Factors Influencing the Utilization of Anti-Retroviral Drugs by HIV Positive Pregnant Women in Busia District, Busia County
Aquinatta ML1*, Gachuno O2, Wachira W3, Chawla K4, Thomasine D. Guberski5, Njiri F6, Wycliffe N7, Oyugi J8, Isaac o. Kibwage9
1 Senior Nursing officer, Department of Obstetrics and Gynaecology, University of Nairobi, Nairobi, Kenya.
2 Senior Lecturer, Department of Obstetrics and Gynaecology, University of Nairobi, Nairobi, Kenya.
3 Department of Social Studies, St. Pauls’ University, Nairobi, Kenya.
4 Senior Lecturer, Department of Obstetrics and Gynaecology, University of Maryland, USA.
5 Nursing, Department of Nursing, University of Maryland, USA.
6 Department of Obstetrics and Gynaecology, University of Nairobi, Kenya.
7 Research Grants Officer, University of Nairobi, Kenya.
8 Senior Lecture, Department of Microbiology, University of Nairobi, Kenya.
9 Professor, Department of Phamaceutical Chemistry, University of Nairobi, Nairobi, Kenya.
*Corresponding Author
Aquinatta .M. Lumili,
Kenya Registered Community Health Nurse-MSc CHD, MSc,
Implementation Science, Senior Nursing officer,
County Focal Person for PMTCT,
Department of Obstetrics and Gynaecology,
University of Nairobi, Nairobi Kenya P.O. Box 21031 Nairobi,
Kenya.
Tel: +254 726702196
E-mail: aquinattalumili@yahoo.com
Received: January 14, 2016; Accepted: March 03, 2016; Published: March 07, 2016
Citation: Aquinatta ML et al., (2016) Factors Influencing the Utilization of Anti-Retroviral Drugs by HIV Positive Pregnant Women in Busia District, Busia County. Int J AIDS Res. 3(1), 51-55.DOI : dx.doi.org/10.19070/2379-1586-1600012
Copyright: Aquinatta ML© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Antiretroviral drugs reduce viral replication in pregnant womeneither by lowering plasma viral load or through post-exposure prophylaxis in their new born. Mother to child transmission is the predominant mode of transmission of HIV in infants and young children.This transmission occurs during pregnancy, labour and delivery and breastfeeding. Providing all HIV positive pregnant women with lifelong ARVs regardless of CD4 count/disease stage is an effective strategy to avert MTCT of HIV. Eliminating vertical transmissions globally is still a challenge. In Busia district, the uptake of antiretroviral drugs by HIV positive pregnant women is about 41%. Despite the varied interventions employed to avert MTCTa number of exposed babies have been seroconverting.
Objective: Factors influencing utilization of ARVs by HIV positive pregnant women.
Methods: Cross sectional study was done through Purposive and random sampling. The study area and the HIV positive pregnant women were purposively selected. Quantitative approach was employed using standardized questionnaires. Exploratory data analysis was preceded by monovariate analysis. Results were summarized using tables and text. The quantitative data was analyzed by Statistics package of social science.
Results: Percentage (30.6%) of women started ARVs in the 3rd trimester. Percentage (37.4%) hides while taking the drugs due to self-stigma and fear of husband. Percentage 57.9% took freely. Half of those who were not on ARVs indicated they were afraid of their husbands while the other half were not willing to take the ARVs.
Conclusion: We found out 85% of the women had their first antenatal care visit in the second trimester while (30.6%) started ARVs in the 3rd trimester. ARVs taken for more than 17 weeks reduces the risk of MTCT. Disclosure of HIV status of pregnant women is essential. Male participation in antenatal care, treatment, counselling and testing for HIV, will increase use of interventions for eMTCT.
2.Broad Objective
3.Background
4.Research Design
5.Study population
6.Study area
7.Data Collection Instruments
7.Sample size
8.Sampling method
9.Ethical consideration and Consent
10.Data analysis
11.Study findings
11.1.Demographic data
11.2.Antenatal data
11.3.HIV status disclosure, treatment and adherence
12.Discussion
12.1.HIV status disclosure, treatment and adherence
13.Conclusion
14.Acknowledgment
15.References
Keywords
Mentor Mothers; Antiretroviral Drugs; Prevention of Mother to Child Transmission of HIV; HIV Positive Pregnant Women.
Broad Objective
To determine factors influencing the utilization of antiretroviral drugs by HIV positive pregnant women in Busia district.
Background
It has been reported by the WHO that globally HIV positive Pregnant women not receiving ARVs to prevent MTCT of HIV is 50% and women not on ARVs during breast feeding is about 80% and further reported that they are responsible for 65% of MTCT [1-4].
Globally, Sub-Sahara Africa continue to bear the burden of maternal to child transmission due to low utilization of ARVs and accounts for the highest number of new pediatric HIV infections [1] This transmission occurs during pregnancy, labour and delivery and breastfeeding. HIV/AIDS transmission from mother to child in Kenya is one of the biggest health and development challenges. Globally, an estimated 350,000 infants acquires the infection. [1, 2] In Kenya about 38,900 infants acquire HIV from mother annually. The most significant risk factor appears to be the HIV viral load in the women who are not on ARVs or have poor adherence and compliance [1, 3] There are now more facilities in Busia that offer HAART to HIV positive pregnant women to address previous bottlenecks of few facilities that had resulted into congestion. [4] A study carried out in Busia district, 96% HIV positive pregnant women were identified but antenatal uptake of ARVs is 41%. [3, 4]. HIV prevalence among pregnant women is 5.1% which almost mirrors the national figure of 7 %. In Busia county, 65% of HIV positive pregnant women do not deliver in the hospital despite the maternity services being availed at no cost .[4, 7] According to Busia District Health Information System (DHIS, 2012-2013) 3,500 children are in need of ARVs ,but only 1,431 are on treatment. [4] 280 children die monthly of AIDS related conditions and poor health seeking behavior.[4]. Most studies that have evaluated factors influencing PMTCT were conducted prior to 2007 when HAART was not being routinely used for prophylaxis to avert vertical transmission. We sought to determine if the same factors influence utilization of ARVs now that HAART has been availed for all HIV positive pregnant women.
Research Design
This was a cross sectional study that employed quantitative method.
Study population
The study population comprised of HIV positive pregnant women in Busia County.
Study area
The study was carried out in 3 County government hospitals and their surroundings (Busia District Hospital, Alupe Sub-District Hospital and Matayos Sub-County Hospital).
Data Collection Instruments
The tool that was used in this study was adapted from a study conducted in Zambia by Rosemary Mwanza (2009) that focused on factors influencing the uptake of ARVs for PMTCT.
Sample size
One hundred and eight (108) women were recruited. However, the number required for the study was seventy-five women according to sample size calculation using Fishers’ exact formula 1954 is illustrated below.
n= estimated sample
p=prevalence 5.1 %( prevalence of HIV infection among pregnant women in Busia)
∂= error margin set at 5%
z=standardized normal variable value corresponding to 95%.
Confidence interval is a normal distribution frequency which is 1.96.
Prevalence 5.1/100=0.051
n = (1.96)2 x 0.05 (1-0.05) / 0.05 x0.05
n = 3.8416 x 0.051 x (0.949) / 0.05 x 0.05 = 0.7530784 / 0.05 x 0.05
n = 0.7530784
n = 75
Sampling method
Cluster random sampling method was used to identify HIV positive pregnant women. Each cluster comprised of women that were linked to a mentor mother who provided a list of HIV positive pregnant mother. The participants were then picked randomly for interview at the time when they visited the facility at the antenatal clinic.
Ethical consideration and Consent
Ethical approval for this study was obtained from the Kenyatta National Hospital and University of Nairobi Ethical Review Committee. Additional clearance was obtained from Busia District and County Referral Hospital Research and Ethics committee.
Data analysis
AData was collected using a standardized data collection tools and entered into a password protected database. The validity of the questionnaire had been obtained during the pretesting. The data was analyzed through (SPSS) Statistics Package of Social Science.
Demographic data
We enrolled 108 HIV positive women who were pregnant. Fifty percent of these women were taking ARVs. Among all enrolled women, 63% had attained primary education, 25% secondary and 3.7% had no formal education. Seventy three percent had spouses as next of kin, 82.2% were married, 94.4% were self-employed, 86.9% were Christians and 10.3% were Muslims.
Antenatal data
Women without a previous pregnancy were 14.8%, one child 25%, and 2 children 18.5% and 3 children 20.4%. Majority of women (67.3%) had previously used family planning. The most common method used was injectable (44%) followed by orals (12%) and implants (12%) with only 5% IUDs. Majority of the women (85%) came for their antenatal clinics after the first trimester with 33% first attending during the 4th month (18wks), 25% during the 5th month, 22% during the sixth month (28wks) and 5% coming after 6months (28wks).
Over half (59%) of women came to the antenatal clinic to check the status of their pregnancy, 27% because they were unwell, 13% because they were advised by the health worker and only 3% because they were informed of free maternity services. During the ANC visit, all women were checked for blood pressure and weight, 97% had a physical exam, 90% had counseling, 52% got ARVs, 39% had a HIV test, 11% were tested for malaria and 9% were given antimalarial drugs. A small number of women 27% came for just a single ANC visit, with 37% coming for two visits, 11% coming for 3 visits and only 24% coming for 4 visits. During the antenatal visits, only 4% of the women reported waiting for less than 15 minutes, with 11%, 36%, 44% and 5% waiting for half an hour, one hour, over one hour and the whole day respectively. Majority of the women (82%) reported the services to be friendly, 1% said the service providers were rude or hostile and 16% said the service providers were kind but busy (Table 1).
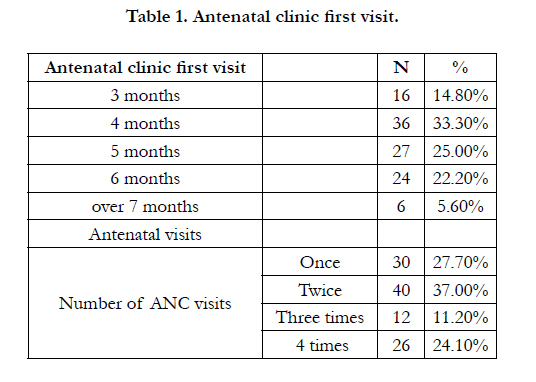

Table 1. Antenatal clinic first visit.
HIV status disclosure, treatment and adherence
Majority of HIV positive pregnant women were tested between the year 2012 and 2015 with only 5% being tested before the year 2005. At the time of testing 59% of the women were pregnant. After testing for HIV, a third 34% of the women were shocked, 22% cried, 18% were sad while the rest had other various emotional reactions. A half of the women 50% disclosed their HIV status to someone; 40% to spouse, 34% to a parent, 14% to a relative, 10% to a friend and 2% to a sibling. On disclosure, 64% of those disclosed to were supportive, 11% were in shock and 5% were unsupportive. Among the reasons for non-disclosure was; breakage of marriage 34%, secrecy 25%, fears of rejection 20% and stigma 20%. In terms of awareness of mother to child transmission of HIV, 95% of the women knew of transmission during breastfeeding, 91% during labor, 86% during pregnancy and 11% during weaning. Ninety eight percent of the women were aware that it was possible to prevent mother to child transmission using ARVs. 42% reported not being on ARVs at the time of the study with 68% reporting starting ARVs between the years 2012 and 2015. Only 5% reported starting ARVs before the year 2006. All women reported being counseled on use of ARVs. However, 37% reported fear and had to hide ARVs while taking them, 5% felt stigmatized and 58% took the ARVs freely. Percentage 64% of the women took ARVs at specific times and 35% at any time, with 35% reporting missing ARVs at least once and 24% missing ARVs more than two times. 14% reported missing ARVs for more than 5 times. Almost two thirds of the women 61% had a treatment partner who checked on them daily 48%, weekly 38%, two-weekly 2% and monthly 8%. All women reported knowing that ARVs benefits HIV positive pregnant women (Table 2).
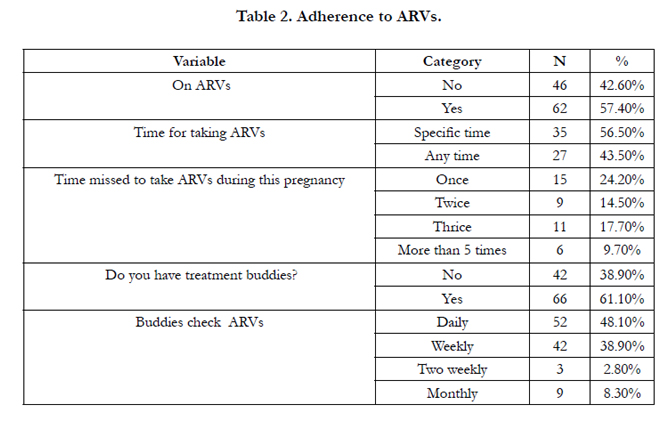
Table 2. Adherence to ARVs.
Discussion
Our study revealed that, 63% of the interviewed women had attained primary education, 25% secondary and 3.7% had no formal education. Level of education helps an individual to make important decisions in life. Women with primary level of education have a different understanding of the use of ARVs compared to those with secondary level of education. This is evidenced by a study in Tanzania which showed that men, who had attained secondary education, were more likely to be involved in the intervention of PMTCT compared to those who had primary or no formal education. Education has influence over the utilization of ARVs. We found out that majority of women (85%) make their first antenatal care visit in the second trimester. Previous studies revealed the importance of starting antenatal care early. When ARVs are taken for more than 17 weeks, it lowers viral load thus reducing the risk of MTCT. Early antenatal care attendance can optimize ARVs utilization for PMTCT.
A study done in Uganda [20, 21] on awareness among pregnant women about PMTCT improved the health of HIV positive pregnant women in both urban and rural areas. This attitude improved the uptake of the ARVs because the communities were sensitized on the importance of ARVs among HIV positive pregnant women.
HIV status disclosure, treatment and adherence
We found out that disclosure can influence the uptake of ARVs among pregnant women. A half of the women (50%) disclosed their HIV status to someone; 40% to spouse, 34% to a parent, 14% to a relative, 10% to a friend and 2% to a sibling. Disclosure has been found to be a source of distraction in the family in Sub- Saharan Africa. Among the reasons for non-disclosure were; fear of breaking marriage 34%, keeping as a secret 25%, fear of rejection 20% and stigma 20%. The study also revealed that 37% hide themselves time for taking ARVs, 5% felt self- pity when taking. If a woman has not disclosed her status to the spouse she cannot feel free to swallow her drugs in his presence.
Almost two thirds of the women 61% had a treatment buddy who checked on them daily, 48% weekly and38% two-weekly. This study has shown that 56% of the women took ARVs at specific times, with 24% reporting missing ARVs at least once.
Our study has shown that male partner involvement in PMTCT increases ARVs uptake, behaviour change, and compliance. Moreover, several studies from Uganda and Tanzania have shown that male participation in the antenatal care increases use of the interventions for PMTCT. Desire et al (2005) in his study confirmed that male involvement in PMTCT was a very powerful tool in the uptake of ARVs by pregnant women who test HIV positive. Comparing with the other studies done by Gourlay et al (2012) male involvement was minimal because of socio-cultural and economic factors that negatively influence them (Table 3).
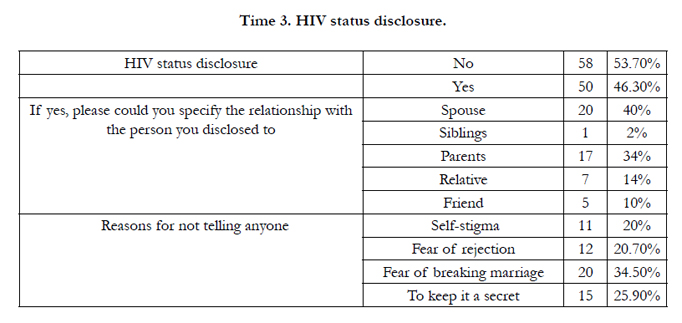
Time 3. HIV status disclosure.
Conclusion
We should advocate for early start of ANC because ARVs taken for more than 17weeks reduces the risk of MTCT. Adherence is important for good results. Disclosure of HIV positive results is crucial for the utilization of ARVs. There need for community sensitization on the utilization of ARVs by HIV positive pregnant women. To achieve the goal of eMTCT, male participation in antenatal care is very important.
Acknowledgment
Writing of this manuscript was supported by Medical Education Partnership Initiative (MEPI) and Partnership in Innovative Medical Education in Kenya (PRIME-K) under National Institute for Health (NIH), Grant NumberNIH-R24TW008889. My appreciationto God who gave me knowledge, strength and good health to go through this process. My gratitude to the principle of college of Health science for the chance to train as a fellow in Implementation science. My supervisors and co-others: Dr.Onesmus Gachuno,Dr. WachiraWamuyu , Dr. Kiranpreet Chawla, Dr. Thomasine D. Guberski, Dr. Oyugi Julius, Wycliffe Ndege for making it possible to prepare this manuscript, Francis Njiri for analyzing my data, All the Prime-K staff who were supportive during the process. And the entire community of the sisters of Mary of Kakamega for their love, care and continued support.
References
- UNAIDS (2012) Global report: UNAIDS report on the Global AIDS epidemic.
- National AIDS and STI Control Programmed (2011) National Guidelines for Antiretroviral Therapy in Kenya. (4th Edtn), Nairobi, Kenya.
- WHO (2010) PMTCT Strategic vision 2010-2015, preventing mother to child transmission of HIV to reach the UNGASS and Millennium Development Goal, in moving towards the elimination of pediatric HIV. Geneva.
- National AIDS and STI Control Programme (2009) Kenya AIDS Indicator Survey 2007: Final Report, Nairobi, Kenya.
- Kenya Demographic and Health Survey (2008-09). Calverton, Maryland: KNBS and ICF Macro.
- UNAIDS (2010) Global report: UNAIDS report on the global AIDS epidemic.
- World Health Organization (WHO) (2012) Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants: Programmatic Update. Geneva.
- National AIDS and STI Control Programme (2010) National Guidelines for HIV Testing and counseling in Kenya. (2nd Edition), Nairobi, Kenya.
- Gourlay A, Birdthistle I, Mburu G, Iorpenda K, Wringe A (2013) Barriers and facilitating factors to the uptake of antiretroviral drugs for prevention of mother to child transmission of HIV in sub-Saharan Africa: a systematic review. J Int AIDS Soc 16: 18588.
- Dabis F, Newell ML, Fransen L, Saba J, Lepage P, et al. (2000) Prevention of mother-to-child transmission of HIV in developing countries: recommendations for practice. The Ghent International Working Group on Mother-To- Child Transmission of HIV. Health Policy Plan 15(1): 34-42.
- Peltzer K, Mosala T, Dorkenoo E, Gumede T (2003) Health facility baseline report on Preventing Mother-To-Child Trans- mission (PMTCT) in a district of the Eastern Cape. Ford Foundation, Johannesburg.
- Henda N, Peltzer K (2005) Traditional birth attendants in the Eastern Cape, South Africa: characteristics, role and HIV/AIDS.
- Kominami M, Kawata K, Ali M, Meena H, Ushijima H (2007) Factors determining prenatal HIV testing for prevention of mother to child transmission in Dar Es Salaam, Tanzania. Pediatr Int 49(2): 286-292.
- Parahoo K (2007) Nursing Research: Principles, Process, Issues. MacMillan, London.
- Polit DF, Beck CT, Hungler BP (2001) Essentials of Nursing Research: Methods, Appraisal and Utilization. (5th edtn), Lippincott Williams & Wilkins, Philadelphia.
- Bajunirwe F, Massaguoi I, Asiimwe BS, Kamya M, Arts EJ, et al. (2004) Effectiveness of nevirapine and zidovudine in a pilot program for the prevention of Mother to child transmission of HIV-1 in Uganda. Afr Health Sci 4(3): 146-154.
- Bajunirwe F, Muzoora M (2005) Barriers to the implementation of programs for the prevention of mother-to-child transmission of HIV: A cross-sectional survey in rural and urban Uganda. AIDS Res Ther 2: 10.
- Rutenberg N, Baek C (2005) Field experiences integrating family planning into programs to prevent mother-to-child transmission of HIV. Stud Fam Plann 36(3): 235-245.
- Orne-Gliemann J, Tchendjou PT, Miric M, Gadgil M, Butsashvili M, et al (2010) Couple-oriented prenatal HIV counseling for HIV primary prevention: an acceptability study. BMC Publ Health 10: 197.
- Karamagi C, Tumwine J, Tylleskar T, Heggenhougen K (2006) Antenatal HIV testing in rural eastern Uganda in 2003: incomplete rollout of the prevention of mother-to-child transmission of HIV programme? BMC International Health and Human Rights 6: 6.
- Maman S, Mbwambo JK, Hogan NM, Weiss E, Kilonzo GP, et al. (2003) High rates and positive outcomes of HIV-serostatus disclosure to sexual partners: reasons for cautious optimism from a voluntary counseling and testing clinic in Dar es Salaam, Tanzania. AIDS Behav 7(4): 373-382.
- Moth IA, Ayayo AB, Kaseje DO (2005) Assessment of utilization of PMTCT services at Nyanza Provincial Hospital, Kenya. Sahara J 2(2): 244-250.
- Omondi MX, Ongo’re D, Ngugi E, Nduati RW (2012) The quality of PMTCT services and uptake of ARV prophylaxis amongst HIV positive pregnant women in Kakamega district, Kenya. Afr J Pharmacol Ther 1(2): 55-61.
- Futterman D, Shea J, Besser M, Klosinski L, Stafford S, Rotheram-Borus MJ (2009) Mamekhaya: Enhancing South African PMTCT programs with culturally-adapted evidenced-based intervention AIDS 2006 _ XVI International AIC conference.
- Mothers2Mothers (2006) Annual report.





