Profile of Seropositives Visiting a HIV Screening Centre of a Tertiary Care Teaching Institute in North India
Siddharth Rao PS1*, Bajpai S2, Pandey P3, TN Dhole4, Hem Chandra5
1 Senior Resident, Department of Hospital Administration, SGPGIMS, Lucknow, India.
2 Laboratory Technologist, Department of Microbiology, SGPGIMS, Lucknow, India.
3 Counsellor, Department of Microbiology, SGPGIMS, Lucknow, India.
4 Professor and Head, Department of Microbiology, SGPGIMS, Lucknow, India.
5 Professor and Head, Department of Hospital Administration, SGPGIMS, Lucknow, India.
*Corresponding Author
Siddharth Rao PS,
Senior Resident,
Department of Hospital Administration,
SGPGIMS, Lucknow-226014, India.
E-mail: drsidrao@gmail.com
Received: December 16, 2015; Accepted: January 28, 2016; Published: February 02, 2016
Citation: Siddharth Rao PS et al., (2016) Profile of Seropositives Visiting a HIV Screening Centre of a Tertiary Care Teaching Institute in North India. Int J AIDS Res. 3(1), 46-50.DOI : dx.doi.org/10.19070/2379-1586-1600011
Copyright: Siddharth Rao PS© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: In the era of declining HIV/AIDS prevalence, low penetration of Information Education and Counseling (IEC) activities, particularly among the rural community is still a matter of concern for public health officials. Integrated Counseling and Testing Centers (ICTC’s) are key entry points for a wide range of interventions in HIV awareness, prevention and care in India.
Objective: The objective of current study was to assess the socio-demographic profile and risk behavior of attendees who tested seropositive at our ICTC clinic.
Methodology: A prospective questionnaire based study from August 2009 to December 2013 was conducted in the ICTC attached to Microbiology department of SGPGIMS to enumerate the socio-demographic and risk behavior pattern of HIV positive cases.
Result: Among 16038 attendees investigated during the study, 298(1.86%) tested positive for HIV with a male to female ratio of 2.24:1. Maximum seropositivity (35.6%) was found in the age group of 31-40 years followed by 21-30 years age group (26.8%). Most of the study individuals were married (86.6%) and belonged to rural community. Unprotected heterosexual route was found to be the commonest (71.1%) mode of infection. The majority of the subjects had received education up to primary (36.2%) and secondary level (31.9%).
Conclusion: The rural population and the sexually active and economically productive age group dominated among the HIV seropositives presenting at this centre. Heterosexual route is still the predominant mode of transmission among seropositives. Recommendation: The planning and designing of IEC activities should be based on socio-demographic profile and risk behavior pattern of a particular area.
2.Introduction
3.Methodology
4.Results
5.Discussion
6.Conclusion & Recommendation
7.Limitations of Study
8.References
Keywords
HIV; AIDS; Seropositive Profile; ICTC.
Introduction
HIV/AIDS continues to behave as a pandemic and is still a major issue as far as morbidity and mortality are concerned. The burden has already started to decline. According to UNAIDS/ WHO estimates, there are 35.3 million people living with HIV worldwide [1]. National AIDS Control Organization (NACO), supported by UNAIDS and WHO, indicate that the national adult HIV prevalence in India is approximately 0.27%. This corresponds to an estimated 20.9 lakhs of people living with HIV in the country [2].
Since the detection of the first case in 1986 from Chennai, HIV/AIDS is spreading very fast in India. The spread is a consequence of a specific behavioral pattern and the distribution is quite uneven in India. Hence to strengthen interventional strategy, an assessment of socio-demographic factors, level of awareness as well as risk behavior of the population is mandatory. The Integrated Counseling and Testing Centre (ICTC) is an entry point to free HIV testing in India. It provides the general public with an opportunity to learn and accept their HIV serostatus in a confidential environment [3].
In view of non-availability of a licensed vaccine, and relatively expensive drugs, ICTC has become a cost effective intervention in preventing HIV transmission through early detection and behavioral counseling. The therapeutic angle is dealt with by giving free retroviral drugs at ART centers located in medical colleges of the country. These two approaches have become the cornerstone of the fight against HIV/AIDS in India.
The objective of this study was to assess the socio-demographic profile as well as risk behavior of attendees who tested seropositive at our ICTC clinic.
Methodology
The study was conducted in the ICTC clinic attached to microbiology department of Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGIMS), a premier tertiary care medical research institute of North India. On an average, 15-20 individuals per day present for HIV related investigations in this centre. Only seropositive attendees from August 2009 to December 2013 were included in this study. An informed, verbal and written consent was taken from participants. Patient’s confidentiality was ensured throughout the course of the study. In order to elicit information regarding socio-demographic profile and risk behavior, a structured, pretested proforma was used. It was composed of only close-ended questions of dichotomous as well as multiple choice types. In addition, seropositive females were interviewed to assess their knowledge regarding the modes of transmission of HIV.
Results
ICTC is a unit centre of National Aids Control Organisation (NACO) established by the Government of India at SGPGIMS for HIV testing and counseling services free of charge to the general public. A total of 16038 attendees were registered during the period of study at ICTC. The study included only the data of the 298 seropositives. The overall HIV positivity was 1.86% (298/16038). Male to female ratio among seropositives was 2.14:1 (Table 1) (Figure 1).
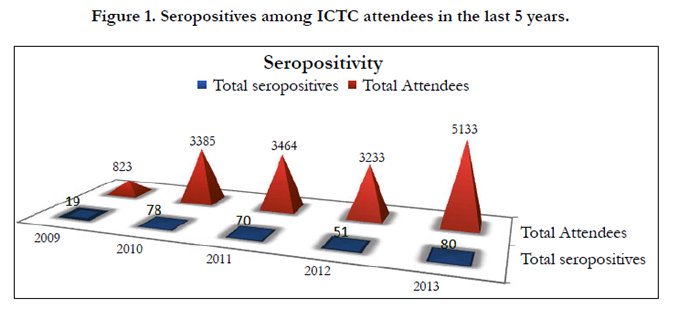
Figure 1. Seropositives among ICTC attendees in the last 5 years.
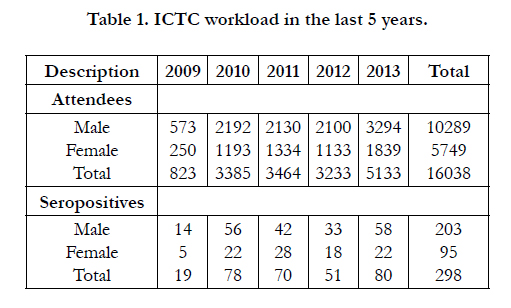

Table 1. ICTC workload in the last 5 years.
The most common affected age group was 31-40 years (35.6%). The median age among the seropositives was found to be 35 years.
Overall 87.6% of the study individuals were literate. Illiteracy was more pronounced in female seropositives than males (22.1% in females vs. 7.9% in males). More than two third (70.5%) of the seropositives were from rural areas.
In relation to marital status 87.7% positive males and 84.2% of positive females were married. The married to unmarried ratio was 7.8:1. Majority of the study individuals were Hindus (92.9 %) and Muslims constituted 6.7 % of the seropositives.
Regarding occupation, service and business class comprised of 9.1% and 20.5% respectively.
Most of the seropositives belonged to rural set up (70.5%). This type of distribution is most likely representative of the catchment area of the institute.
Heterosexual contact was found to be the most common mode of transmission; 71.9% (males) and 69.5% (females). None of the female clients in this study were commercial sex workers.
Self initiated clients accounted for 5.9% (7.28% males versus 3.48% females). From among the 298 seropositives, 80.9% underwent healthcare provider initiated HIV testing (i.e prescribed by a doctor) and 19.1% walked in directly. The demographic, socioeconomic, and risk behavior profiles of HIV positive clients are depicted in Table 2.
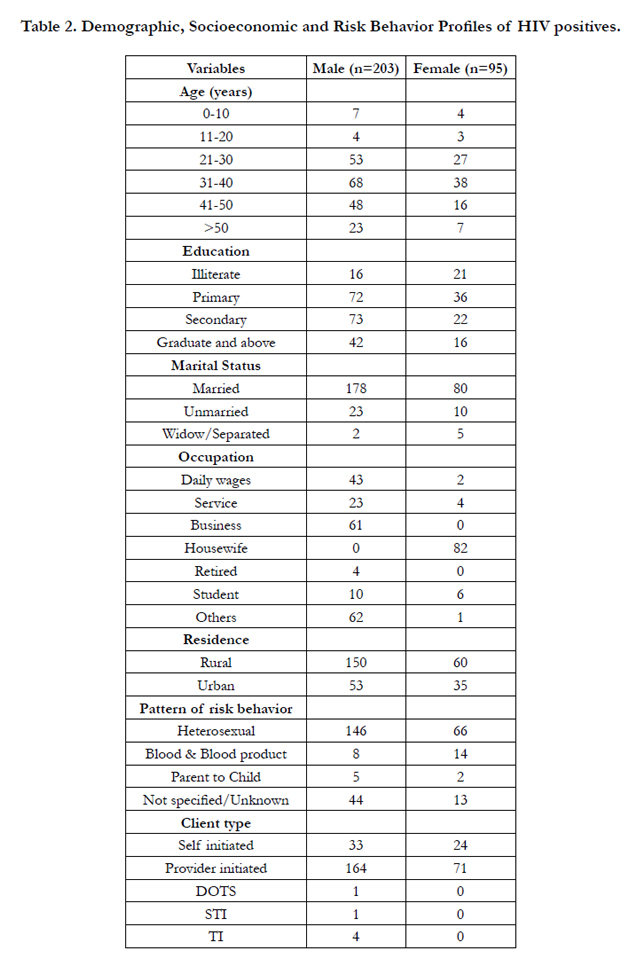
Table 2. Demographic, Socioeconomic and Risk Behavior Profiles of HIV positives.
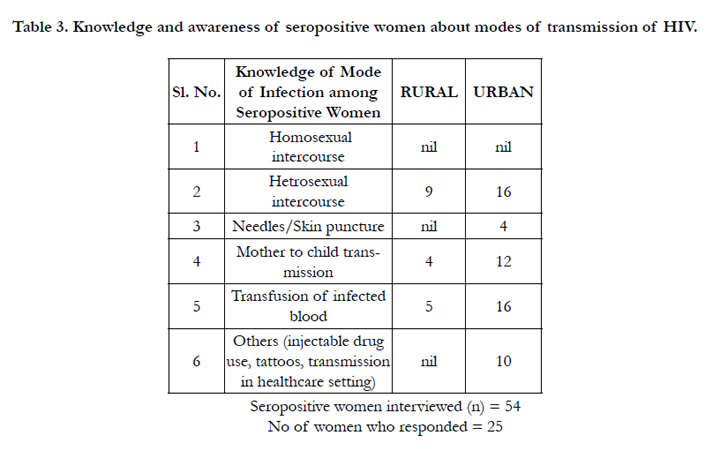
Table 3. Knowledge and awareness of seropositive women about modes of transmission of HIV.
Of the seropositive women (n=54) who were requested to answer questions regarding the modes of transmission of HIV, only 25 of them agreed to participate.
Amongst the respondents, none of them had any idea of the homosexual route of transmission of HIV (even among those who came from an urban background). As the catchment area of this institute lies within an ultra conservative region of the country where homosexuality is taboo, this outcome was not surprising to the researchers.
Transmission from mother to child as a mode was known to more urban women than those from a rural background.
Women from a rural background also did not have knowledge of injectable drug use, tattoos and risk of acquiring HIV infection in a healthcare setting as a mode of infection.
Discussion
ICTCs are located in the microbiology department of all government medical colleges in India. They provide HIV counseling and testing services free of charge to the general public. This study was intended to give an overview of profile of seropositive clients who visited our ICTC. The trend showed a steady increase in the number of attendees and seropositives over years except for a small decline in 2012.
The prevalence of HIV seropositivity among ICTC clients in the present study was noted to be 1.86%, which was similar (1.006%) to a study conducted in Meerut during 2013 [4]. In contrast, the prevalence was lower than that reported from a study conducted in Wardha district of Maharashtra in 2008 (12.5%) [5].
Higher seropositivity in the present study compared to that from Meerut [4] was due to increased number of attendees from rural population. Differences in health seeking behavior of community could also have contributed to the difference in HIV prevalence in different studies.
Seropositive females were 31.9% of the total HIV positives, which was slightly lower than the national average for females (39%). The difference in attendance rate at ICTC suggested the existence of a gender barrier preventing access for females to avail health services. Stigma and discrimination as a barrier to seeking treatment could not be ruled out.
Majority of seropositives (72.9% males and 80% females) belonged to the sexually active age group (15-45 yrs). Other studies conducted at Udupi and at Gwalior reported the percentage of reproductive age group among attendees to be 88.7% and 83.2% respectively [6, 7]. These findings emphasize that specific interventions should be targeted towards this vulnerable group.
A total of 94.07% (15088/16038) clients were being referred by doctors and among them HIV seropositives constituted 1.6%. However, among the self initiated clients, the seropositivity was 6%. The referred clients’ ratio was high because of the health seeking behavior of a particular region which in turn is influenced by IEC activities in that area.
The majority of the seropositives had received education till secondary level (68.1%). The rest was composed of 12.5% illiterate and 19.4% were graduates and above.
Many who tested seropositive belonged to rural background (70.5%). This type of distribution could be explained by the fact that a number of patients seeking treatment in this institute are referred from rural areas.
Our study demonstrated 86.6% of seropositives to be married and which corresponds to a study by Rawat et al from Meerut (80%) [4]. However, other studies showed marital status to be unrelated to HIV seropositivity [8].
With respect to occupation, high seropositivity was seen in subjects employed in government service and among businessmen (9.1% and 20.5% respectively). Association of seropositivity among females was higher among housewives. Students constituted 5.4% among the seropositives. The long distance truck drivers and daily wage workers who are a highly mobile group composed 18.4% and 17.1% respectively.
In our study 71.1% of transmission was through heterosexual route. Blood and blood product transfusion and mother to child transmission shared 7.4% and 2.4% respectively. The study from Meerut demonstrated heterosexual route to be associated with 85% of incidences of transmission [4]. Transmission linked to blood and blood products accounted for only 1%.
Poor knowledge among rural women regarding transmission of HIV virus especially modes like homosexuality, injectable drug use, tattoos in addition to risk of acquiring HIV infection in a healthcare setting. This was reflected in the poor response to questions. This indicates the poor penetration of Information, Education and Counselling (IEC) activities despite increased government focus and spending.
Conclusion & Recommendation
Awareness of HIV-AIDS among the population is still low leading to more seropositive patients among rural population compared to that from urban areas. Activities should be vigorously planned to increase attendance at ICTC, particularly with reference to self initiated clients. The planning and designing of IEC (Information, Education and Communication) activities should be based on socio-demographic profile and risk behavior pattern of a particular area.
Limitations of Study
As this study was hospital based, the results obtained from the study were influenced by the catchment area of hospital, care seeking behaviour of population and social stigma associated with the disease. Hence generalizing the results to the population would be inappropriate. A better alternative could be a community based study.
References
- UNAIDS Report on the Global AIDS Epidemic 2013.?
- NACO Annual Report: Department of AIDS Control Ministry of Health and Family Welfare. New Delhi.
- Campbell CJ, Marum ME, Alwano-Edyegu M, et al. (1997) The role of HIV counseling and testing in the developing world. AIDS Educ Prev 9(suppl): 92-104.
- Rawat A, Pandey A, Madan M, Singh V, Shivendra, et al. (2013) Profile of HIV positive attendees of an integrated counseling and testing centre in Meerut – A Changing Trend. Indian J Public Health Res Development 4(2):44-47.
- Quazi S, Nimbarate S, Selokar D, Gaidhane A, Mudey A, et al. (2010) Profile of clients attending an integrated counseling and testing centre at a private rural tertiary care hospital in India. Australasian Med J 3(6): 349-352.
- Gupta M (2009) Profile of clients tested HIV positive in a voluntary counseling and testing centre of a district hospital, Udupi. Indian J Community Med 34(3): 223-226.
- Mishra S, Mishra A (2013) Sociodemographic profile of an integrated counseling and testing centre attendees: A cross sectional study at a tertiary care hospital in Gwalior, India. Nat J Community Med 4(3): 493-497.
- Giri TK, Wali JP, Meena HS, Pande I, Uppal S, et al. (1995) Sociodemographic characteristic of HIV infection in Northern India. J Commun Dis 27(1): 1-9.





