Barriers Access to HIV Testing and Treatment Services in the District of Purba Medinipur, West Bengal; India – Focus Group Discussion
Biswas DK1*, Bhunia R2, Basu M3, Mishra A4
1 Dy. Chief Medical Officer of Health-II, District: Purba Medinipur, West Bengal, India.
2 District Maternal and Child Health Officer, District: Howrah, West Bengal, India.
3 Associate Professor (Community Medicine), Institute of Post Graduate Medical Education and Research (IPGMR) & SSKM Hospital, Kolkata- 20,
West Bengal, India.
4 Manager, Social Development and Infrastructure, National Urban Livelihood Mission, Haldia Municipality, PO: Debhogh, Dist: Purba Medinipur,
West Bengal, India.
*Corresponding Author
Dr. Dilip Kumar Biswas,
Dy. Chief Medical Officer of Health-II,
District: Purba Medinipur, Pin: 721636, West Bengal, India.
Tel: +919433200804
E-mail: dilipbiswas29@gmail.com
Received: August 15, 2016; Accepted: September 07, 2016; Published: September 09, 2016
Citation: Biswas DK, Bhunia R, Basu M, Mishra A (2016) Barriers Access to HIV Testing and Treatment Services in the District of Purba Medinipur, West Bengal; India – Focus Group Discussion. Int J AIDS Res. 3(7), 119-125.DOI : dx.doi.org/10.19070/2379-1586-1600023
Copyright: Biswas DK© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Services provided on HIV testing, treatment and care toward clients were not adequate in the district of Purba Medinipur. We aimed to recognize those barriers and recommended for improvement of utilization of HIV related services.
Method: Focus group discussion (FGD) were conducted among the homogenous groups of female sex workers (FSW), migrant labourers, truckers, peer educators (PE) and people living with HIV/AIDS (PLHA) of the district of Purba Medinipur between February and April 2013.
Result: Fifteen FGDs were carried out involving 151 participants. The mean age of the participants were 33.68 years with range from 18 – 57 years. More than 60% (91) were female participants. Migrant labourers and truckers had no adequate knowledge about HIV prevention, they did not know about Integrated Counseling & Testing Center (ICTC) services, Anti Retroviral Treatment (ART) services. Female Sex Workers (FSW) and People living with HIV/AIDS (PLHA) indicated long distance to attend ICTC, long distance and long waiting time at ART center. Short supply of ART medicines forced them frequent visit at ART center caused increased pocket expenditure. Participants mentioned about fear of disclosure of HIV positive status psychologically created negative influences on client’s mind which might reluctant to access HIV services. Most of participants indicated about discrimination in family, community and at working place due to HIV positive status.
Conclusion: Implement HIV care services for the vulnerable peoples at their close proximity and improving the quality of the existing health care delivery services would be helpful to overcome multiple barriers about utilization of services.
2.Introduction
3.Methodology
3.1.Study Population and study setting
3.2.Focus Group Discussion and Analysis Plan
3.2.Ethical Approval
4.Result
4.1.Study Population
4.2.Knowledge of HIV/AIDS
4.3.Sexual exposure, nature and degree of high risk behaviour
4.4.Barriers Experienced by Different Groups of People: (Table 3)
4.5.Stigma and discrimination influenced HIV services
5.Discussion and Recommendation
5.1.This study adds
6.Acknowledgement
7.References
Keywords
Barriers; HIV Services; West Bengal
Introduction
It was estimated in 2012 that 35.3 (32.2 – 38.8) million were lived with HIV and AIDS globally [1]. In India, estimated population living with HIV/AIDS in 2013 was 2.1 million (Range 1.7 – 2.7 million) with adult prevalence was 0.3% [1]. The epidemic situation in India was declining with 19% decline of new HIV infection (130000 in 2013) and reduction of AIDS related deaths 38% between 2005 and 2013 year [2]. High HIV prevalence state were South India like Andra Pradesh, Maharasthra, Karnataka and Tamil Nadu accounting 55% of HIV infection in the country; Whereas in West Bengal, Bihar, Gujarat and Uttar Pradesh were accounting 22% of HIV infection [3]. According to the prevalence of HIV infection among the antenatal mother and high risk population and smooth running the HIV/AIDS programme, National AIDS Control Organization (NACO) sub-classified all district of India into A, B & C category. A category means prevalence of HIV among antenatal mother > 1% and high risk population > 5%. B category district means prevalence of HIV among antenatal mother is < 1% and high risk population > 5% and C category means prevalence of HIV among antenatal mother < 1% and high risk population < 5%. The district Purba Medinipur was “B” category district [4]. HIV was mostly transmitted through heterogeneous route, unprotected paid sex, and higher incidence of HIV infection observed among certain population group [5]. ART programme launched in 2004 at the six high prevalence state and in 2013, there were around 18.13 lakh PLHA were registered at different ART center all over India [6]. Lack of knowledge of HIV, HIV testing, treatment & treatment centers, services of care, support and treatment (CST), low perception of personal risk of HIV among sex workers, truckers and migrant labourers were the main reason for not accessing HIV services [7].
Purba Medinipur was a vulnerable district for HIV transmission. There were tourist spots named Digha, Mandarmoni and Sankarpur sea beach, industrial area like Haldia petrochemicals and Haldia port, Kolaghat thermal power plant were situated (Figure 1). A large numbers of laborer were working there. National highways (NH) like NH 6 and 41 were passing through the district. The different kinds of sex tread were active such as brothel based sex worker, lodges based sex workers, and some were flying sex workers. They were continuing their sex tread in different places of the district. It was needed to provide services related to HIV prevention and treatment as well as regular check up for sexually transmitted diseases (STD). In order to understand the barriers of utilization of HIV services by the key population and to identify the strategies to overcome these barriers, we conducted the study.
The objectives of this study were:
- (a) To search the knowledge, experiences and barriers observed by the different groups of people while accessing HIV testing, ART services, care services to PLHA.
- (b) To provide recommendations to overcome these obstacles.
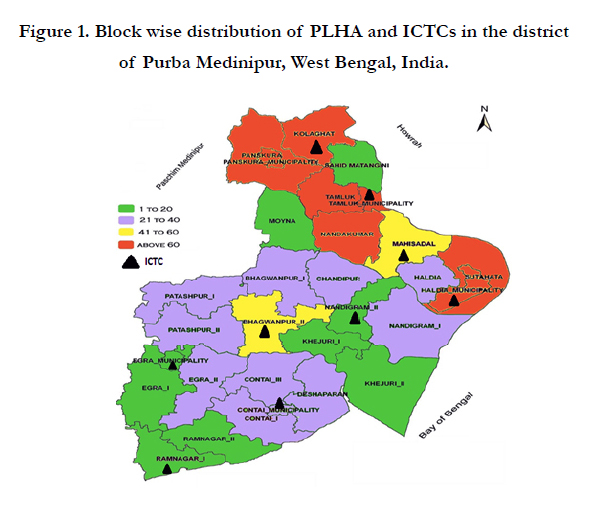

Figure 1. Block wise distribution of PLHA and ICTCs in the district of Purba Medinipur, West Bengal, India.
Methodology
Focus group discussions (FGDs) were conducted among different groups of people such as Female sex workers (FSWs), Migrant labours, Truckers, Peer Educators (NGOs staffs) and People Living with HIV & AIDS (PLHAs) in the district of Purba Medinipur in February and April 2013. Written consent was obtained from the individual participants before start of discussion. The participants were recruited purposefully with the help of Non-Government Organization (NGOs). Each FGD comprised with 6 – 14 participants. Ages of the participants were 18 years to 57 years. FSW were selected based on different types of FSW such as brothel based, lodged based, flying and street based. Migrant labour and truckers were recruited from the local industry at Haldia Petrochemical area of Purba Medinipur district.
Each FGD was lead by a moderator who was trained and he followed the guideline of the study. He was Master of Anthropology and skilled in local language. He was experienced in qualitative study. Before start of data collection one mock up round was conducted in presence of senior staff and was taught about data collection and recording. All FGDs were taken in a separate room using semi-structured in-depth interview in Bengali and Hindi as per situational need. The following aspects were discussed in the FGD such as (i) Socio-demographic status, (ii) Sexual exposure and high risk behaviour, (iii) Knowledge of HIV and AIDS, (iv) Barriers to access HIV testing and treatment services at ICTC, PPTCT and ART center, (v) Interpersonal factors, stigma and discrimination related to HIV & AIDS. Interview were recorded in Bengali and transcribed into English. Analysis of data was done with the perceived themes and ideas. The total duration of FGD was 90 minutes to 120 minutes. An honorarium of Rs: 100/- (One hundred) with a tiffin packet was served to the participants. Data was collected by the health workers engaged at the HIV/AIDS programme. Quantitative data was analyzed in excel software.
Administrative approval was obtained from the MD, NRHM, Government of West Bengal, and Department of Health & Family Welfare. Number was used instead of name to maintain confidentiality and anonymity.
Result
The district Purba Medinipur was “B” category district in respect of National AIDS Control Programme (NACP). Total Population of the district was 5102010 and overall literacy rate was 80% [8]. Every year more than 150 cases were detected at nine ICTCs in the district. A total 151 individuals were participated in 15 focus groups. Of which, 49 FSWs were participated from four focus groups such as 13 from brothel based FSWs, 12 from lodge based FSWs, 12 from flying FSWs and 12 from street based FSWs. Total 15 migrant labours were participated in two focus groups and 16 truckers were participated in two focus groups. Twenty one peer educators (PE) were participated with three focus groups. Fifty PLHAs were participated in four focus groups. The mean age of the participants were 33.68 years with range from 18 – 57 years. (Table 1) Sixty three percent (n=95) of the participants were married and 33% (n=50) of them were illiterate. Average monthly family income was Rs: 7088/-. Among the all groups, lodge based FSW had maximum average monthly income (Rs: 15000/-). (Table 2) We clubbed findings under several sub-heading to discuss the barriers at group level and interlinked with individual level. There were two link-ART centers in the district but had no ART center. The nearby designated ART center for the district was Midnapore Medical College and Hospital which was situated at Pachim Medinipur district and around 108 Kilometer away from the district head quarter. Patients had to go to Midnapore Medical College ART center for collection of medicines and CD4 cell count. In the last three years, around 35% of patient failed to collect medicines from the ART center.
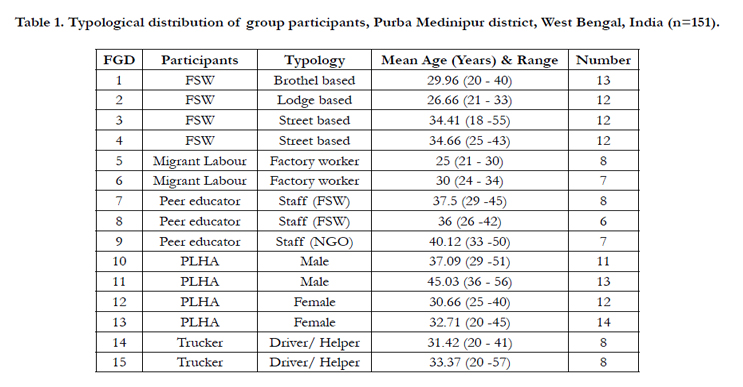

Table 1. Typological distribution of group participants, Purba Medinipur district, West Bengal, India (n=151).
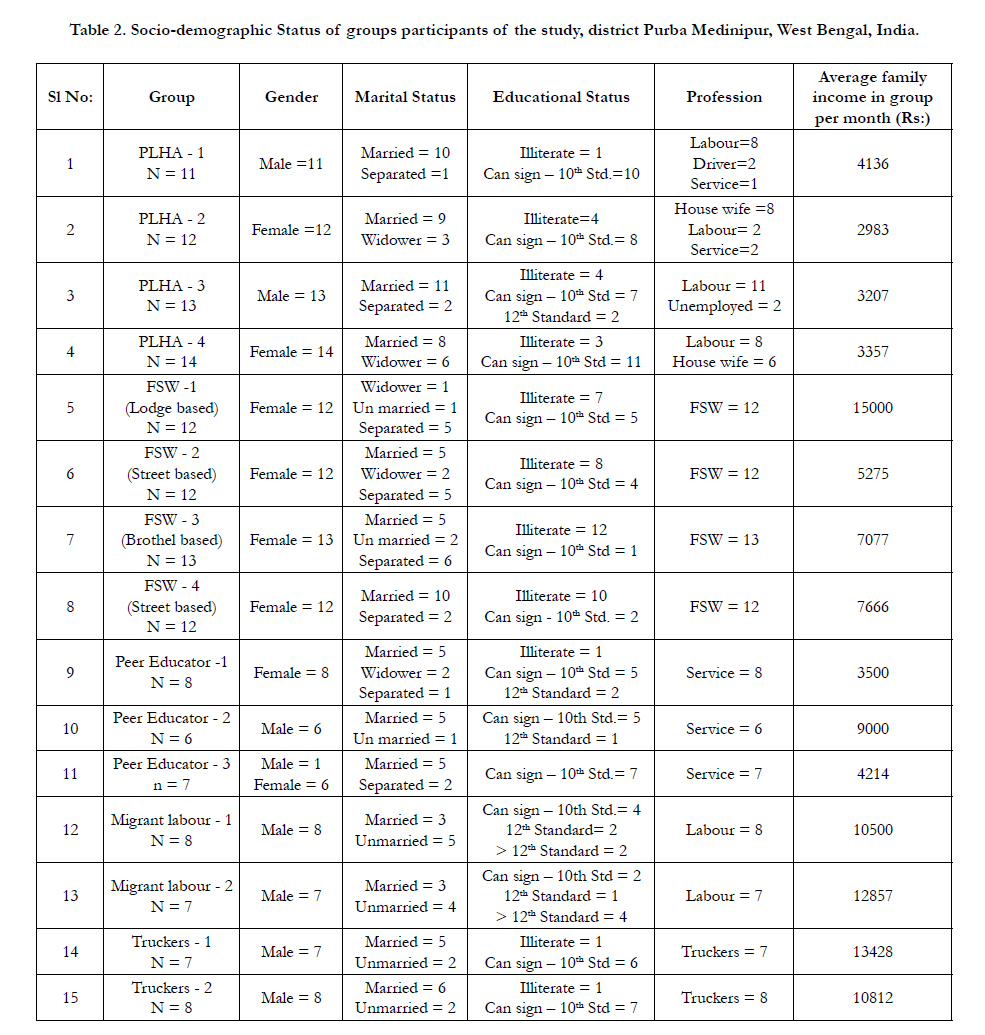
Table 2. Socio-demographic Status of groups participants of the study, district Purba Medinipur, West Bengal, India.
Most of the participants heard the name of HIV and AIDS and accurately indicated the vulnerability of HIV infection. But they had limited knowledge about HIV transmission and prevention. Truckers and migrant labour could not mention properly where HIV services were available.
FSW had different kinds of sex partner like truck driver, helper, business man to college students and many others. Most of them were used condom during sexual activities. So some client dissatisfied while used condom at sex. None of them practiced anal sex.
We analyzed the responses of different groups of people related to the following services provided.
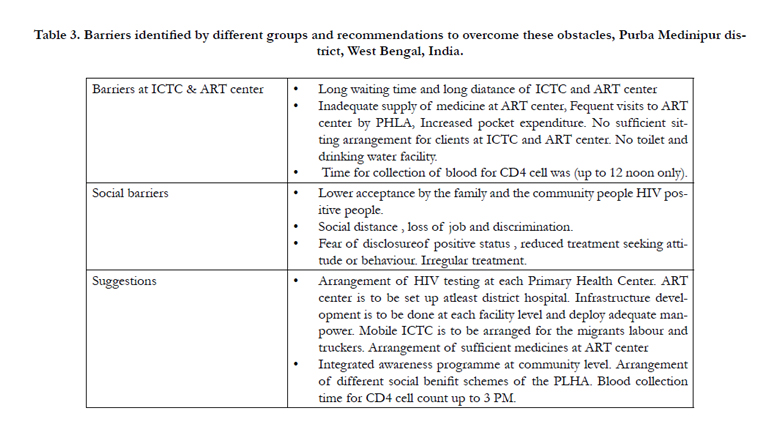
Table 3. Barriers identified by different groups and recommendations to overcome these obstacles, Purba Medinipur district, West Bengal, India.
Migrant labours and truckers indicated that they had limited time to attend at ICTC. Factory management does not release them at duty hour to attend the clinic. Truckers also had no scheduled time; they only stayed there for only loading and unloading of trucks. It takes at least three – four hours to complete counseling and testing services. So, they demanded mobile ICTC. One of the truck drivers mentioned as:
“I stayed at the port area for a short time. I have to look after my vehicle whether loading and unloading is completed or not. It is impossible to leave my vehicle unattended. I merely go to township for personal needs. No time to spend health check up. But if it is arranged at factory sites like mobile ICTC then I can examine my blood.”
Peer educators mentioned that IEC materials were not properly displaced at facility centers. PLHA indicated long distance and long waiting time for getting testing result at ICTC. Some of the counselor misbehaved with them. There was no supply of safe drinking water and adequate space for counseling (lack of privacy). They experienced refusal of HIV test due to non-availability of test kits. Police harassed FSWs while they attended ICTC. Some of the counselor disowned them and fingered their practice. They wanted to perform VDRL and HIV test in same setting which was not offered from single window in many cases. One of the FSW shared experiences as follows:
“We along with our peer educator came out from the lodges to attend the ICTC clinic. The police personnel somehow could know our movement and trapped us and held us at police station. The police personnel harassed us and misbehaved with us and we got release instead of some amount of money. We failed to attend ICTC at that day. After that we move outside the lodge very carefully for STI check up and ICTC test. We preferred to attend the ICTC clinic at afternoon”.
Antenatal mother attended the PPTCT center for HIV testing. Counselor counseled them and prepared mother for delivery. But sometimes health care workers refused to provide services towards positive antenatal mother and referred them to higher center without proper indication.
The knowledge about PPTCT services was found very poor among migrant labours and truckers. Even they were unaware about such services available at district level. But the Peer educators were quite well aware about the PPTCT services and they faced some problem to access those services for pregnant women. The statement of one Peer Educator as follows:
“I accompanied one antenatal HIV patient for admission. She had labour pain. At emergency, attending doctor admitted the patient at labour ward. I rushed with the patient to labour ward. On duty nursing staff examined all relevant documents and found report of HIV. She informed doctor and convinced doctor to refer the patient to higher center, like Kolkata, as because she was HIV positive. Then I informed Dy. Chief Medical Officer –II who was the nodal officer of HIV/AIDS programme. After his interfere, patient was delivered at the same hospital.”
All PLHAs and peer educators indicated that some documents were required for registration at ART center. It was difficult to collect these documents such as residential certificate from panchyate prodhan or municipality chairman.
PLHAs experienced long waiting time and long distance at ART center. They had to visit twice for collection report of CD4 test. Supply of medicines was insufficient. They had to receive seven days medicine. ART center was more than 100- 150 kilometer away from different pockets of the district. So long distance they had to travel and spend large pocket money which was beyond their capacity. So they mentioned if at least bus and train fare was exempted during their visit to hospitals would be a great help for them. They had to stay at ART for a long time. But here was no arrangement for drinking water, toilet and proper sitting arrangement for clients. One statement of PLHA was bellow:
“I had to get up very early to hold the bus to go to Midnapore Medical College and hospital. It was 135 kilometer away from my residence. I reached at Midnapore Medical College and hospital at 11.00 AM. I met with the counselor and appeared for CD4 cell test. I asked for medicines, they refused to supply medicine as there was no doctor present on that day. Counselor advised me to come back after seven days. I missed to continue the drugs for three days. I got CD4 cell count at 3.30 PM and reached at home at 9.00 PM” on that day my expenditure was around Rs.240.00 and could not collect medicine. The same amount I had to spend for collecting medicine on next schedule date”.
The HIV positive status was not accepted in the community and in the family. HIV positive meant lifelong treatment like other chronic diseases such as diabetes, hypertension and heart diseases. But community people were not bothered about these diseases. Community people and even family member disregard HIV positive people. So, they were afraid of disclosure of positive status. With these consequences they missed to collect ART medicines, they feared to attend local hospital for disclosure of positive status. FSW and general client also reluctant to attend ICTC. Disclosure of HIV status would have been trouble to the children who would go to school. One of the FSW stated as her own experiences as:
“My husband is an alcoholic person. I have to look after my child. I used to practice this tread for last 8 years. I feared to test HIV at ICTC. Our PE always requested me to go to ICTC. One day I went there for test of my blood and found negative. After that I visited ICTC in regular interval and did HIV test. I apprehended that if I become positive. I will be evicted from my family. I will be treated characterless woman”.
Most of the working participants in the FGD confessed that positive status of her/him would not been accepted at her/him working place. Their colleague might have disowned her/him. Her/his job may be terminated due to HIV positive status. They heard that HIV is a chronic disease and will not be cured and had to treat whole life. So, the physical strength might have been reduced. PLHA and the peer educators stated that community people still had incorrect, incomplete & inadequate knowledge about HIV transmission. They still believed that HIV will be transmitted trough common social interaction and community activities and cultures. Due to this, PLHA were facing social distances, separation from the community, even eviction from the village. Education of their children also hampered. Participants among the FSW agreed that their clients would be reduced. One the PLHA stated his idea as follows:
“I was very sick, I was unable to move. Villagers could know somehow I and my husband were HIV positive. Nobody came to help me. Even villagers boycott us socially. With the help of NGO we (me & husband) started treatment at ART center at STM, Kolkata. Gradually we recovered from the illness and both of us physically fit. With the help of NGOs and district administration, some sensitization meeting was held at the village in presence of young people and PRI member. Now they did not refuse us. They communicated us socially and behave with us normally. Our child also study in the nearby school.”
Discussion and Recommendation
Summarizing the observations based on different FGDs we found out barriers at different levels related ICTC services, PPTCT services, ART services and personal and social barriers. Poor knowledge about HIV/AIDS was observed among the all participants accept peer educators. Knowledge about prevention of HIV/AIDS was worst among truckers and migrants labour. Some of the key barriers on HIV/AIDS services we observed such as (i) Distance of ICTC, PPTCT, ART center (ii) Improper sitting arrangements, inadequate space, unavailability of drinking water supply, toilets and over all unhygienic situation at facility centers (iii) Misbehaviour of staffs due to shortage of manpower, (iv) Inadequate supply of medicines and testing kits (v) Inter personal and social barriers. These findings were needed to be addressed by improving the care, support, testing and treatment services, and increased infrastructure development and human resource development.
The improvement of HIV testing services, availability of ART medicines, proper care and support to the PLHA increase the longevity and quality of lives of PLHA. These few points were the strategy to prevent HIV in the many developing world [9]. ICTCs were situated only at the a few health facilities. Only nine ICTCs were situated in the district with more or less 20 kilometer distance each. Knowledge about ICTC services were not been known by the migrants labours, truckers and FSWs. On the other hand long waiting times and long distance at ICTCs PPTCTs, ART center people were reluctant to receive services from there. Poor knowledge about HIV prevention and HIV transmission by the risk people, delayed to access services. Similar findings were found in the meta-analysis report [10]. As a result late diagnosis of HIV was done. Sometimes patient diagnosed as HIV positive at last stage and expired without much help with the ART medicines. Study in India also indicated long distance also hampered to access HIV services among the migrant labourer [11]. A study in Russia also indicated that inadequate knowledge among migrant labour about HIV, decreased access to HIV services [12]. To increase the knowledge of HIV/AIDS among the truckers and migrant labours there would be arrangement of sensitization meeting at their work place at regular interval. Folk media campaign and displace of posters will be helpful for them. NGOs were needed to be engaged to sensitize them in this regard. Mobile ICTC service would be arranged to minimize the time among the labourers to examine HIV at work place. Corporate authority could use some fund to the workers in this regard as corporate social responsibility (CSR).
But sensitization about HIV/AIDS among lodge based and street based FSW would be very difficult because they were not organized. They were flying and their clients were also flying. They were needed to be health check up on STI and RTI and HIV regularly. In this situation, sensitization among the hotel owners and their workers would be helpful to prevent HIV transmission. But it was easier to sensitize brothel based FSW and they were sensitized at regular interval. Here NGOs could play a crucial role. They might be organized health check up about STI, RTI and counseling services to FSW at their office and have to be arranged periodic HIV test at ICTC. But only one NGOs was engaged to perform such job for brothel based FSW. So, more NGOs would be helpful to overcome this barrier.
For HIV/AIDS control programme, screening of HIV virus is important. This service was being providing through ICTC & PPTCT center. All the participants indicated that these testing center were situated a far away from their residence. All the Block Primary Health Centers (BPHCs) were not covered with ICTC service. If all BPHCs were equipped with ICTC services then the accessibility of ICTC services will be increased. The prevention of HIV transmission among the migrant labourer could be done by regular HIV testing at their factory sites through mobile ICTC services and sensitization meeting with them. Sensitization could be achieved by magic show, folk song or any other medium about IEC.
NGOs workers indicated about police harassment with flying or lodge based FSW while they were come out from lodges to ICTC for HIV testing and counseling services. Such kind of police harassment was also seen in literature also [13]. So, counseling and HIV testing to FSW were needed to be arranged at Drop in Center (DIC). NGO workers and police department needed to be communicated each other while providing HIV services to the FSW.
Structural barriers such as less number of ICTC set up, less space at counseling center, less referral of pregnant women by the health care provider hampered the total ICTC services. This finding is similar with other study in Ethiopia [14]. Only district hospital has the designated PPTCT services for the pregnant women. This service was being providing integrated way through ICTCs. Health care providers sometimes refused to deliver service to HIV positive patient and refer them to other health facility without proper indication. This problem would be minimized by repeated sensitization to health care workers about HIV and AIDS. PLHA mentioned about short supply of ART medicines and non-availability HIV testing kits, reagent for CD4 and problem in laboratory machines forced them to repeated visit to ART center. PE and PLHA shared their experiences about pre-ART registration. Collection of some documents such as certificates from the panchyate or municipality, ration cards or voter card were troublesome on them. They had to rush before chairman of municipality or prodhan of panchyate several times. There was chance of disclosure of positive status. But it was require for registration. They lost their daily wages. Their pocket expenditure was increased. For this reason, there was chance of delay of initiation of treatment and a number of patients reluctant to collect medicines in time and started irregular treatment. So, strategy for ART center should be as simple as possible for the PLHA [15]. Study at African setting and at Maharashtra, India also observed that inadequate supply of medicines, long waiting time and long distance at ART center, frequent visit for collection medicines and medical reports caused increased expenditure to PLHA [16, 17]. There was no sufficient sitting arrangement, safe drinking water and toilet facility at ART center. These were the basic need for the clients. These arrangements needed to be improved for the patients. Due to increased patient load, there were needed to deploy more staff to serve the clients, especially at ART center. Social benefit scheme and travelling concession while attending at ICTC or ART center would helpful to PLHA. Social discrimination and stigmatization of HIV positive people is drawback of the HIV control programme. HIV/AIDS is one of chronic diseases like diabetes, hypertension which need lifelong treatment. All the respondents were afraid of disclosure of positive status and they felt trouble at home (eviction from the family), at community (social separation) and at working place (loss of job). Similar observation was mentioned a study at Karnataka, India [18]. In this situation a number of clients denied to collect medicines and lost to follow up. These social problems needed to be addressed with social counseling, extensive IEC campaign in the community and corporate sectors. HIV positive people’s forum took active part in this regards.
Proper trainings of health care providers are necessary to reduce the negative attitude towards HIV patients. Transmission of HIV among the truckers and migrants labours are to be reduced by sensitization workshop with them and supply of free condoms. Screening of HIV will be increased by engagement of mobile ICTC at factory sites. Regular sensitization campaign with FSWs and arrangement of regular health check up for STI/RTI and arrangement of free condoms are to be ensured to them. ART drugs and HIV testing kits are to be available uninterruptedly at ART center and ICTCs. Over and above ICTC services are to be provided at primary health center.
This study adds:
- Long waiting time and long distance of ICTC & ART center which hinder clients to access services.
- Insufficient ART medicines caused PLHA frequent visit at ART center.
- Structural barriers such as less number of ICTC and no ART center at district.
- Social & interpersonal barriers such as disclosure of HIV status and fear of discrimination in the community.
- This study suggested setting up ICTCs at each primary health center and ART center at least district hospital. Awareness generation programme is to be organized among the migrant labours, truckers and FSW on regular basis. Ensure regular and adequate supply of ART medicines. Arrange of social benefit scheme to PLHA.
Acknowledgement
The authors acknowledged NGO workers such as (SPARSHA,VES, TSK, Purba Medinipur), who supported us for data collection. The author also acknowledged Chief Medical Officer of Health Purba Medinipur for his guidance and co-operation.
References
- UNAIDS (2013) Global Report: UNAIDS report on the global AIDS epidemic 2013. “UNAIDS/ JC2502/1/E”, November 2013. www.unaids. org/sites/default/files/media_asset/UNAIDS_Global_Report_2013_en_1.pdf
- United Nations Programme on HIV/AIDS. USAIDS Gap Report, 2014. www.usaids.org/sites/default/files/en/media/unaids/contentassets/documents/unaidspublication/2014/UNAIDS_Gap_report_en.pdf
- The World Bank, HIV/AIDS in India, July 2012. www.worldbank. org/en/news/feature/2012/07/10/hiv-aids-india
- District Categorization for Priority Attention, National AIDS Control Organization (NACO), Prioritization of district for Programme implementation. naco.gov.in/upload/NACO%20PDF/District%20Categorisation%20for%20Priority%20Attention.pdf
- National AIDS Control Organization (NACO). National AIDS Control Programme (NACP-III), Preventive Strategy. www.naco.gov.in/ NACO/National_AIDS_Control_Program/Prevention_Strategies/
- Anti-Retroviral Therapy Guidelines for HIV Infected Adult and Adolescent, Department of AIDS Control, National AIDS Control Organization, Ministry of Health & Family Welfare, Government of India, May 2013.
- Census of India, 2011. www.census.gov.in
- Matovu JK, Makumbi FE (2007) Expanding access to voluntary HIV counselling and testing in sub-Saharan Africa: alternative approaches for improving uptake, 2001-2007. Trop Med Int Health. 12(11): 1315-22.
- Weine SM, Kashuba AB (2012) Labor migration and HIV risk: a systematic review of the literature. AIDS Behav. 16(6): 1605-1621.
- Pandey A, Benara SK, Roy N, Sahu D, Thomas M, Joshi DK, et al., (2008) Risk behaviour, sexually transmitted infections and HIV among longdistance truck drivers: a cross-sectional survey along national highways in India. AIDS. 22( 5): S81–90.
- Amirkhanian YA, Kuznetsova AV, Kelly JA, Difranceisco WJ, Musatov VB, Avsukevich NA, et al., (2011) Male labor migrants in Russia: HIV risk behavior levels, contextual factors, and prevention needs. J Immigr Minor Health. 13(5): 919–928.
- Weine S, Bahromov M, Mirzoev A (2008) Unprotected Tajik male migrant workers in Moscow at risk for HIV/AIDS. J Immigr Minor Health. 10(5): 461–468.
- Adedimeji A, Abboud N, Merdekios B, Shiferaw M (2012) A Qualitative Study of Barriers to Effectiveness of Interventions to Prevent Mother-to- Child Transmission of HIV in Arba Minch, Ethiopia. International Journal of Population Research.
- Beattie TS, Bhattacharjee P, Suresh M, Isac S, Ramesh BM, Moses S (2012) Personal, interpersonal and structural challenges to accessing HIV testing, treatment and care services among female sex workers, men who have sex with men and transgenders in Karnataka state, South India. J Epidemiol Community Health. 66(2): ii42-48.
- Hardon AP, Akurut D, Comoro C, Ekezie C, Irunde HF, Gerrits T, et al., (2007) Hunger, waiting time and transport costs: time to confront challenges to ART adherence in Africa. AIDS Care. 19(5): 658-665.
- Joglekar N, Paranjape R, Jain R, Rahane G, Potdar R, Reddy KS et al., (2011) Barriers to ART adherence & follow ups among patients attending ART centres in Maharashtra, India. Indian J Med Res. 134(6): 954-959.
- Boender TS, Sigaloff KC, Kayiwa J, Musiime V, Calis JC, Hamers RL et al., (2012) Barriers to Initiation of Pediatric HIV Treatment in Uganda: A Mixed-Method Study. AIDS Res Treat. 2012: 10.
- Beattie T, and Bhattacharjee P. Access to HIV testing and treatment services by high-risk groups in Karnataka, India: Barriers and Motivators. 2009. Karnataka Health Promotion Trust. www.khpt.org





