregivers is well recognized but burden on them is poorly understood [4]. Zarit et al., have defined caregiver burden as: “The extent to which caregivers perceive that care given have adverse effect on their emotional, social, financial, physical, and spiritual functioning”[5]. Caregivers burden is dependent on a host of variables while providing care to a seriously ill family member. This compromises the caregiver’s overall health, financial, physical, psychosocial, and spiritual wellbeing.
Anecdotal experience from our center revealed missed clinic appointments by caregivers possibly due to some challenges and competing needs. Hence, this study was conducted to critically examine the experiences and burden of caring for HIV infected children. This is expected to provide better understanding of the challenges experienced by caregivers and advise on coping strategies.
Subjects and Methods
This analytical cross-sectional study was carried out at the Children Outpatient Clinics (CHOP) and Children ward of the University of Calabar teaching hospital, Calabar, Nigeria. The study was conducted over a period of six months from January-June, 2017. The study population comprised of the child’s parents, family caregivers, which we defined as, any layperson, who was unpaid and willing to participate, whom the patient himself/herself identified as being in a close supportive role, and sharing most of his/her illness experience. The study process was explained to the parents, guardian or caregivers of each child, informed consent and ethical approval were obtained from caregivers and the institution respectively. The interviewer administered semistructured questionnaire and the burden of care was measured using the Zarit Burden data instrument. It is a 22-item Likert scale, which assesses five main domains of burden namely health, psychological wellbeing, finances, social life and relationship with the patient. The final scores range is from 0 to 88. It is stratified into four categories, that is, a score of 0-20 indicates no or minimal burden, 21-40 mild to moderate burden, 41-60 moderate to severe burden and 61-88 indicates severe burden. Non-participation in the study did not affect the care provided to the patient. The ethical committee of the institution approved this study.
Data collected was analyzed using SPSS Version 22 statistical software. For continuous variables, the mean, standard deviation and degree of freedom were calculated. Categorical variables were presented as simple proportions and percentages. The p-value <0.05 was considered to be significant.
A total of 110 caregivers were interviewed. Caregivers had mean age of 35.92 (±10.18) years, with most of them in the age range of 40-49 years. Women and men accounted for 81.8% and 18.2% of the caregivers respectively. More than three-fourth of the caregivers were married, 18.1% unmarried and 5.5% widows. More caregivers (43.6%) had tertiary education and only 1.6% without formal education. Ninety percent of the caregivers were Christians and 71% of our study population tested positive to HIV. Majority (83.6%) of the caregivers and the children lived together. Approximately 87.3% of the caregivers were biological parents of the children while the rest were grandparents(3.6%), family relations (8.2%), and neighbors 0.9%. Most of the children who received care were less than five years <3 years (54.5%); 4-5 years (32.7%); and >5years (12.8%). (Table 1)
Generally 76.4% of the caregivers had no or minimal burden while 16.4% had mild to moderate burden. Approximately 1.8% of the caregivers had severe burden. (Table 2)
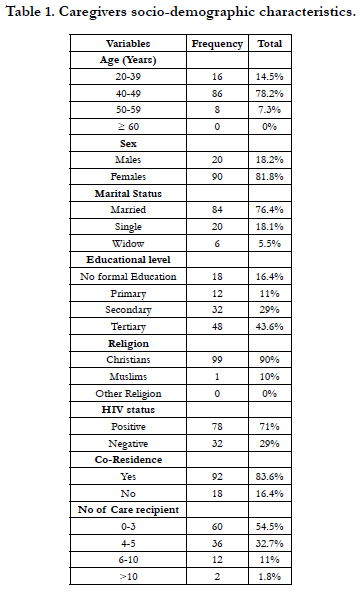

Table 1. Caregivers socio-demographic characteristics.
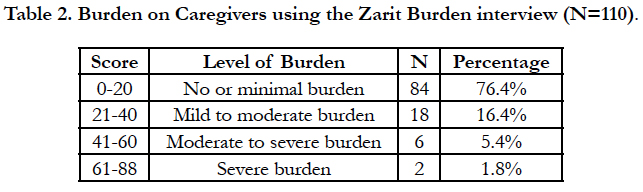
Table 2. Burden on Caregivers using the Zarit Burden interview (N=110).
Majority (72.7%) of the caregivers who did not disclose their status had little to moderate burden. Two of those who disclosed their status had severe burden (p=0.096). More caregivers who were absent from their places of work had moderate and severe burden. In our study 64, 14 and 2 of the respondents who were married, and 14, 6 and none of the unmarried respondents, had none or minimal burden, mild to moderate burden and severe burden respectively (p=0.157). The females have more burden than males; also those caregivers who were educated showed more degree of burden. Among those who had given care for more than 5 years, 6 of them had mild to moderate burden and none had severe burden. On the other hand, 22 and 2, of those who had given care for 5 years and below, had mild to moderate and severe burden, respectively (p = 0.199).
The care givers who could not ascertain their monthly income as well as those who earned <10,000 Naira were more and they had little or no burden compared to those with income ranging between 10,000-20,000 Naira (p=0.199). The non-biological parents of the children had severe burden compared to the rest. The caregivers with support had less burden compared to those who received support (p=0.157). In addition 39 and 2 of the caregivers who had less than five children under their care had mild to moderate and severe burden, respectively, compared to 9 and 3 of those who had more than 5 children in their care (p= 0.096). (Table 3)
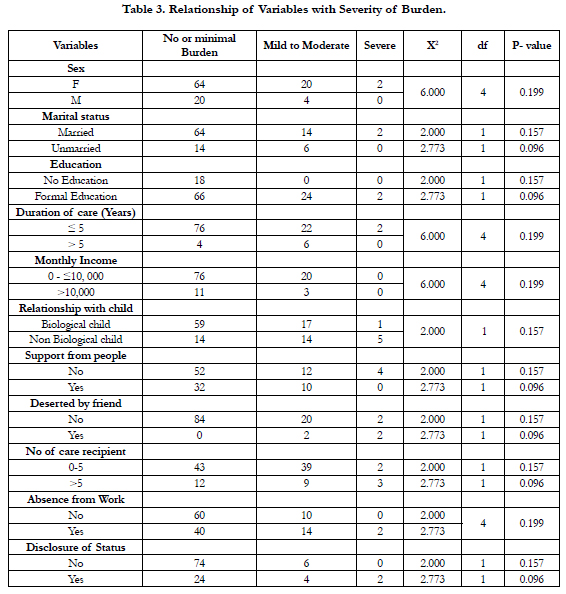
Table 3. Relationship of Variables with Severity of Burden.
Discussion
Approximately 5.4% of the caregivers in this study experienced moderate to severe burden. Singh et al., in South Africa corroborated this low percentage. This is at variance with other studies [6, 7]. Asuquo et al., [8] in Calabar Nigeria observed that majority of the caregivers had moderate to severe and severe burden to be 36% and 25% respectively though among caregivers of adults PLHIV. Studies have shown that risk factors for caregivers burden include female gender, low educational status, residing with the patient, depression, social isolation, and lack of choice in being a caregiver [9, 10]. The minimal burden observed in our study may not be unrelated to the short duration of care, few numbers of children under care. In addition, the majority of the children were the biological children of the caregivers. Most literatures have highlighted the physical, social and emotional impact on caregivers of HIV infected children [11]. It is also documented that caregiving have features of chronic stress experience [12].
In Africa, the burden of caregiving is the traditional role of women as social norms and expectations. However, various studies have reported that men do not take the role of informal caregivers except in situations where there are no women available to do so. This is in keeping with our study where older women compared with the younger age groups were mostly the caregivers. This is may be due to the fact that observed age range may have become grand mothers and step in as caregivers of relations’ children whose parents may have died of AIDS. The high burden observed among married couples might not be unrelated to the competing family needs that eventually put enormous stress on the woman and family finances. Increased caregiver burden and continued drain on the financial resources heightened the perception of burden [13]. Caregiver characteristics that might influence outcomes include age, gender, socioeconomic status, duration of caregiving and family relationship between the patient and the caregiver [14]. Though most of caregivers studied were not literate and in low socioeconomic status, but in contrast to other studies [15] had minimal burden that was not statistically significant. This may be due to the additional support received from their spouses. In addition, coping and adaptive skills by African female caregivers may account for this observation [16].
The burden of care did not adversely affect the caregivers from their workplaces and businesses. This can be attributed to the fewer children in care as well as support rendered by family, relations and friends. In Nigeria and Africa as whole communal living and assistance is part of the African culture. Disclosure of status to a close friends or relatives is expected to relieve or decrease burden as well as provide better psychological adjustments on caregivers [17]. In this study, 24% of the caregivers disclosed and this did not decrease the burden experienced by caregivers. Conversely, 5% of those who disclosed had severe burden, though not statistically significant. This may be attributed to possible rejection from stigmatization and discrimination [18, 19].
Conclusion
A minimal level of burden was observed among caregivers. The variables studied did not have statistically significant effect on the burden of caregivers.
Recommendations
Routine screening for caregivers burden by health care professionals dealing with HIV infected children would help expose existing caregiver burden and promote the provision of appropriate need driven support. Establishment of caregivers counseling and support groups in healthcare facilities would mitigate some of the challenges. Further studies on this subject with larger sample are recommended.
Acknowledgement
The authors would like to acknowledge Mr. Edom Awara of the department of pediatrics, University of Calabar Teaching Hospital, Calabar for his assistance during the data collection for this study.
References
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Ending AIDS: Progress towards the 90-90-90 targets. Global AIDS Update. 2017.
- UNICEF. For every child, end AIDS–seventh stocktaking report. New York: UNICEF. 2016.
- UNAIDS. Children and HIV Fact sheet. 2016.
- Grunfeld E, Coyle D, Whelan T, Clinch J, Reyno L, Earle CC, et al. Family caregiver burden: results of a longitudinal study of breast cancer patients and their principal caregivers. CMAJ. 2004 Jun 8;170(12):1795-801. PubMed PMID: 15184333.
- Zarit SH, Todd PA, Zarit JM. Subjective burden of husbands and wives as caregivers: a longitudinal study. Gerontol. 1986 Jun;26(3):260-6. PubMed PMID: 3721233.
- Lee SJ, Li L, Jiraphongsa C, Rotheram‐Borus MJ. Caregiver burden of family members of persons living with HIV in Thailand. Int J Nurs Pract. 2010 Feb;16(1):57-63. doi: 10.1111/j.1440-172X.2009.01812.x. PubMed PMID: 20158549.
- Ugwuoke KA, Remmikat N. A Case Study of the Burden of Care among Caregivers of HIV/Aids Patients in Jos Prison, Nigeria. Inter J for Soc Studies. 2016;2;245-50.
- Asuquo EF, Etowa JB, Adejumo P. Assessing the relationship between caregivers burden and availability of support for family caregivers’ of HIV/ AIDS patients in Calabar, South East Nigeria. World Journal of AIDS. 2013 Dec 2;3(04):335.
- Adelman RD, Tmanova LL, Delgado D, Dion S, Lachs MS. Caregiver burden: a clinical review. JAMA. 2014 Mar 12;311(10):1052-60. doi: 10.1001/jama.2014.304. PubMed PMID: 24618967.
- Collins LG, Swartz K. Caregiver care. Am Fam Physician. 2011 Jun 1;83(11):1309-17. PubMed PMID: 21661713.
- Pearlin L, Mullan J, Aneshensel C, Wardlaw L, Harrington C. The structure and functions of AIDS caregiving relationship. Psychiatr Rehabil J. 1994;17(4):51-67.
- Schulz R, Sherwood PR. Physical and mental health effects of family caregiving. Am J Nurs. 2008 Sep;108(9 Suppl):23-7. doi: 10.1097/01.NAJ.0000336406.45248.4c. PubMed PMID: 18797217.
- Mushonga RP. Social support, coping and perceived burden of female caregivers of HIV/AIDS patients in rural Zimbabwe. 2005.
- Mupedziswa R. AIDS and older Zimbabweans: Who will care for the carers?. S Afri J of Gerontol. 1997 Oct;6(2):9-12.
- Sepulveda C, Habiyambere V, Amandua J, Borok M, Kikule E, Mudanga B, et al. Quality care at the end of life in Africa. BMJ. 2003 Jul 26;327(7408):209-13. PubMed PMID: 12881267.
- Mui AC. Caregiver strain among black and white daughter caregivers: A role theory perspective. Gerontologist. 1992 Apr;32(2):203-12. PubMed PMID: 1577316.
- Bachanas PJ, Kullgren KA, Schwartz KS, Lanier B, McDaniel JS, Smith J, Nesheim S. Predictors of psychological adjustment in school-age children infected with HIV. J Pediatr Psychol. 2001 Sep;26(6):343-52. PubMed PMID: 11490035.
- Paxton S. The paradox of public HIV disclosure. AIDS Care. 2002 Aug;14(4):559-67. PubMed PMID: 12204158.
- Rohleder P, Gibson K. “We are not fresh”: HIV-positive women talk of their experience of living with their spoiled identity. University of Cape Town; 2005.





