Perceptions Regarding HIV/AIDS and Risky Behaviours Among Prison Inmates in Southwest Region of Cameroon
Tarkang EE1,4*, Pietra V2, Adam A1, Fusheini A1, Kweku M1, Pencille L3,4
1 School of Public Health, University of Health and Allied Sciences, Ho, Volta Region, Ghana.
2 Institute of Infectious and Tropical Diseases, Faculty of Medicine, University of Brescia, Brescia, Italy.
3 Charlie Norwood VA Medical Center, One Freedom Way Augusta. GA 30904, USA.
4 HIV/AIDS Prevention Research Network Cameroon, Kumba, Southwest region, Cameroon.
*Corresponding Author
Elvis Tarkang,
HIV/AIDS Prevention Research Network Cameroon,
Kumba, Southwest region, Cameroon.
E-mail: ebeyang1@yahoo.com
Received: July 01, 2016; Accepted: October 22, 2016; Published: October 26, 2016
Citation: Tarkang EE, Pietra V, Adam A, Fusheini A, Kweku M, et al., (2016) Perceptions Regarding HIV/AIDS and Risky Behaviours Among Prison Inmates in Southwest Region of Cameroon. Int J AIDS Res. 3(8), 126-131. doi: dx.doi.org/10.19070/2379-1586-1600024
Copyright: Tarkang EE© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Prisoners are at exceptional risk of infection with HIV because of the association of injection drug use, tattooing, sex between men and unprotected sexual intercourse with incarceration. This study described the perceptions regarding HIV/ AIDS and risky behaviours among prison inmates in Kumba in the Southwest region of Cameroon.This was a cross sectional study, conducted among 232 male prison inmates in Kumba, in December 2015. Data were collected using a structured pretested questionnaire, and analysed using frequencies, percentages and Chi-square at the level 0.05, using SPSS version 20 software program. The majority, 178 (76.8%) were between the ages of 25 and 45 years; most, 133 (57.3%) had primary education and 184 (79.3%) were Christians. Most of them, 125 (53.9%) perceived that prison inmates are prone to HIV/AIDS, and only 44 (19%) perceived that condoms are available in the prison; 56 (24.1%) perceived that sterile objects are available in the prison; majority, 187 (80.6%) perceived that sexual intercourse exists in the prison, but only 39 (16.8%) perceived that condoms are used by inmates. Majority, 136 (58.6%) perceived that tattooing is practised in the prison, and 170 (73.3%) agreed that sexuality education should be provided in the prison. Being of a lower academic level was associated with an increased perception that prison inmates are prone to HIV/AIDS infection (P=0.030), and also associated with an increased perception that tattooing is being practised in the prison (P=0.034). These findings call for concerted efforts bystakeholders to implement strategies to improve the perceptions regarding HIV/AIDS, and to eliminate risky behaviours among prison inmates that might expose them to HIV infection.
2.Introduction
3.Methods
3.1.Study Site
3.2.Study Design
3.3.Ethical Considerations
3.3.Data Collection Instrument
3.3.Data Analysis
4.Results
4.1.Socio-Demographic Characteristics of the Prison Inmates
4.2.Perceptions Regarding HIV/AIDS and Risky Behaviours of Inmates
4.3.Associations between Socio-Demographic Characteristics, Perceptions Regarding HIV/AIDS And Risky Behaviours
5.Discussion
6.Limitation
7.Conclusion and Recommendation
8.References
Keywords
Perceptions Regarding HIV/AIDS; Risky Behaviours; Prison Inmates; Urban Cameroon.
Introduction
The situation of HIV in prisons is an issue which is often ignored and neglected. This is mainly because of the fact that prisoners are often the forgotten lot of the society. The stigma associated with HIV also means that prison inmates are often doubly victimized in terms of access to care and treatment [1, 2].
Prisons concentrate great numbers of HIV-infected and at-risk populations, while prisoners comprise one of the least represented populations in national HIV strategies. Several issues need to be considered with regard to HIV in prison settings. Prison inmates are at risk of contracting HIV because they engage in high-risk behaviours such as homosexuality, unprotected sexual intercourse, use of non-sterile contaminated injection equipment and tattooing [3]. This risk is aggravated by the prison conditions characterized by overcrowding, boredom and inadequate access to health services [4]. This phenomenon poses significant health concerns with regard to control of infectious diseases and HIV prevention and care [5]. A high proportion of prisoners around the world are sentenced for drug-related crimes, including trafficking. Many continue drug use while in prison. Injection drug use with contaminated equipment accounts for a large number of HIV cases in prisons on a worldwide basis [6].
The majority of prisoners are male; this is especially the case in Africa. Given this, the prison environment is highly conducive for violence and homosexuality, which are key factors driving the spread of HIV infection [7]. Given that force is exercised and that condoms are not used, victims of rape and other forms of sexual violence are at higher risk of contracting HIV [8].
Many inmates engage in high-risk behaviours before they are incarcerated. The lifestyles of many inmates prior to incarceration include unprotected sexual intercourse, drug and alcohol abuse, poverty, homelessness, under-education, and unemployment, all of which are associated with risk of HIV/AIDS. In both the free world and within the microcosm of society that prisons represent, these individuals disproportionately experience poor health outcomes as well as a high prevalence of HIV/AIDS and other infectious diseases, owing to numerous barriers and structural constraints [9, 10].
Although it is clear that most of these infections occurred in the community prior to incarceration, the lack of implementation of risk reduction programs in prison settings is a missed opportunity. Therefore incarceration offers an ideal opportunity for the delivery of health education programs and especially HIV prevention messages that focus on high-risk behaviors [9, 10].
Prisoners are often in close contact with the general population, thus making the prison population a significant vector of inward and outward transmission of HIV [9, 10]. Probably, a possible positive aspect to the issue of HIV in prison is the fact that within the prison premises, the inmates are a captive audience who may otherwise be hard to reach and may ordinarily avoid seeking health services especially related to HIV due to stigma, fear, and criminal policy. As a result, prisons present an opportunity for HIV prevention. Thus, it is essential to address the issue of HIV in prisons.
In prisons, health services are generally poor, ill equipped and understaffed, or non-existent. Universal precaution principles are often poorly applied.There is poor or no access to HIV and other STI prevention or treatment services. Access to voluntary counselling and testing and to HIV treatment are often nonexistent. Prevention commodities such as condoms, sterile needles and syringes, disinfectants for tattooing equipment and information are seldom available as they are perceived to be in conflict with drug laws, or laws which prohibit sexual relations between men or sexual intercourse in the prison. Lack of knowledge and education among prisoners about the risks of contracting and transmitting HIV, coupled with the absence of protective means and proper medical care increase their risks of HIV infection. The risk of infection is also increased for those in contact with members of prison populations such as prison staff and their spouses or partners, and by extension, the broader population.
Prisoners are largely dependent on prisons authorities for access to information about HIV, means of protection, and health services as a whole. There are few HIV-related services provided by the public sector to the prisons [11].
HIV prevalence among most at risk populations (MARPs) in Cameroon is rising. Homosexual practices as found in the prisons is punishable by Cameroonian law and highly stigmatized. The Cameroon national strategic plan for HIV/AIDS 2011-2015 prioritizes incarcerated populations as critical targets in the fight against HIV. The plan identifies the following as gaps in coverage for MARPs: serologic and behavioural surveillance, targeted behaviour change communication (BCC), access to voluntary counselling and testing (VCT) and accessible care and treatment services [12].
The estimated HIV/AIDS prevalence rate among prisoners in Cameroon is 12%. Occupancy rates reflect high levels of overcrowding, which ranges between 300 and 345 % above planned levels. In Cameroon, the prison population rate is 125 per 100,000 persons, giving a total prison population of over 20,000 persons [13].
Generally there is paucity of data on HIV/AIDS in prison in Cameroon as in other parts of Africa, which makes it difficult to undertake adequate and successful prevention interventions. This study was aimed at describing the perceptions regarding HIV/AIDS and risky behaviours among prison inmates in the Southwest region of Cameroon.
Methods
There are currently 73 prisons in Cameroon, which are divided into three main categories: central prisons, located in the capital city of each region; principal prisons, which are linked to magistrates courts accommodating all categories including pretrial prisoners; and, secondary prisons that only accommodate sentenced prisoners and are scattered throughout the country. As its name suggests, the Kumba Principal Prison is of the second type, and is located in the city of Kumba in the Southwest Region of Cameroon, an Anglophone region that applies the common law-based Penal Code [13]. It serves the purpose of providing remand centres especially for those whose cases are going on in courts within the area and those who have been sentenced for various crimes. The “awaiting trial cell” housed nearly three hundred detainees in an area less than 18 x 20 meters square, and there is lack of medical facilities and drugs for which there is a budget.
The study was a descriptive cross-sectional survey conducted in December 2015. The total number of inmates in the prison during the study period was about 500 comprising mostly males. A total of 232 male inmates were recruited for the study after calculating the sample size assuming that 40% ofinmates had realistic perceptions about HIV in prison, using the formula n=Z2pq/d2 and 10% degree precision at 95% confidence interval [14]. Simple random sampling method was used to select a sample of 232 respondents using the full list of inmates available with the prison authorities at the time of the survey. None of the selected male respondents declined to participate in the study. Since a great majority of the inmates were males and the number of females was very insignificant to draw statistical comparisons, only male inmates were recruited for the study.
Permission was obtained from the Kumba prison authorities before data collection took place. Written informed consent was also obtained from the inmates by signing of the consent forms after the contents of the form had been clearly explained to them. They were also told that the study was voluntary and that individuals who agreed to participate will be allowed to withdraw from the study at any stage of the research.
The instrument for data collection was a pretested structured self-administered questionnaire. A pretest of the instruments was carried out with 20 inmates with similar socio-demographic characteristics as those of respondents. The questionnaire was adopted from knowledge, attitudes, perceptions, and practices survey of previous HIV/AIDS studies [15, 16]. The questionnaire comprised questions and items regarding socio-demographic profile, perceptions regarding HIV/AIDS and risky behaviours of the respondents. The questionnaire was written in English.
The questionnaires were administered by trained research assistants of the HIV/AIDS Prevention Research Network Cameroon (HIVPREC), in private rooms made available by the prison authorities.The research assistants received a one-day training on how to use the questionnaire. The researcher spent about two hours with the prison inmates to explain to them the nature of the study. The research assistants were there to clarify and answer questions posed by the respondents and to make sure that the questionnaires were completely filled. Strict confidentiality was maintained. All the respondents completed the questionnaires, and no incentives were given nor coercive strategies used to lure them into responding to the questionnaires.
The data collected were transcribed and translated where appropriate; coded and then analysed using Statistical Package for Social Sciences (SPSS) version 23.0 software program.Comparisons were carried out using cross-tabulations and Pearson Chi-Square where appropriate at the level 0.05.
Results
Of the 232 respondents in this study, the majority, 178 (76.8%) were between the ages of 25 and 45 years, with most of them, 141 (60.8%) being married. One hundred and eighty four (79.3%) were Christians and the majority, 133 (57.3%) had primary education (Table 1).
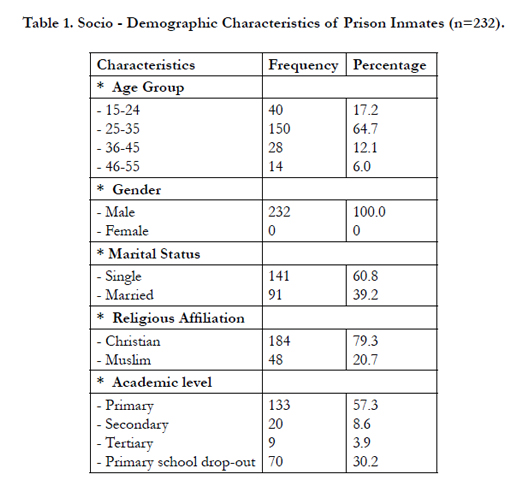

Table 1. Socio - Demographic Characteristics of Prison Inmates (n=232).
Of the respondents, a slight majority, 125 (53.9%) perceived that prisoners are prone to HIV/AIDS; most, 136 (58.6%) perceived that tattooing is practised in the prisons, and only few, 56 (24.1%) perceived that sterile objects are available in the prisons; most, 187 (80.6%) perceived that sexual intercourse exists in the prisons; only 44 (19%) perceived that condoms are available in the prisonsand only 39 (16.8%) perceived that condoms are used by inmates during sexual intercourse. However, majority, 170 (73.3%) agreed that sexuality education should be provided in the prisons (Table 2).
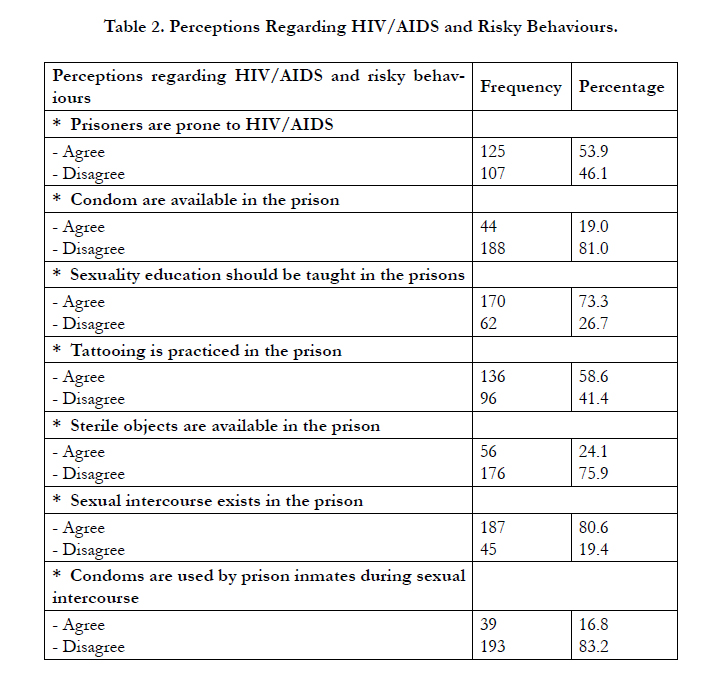
Table 2. Perceptions Regarding HIV/AIDS and Risky Behaviours.
- Being a Christian was associated with an increased perception that sexuality education should be provided in the prisons (P=0.033).
- Being of a lower academic level was associated with an increased perception that prison inmates are prone to HIV/AIDS infection (P=0.030).
- Being of a lower academic level was associated with an increased perception that sterile objects are available in the prisons (P=0.034).
- Being of a lower academic level was associated with an increased perception that tattooing is being practised in the prisons (P=0.034) (Table 3).
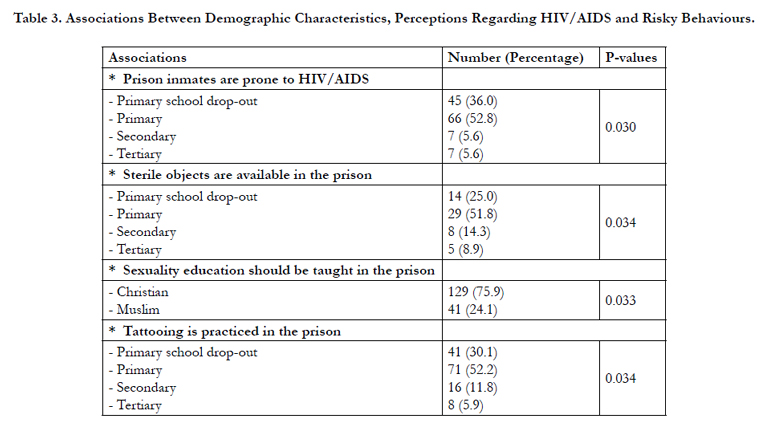
Table 3. Associations Between Demographic Characteristics, Perceptions Regarding HIV/AIDS and Risky Behaviours.
Discussion
This study demonstrated inadequate perceptions regarding susceptibility of prison inmates to HIV/AIDS transmission, and risky practices among prison inmates that might expose them to the risk of HIV/AIDS infection.
The socio-demographic characteristics of the prison inmates in this study showed 87.5% secondary school dropout rates before incarceration. These characteristics are comparable to reports from other studies in Nigeria [17]. The identified age bracket (25- 35 years) in this study where majority of the inmates fall, is of great concern to transmission of HIV as similar studies report that they are the most sexually active age group as well as the ones most likely to involve in risky sexual and nonsexual practices [17, 18].
In this study, only a slight majority of the inmates, 53.9% perceived that prison inmates are prone to HIV/AIDS, while most, 81.0% perceived that condoms are not available in the prison. The majority, 80.6% perceived that sexual intercourse exists in the prison, and most, 83.2% perceived that condoms are not being used by inmates during sexual intercourse in the prison. These perceptions and practices might expose prison inmates to the risk of contracting HIV/AIDS. Inmates who perceive that they are not prone to HIV/AIDS, might not see the need of engaging into protective behaviours such as condoms use during sexual intercourse, or not sharing sharp objects such as syringes or razor blades. In the same vein, inmates who perceive that condoms are not available in the prison might be forced to practice unprotected sexual intercourse, thereby exposing themselves to the risk of HIV transmission. This perception of condoms not being available in the prison is supported by the fact that majority of the inmates (83.2%) perceived that condoms are not being used by prison inmates during sexual intercourse.
Apart from the fact that HIV/AIDS can originate from the prison, there might be instances where prisoners bring HIV into the prison by engaging in risky behaviours outside the prison prior to incarceration. There is a much higher likelihood of new prisoners introducing HIV/AIDS to the existing non-infected prison population.
Prison populations are predominantly male and most prisons are male-only institutions, including the prison staff. In such a gender exclusive environment, male-to-male sexual activity (prisoner-toprisoner and guard-to-prisoner), which is culturally, religiously and politically unacceptable by most societies, is frequent [19, 20]. The actual number of instances is likely to be much higher than what is usually reported mainly due to continual denial, fear of being exposed or the criminalization of sodomy and homosexuality in Cameroon.
While much of the sex among men in prisons is consensual, rape and sexual abuse are often used to exercise dominance in the culture of violence that is typical of prison life [21]. Inmate rape, including male rape, is considered one of the most ignored crimes. Sexual and physical abuse in prison custody remains a tremendous human rights problem [22]. Some inmates are lured by other inmates to have consensual anal intercourse in exchange for food and toiletries probably due to lack of basic sanitary materials and adequate nutrition in prison [18, 23, 24]. The majority of inmates who engage in homosexual activities in the prisons are actually circumstantial homosexuals who would not have become involved in the practice if they were not confined [25].
These sexual encounters are fraught with the risk of contracting HIV because of the frequent tearing of sensitive anal membranes. Despite the necessity of providing targeted HIV prevention interventions for prison inmates, institutional and access barriers such as condoms, may impede the development and evaluation of such programmes. HIV prevalence in the prisons is usually higher than that in the population at large. It could be 5, 6, or even as much as 10 times higher than the values obtained in the general population [26]. Issues regarding condom use are important areas of interest in HIV prevention strategies in the prison.
Homosexuality is, therefore, a common sexual practice in the prison as mentioned by majority of the respondents in this study. In Cameroonian prisons as in other countries, same sex practices are made possible because inmates of the same sex sleep together in the same cell due to overcrowding which militate against the HIV/AIDS and tuberculosis prevention campaign. There is the risk of higher rate of HIV transmission in homosexuals compared with heterosexuals, and prisoners engaging in homosexuality are capable of transmitting HIV infection more than those who are not.
Tattooing and other forms of skin piercing are frequent among prisoners. Blood brotherhood rituals, involving blood exchange and the mixing of blood also occur, carrying a high risk of HIV transmission. One of the major risk factors for HIV infection among prison inmates is tattooing [3]. Education of stan¬dard recaution is, thus, of vital importance.
Most of the respondents in this study, 75.9% perceived that sterile objects are not available in the prison and majority, 58.6% also perceived that tattooing is being practised in the prison. These results are in agreement with other studies in Nigeria, which report use of non-sterile needles and other cutting instruments in the prison [27]. Some prison inmates who are professional barbers use unsterilized barbing instruments to barb prisoners because they might be unaware of the need for sterilizing these instruments [28].
The common high risk behaviours in the prison environment as perceived by the respondents in this study include practice of tattooing, unprotected sex, violence, rape, sexual assault, and sex among inmates (mostly anal and between males) [29]. These suggest significantly high risks behaviours that might expose prison inmates to the risk of contracting HIV/AIDS.
In this study, being of low academic level was associated with increased perceptions that prison inmates are prone to HIV infection and that sterile objects are available in prison. This misperception that sterile objects are available in prison could lead inmates with low academic level into the use of non-sterile objects, which might expose them to HIV transmission. This is reflected in this study because being of low academic level was also associated with increased perception that tattooing is being practised in the prison. This implies that most of the tattooing is being practised by inmates with low academic level, with the use of non-sterile tattooing equipment. These findings call for concerted efforts by the government and other stakeholders to develop and implement strategies, in the form of sexuality education or HIV policy for Cameroon prisons, in order to reduce or eliminate these risky practices that might expose prison inmates to HIV transmission.
Limitation
The study was limited by being done in only one prison due to logistics and financial constraints; however the findings in this study are expected to give an insight into what prevails in other prisons in Cameroon. Equally, the non-inclusion of female prisoners prevented gender comparison. Furthermore, since the manner in which the data was collected assumes HIV/AIDS originated in the prison, there might be instances where prisoners bring HIV into the prison by engaging in risky behaviour outside the prison prior to incarceration. This is a major point that has the potential to greatly bias the results. There is a much higher likelihood of new prisoners introducing HIV/AIDS to the existing non-infected prison population.
Conclusion and Recommendation
Most of the inmates perceived that tattooing is being practised in the prison and that sexual intercourse exists in the prison. These, notwithstanding, most of them also perceived that sterile objects for tattooing and condoms for prevention of sexual transmission of HIV/AIDS, were absent in the prison. These situations might increase the risk of inmates to the transmission of HIV/ AIDS. Efforts should be made by Cameroon government to comply with United Nations Committee on crime prevention and control that recommends that each prison inmate should be made to occupy by night, a cell or room by himself or herself [30]. The Cameroon prison administration should also ensure greater access to education on HIV/AIDS and condoms for prison inmates. The sharing of sharp objects for tattooing and shaving instruments like razor blades should be discouraged in the prison to prevent the spread of HIV among inmates through contaminated instruments. Further research needs to be conducted to distinguish between perceptions of infected new prisoners and perceptions of non-infected prisoners, and also perception of participants’ own risk behaviours.
References
- Goyer KC (2003) HIV/AIDS in Prisons: Problems, Policies, and Potentials. ISS Africa.
- Taiwo OO, Bukar A (2006) Knowledge and attitude of prisoners towards HIV/AIDS infection. RCORTI. 1(1): 31–34.
- WHO (2001) Health in Prisons.www.euro.who.int/__data/assets/ pdf_file/0009/99018/E90174.pdf
- Walmsley R (2003) Global Incarceration and Prison Trends. Forum on Crime and Society. 3(1-2): 65-78.
- Kantor E (2006) HIV Transmission and Prevention in Prisons. UCSF.
- Martin V, Cayla JA, Moris ML, Alonso LE, Perez R (1998) Predictive factors of HIV infection in injection drug users upon incarceration. Eur J Epidemiol. 14(4): 327-331.
- Curtis M (2004) Fighting for Prison Health. Newsletter of the International Harm Reduction Development Program of the Open Society Institute.
- Price J (1995) Inmate’s Lawsuit Point Up HIV Infection by Prison Rapes.
- Wohl AR, Johnson D, Jordan W, Lu S, Beall G, et al., (2000) High-risk behaviors during incarceration in African American men treated for HIV at three Los Angeles public medical centers. J Acquir Immune Defic Syndr.24(4): 386–392.
- Braithewaite RL, Arriola KRJ (2003). Male prisoners and HIV prevention: a call for action ignored. American Journal of Public Health 93(5): 759-763.
- Goyer KC, Gow J (2002) Alternatives to current HIV/AIDS policies and practices in South African prisons. J Public Health Policy. 23(3): 307-323.
- Pepfar (2011) Cameroon operational plan report FY 2011.
- International Centre for Prison Studies (2007) The World Prison Population List.
- Taofeek I (2009) Research Methodology and Dissertation writing for Health and allied Health professionals. (1st Edn), Cress global link limited publishers, Abuja.
- Sabitu K, Iliyasu Z, Joshua IA (2009) An assessment of knowledge of HIV/ AIDS and associated Risky Behavior among inmates of Kaduna convict prison, the implications for prevention programs in Nigerian prisons. Niger J Med. 18(1):52-58.
- Tarkang EE (2009) Knowledge, attitudes and perceptions regarding HIV/ AIDS and sexual behaviours among senior secondary school learners in Kumba, Cameroon. Unpublished doctoral thesis, University of South Africa,Pretoria, South Africa.
- Audu O, Ogboi SJ, Abdullahi AU, SabituAbah KER, Enokela OP (2013) Sexual risk behaviour and knowledge of HIV/AIDS among male prison inmates in Kaduna State, North Western Nigeria. Int J Trop Dis Health. 3(1):57–67.
- Susan C (2007) Impact a decade of global leadership and innovation. Final report on implementing AIDS prevention and care project; 1977-2007. Family Health Int. (FHI): 1-66.
- Human Rights Watch (2002) World Report. Special Programs and Campaigns- Prisons.
- IkuteyijoOL, Agunbiade MO (2008) Prison reforms and HIV/AIDS in selected Nigerian prisons. J Int Soc Res. 1(4): 279–289.
- Human Rights Watch (2001) No Escape: Male Rape in USA Prisons.
- Amnesty International USA. (2001) Abuse of Women in Custody: Sexual Misconduct and Shackling of Pregnant Women : a State-by-state Survey of Policies and Practices in the U.S.A. Amnesty International Publications,USA.
- Joshua IA, Ogboi SJ (2008) Seroprevalence of HIV amongst inmates of Kaduna prison, Nigeria. Sci world j. 3(1): 17-19.
- Olugbenga-Bello AI, Adeoye OA, Osagbemi KG (2013) Assessment of the reproductive health status of adult prison inmates in Osun State, Nigeria. Int J Reprod Med. 2013: 451460.
- Olusegun LI, Melvin OA (2008) Prison Reform and HIV/AIDS in selected Nigeria Prisons. Int J Soci Res. 1(4): 279-289.
- Malignity E, Alvarez GB (1998) Preventive HIV/AIDS education for prisons. Proceedings of the 12th International Conference on AIDS. Geneva, Switzerland. 1018.
- Hutin Y, Hauri A, Chiarello L, Catlin M, Stilwell B, et al., (2003) Best infection control practices for intradermal, subcutaneous, and intramuscular needle injections. Bull World Health Organ. 81(7): 491–500.
- Population Services International, Metrics Nigeria (2010) HIV/AIDS TRaC study evaluating behavior among risk groups in Nigeria Prisons Service. Roud one, PSI TRaC Summary Report.
- Labo HS (2002) A rapid assessment of the Knowledge, Attitude and Practice on HIV/AIDS and seroprevalence amongst staff and prisoners in paramilitary services survey in the Nigerian Para-Military.
- United Nations (2014) First United Nations Congress on the Prevention of Crime and the Treatment of the Offenders: standard minimum rules for the treatment of prisoners.





