Cryptococcal lymphadenopathy: A Rare Case Report
Uttiya Brahmachari*, Guchhait B
Post Graduate Trainee, Department of Tropical Medicine, Calcutta School of Tropical Medicine Kolkata, West Bengal, India.
*Corresponding Author
Uttiya Brahmachari,
Post Graduate Trainee,
Department of Tropical Medicine,
Calcutta School of Tropical Medicine Kolkata,
West Bengal, India.
Tel: +91-9903707630
E-mail: uttiya@live.in
Received: March 25, 2015; Accepted: April 20, 2015; Published: April 22, 2015
Citation: Uttiya Brahmachari, Guchhait B (2015) Cryptococcal lymphadenopathy: A Rare Case Report. Int J AIDS Res. 02(3), 32-33. doi: dx.doi.org/10.19070/2379-1586-150006
Copyright: Uttiya Brahmachari© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Disseminated cryptococcosis is a life threatening opportunistic infection amongst the HIV infected population. Infections of central nervous system, lungs and skin by Cryptococcus neoformans are very common. Although it can infect any organ, cryptococcal lymphadenopathy is a rare manifestation. Here we report a rare case of Cryptococcal meningitis with cryptococcal lymphadenopathy in a HIV infected middle aged female.
2.Abbreviations
3.Introduction
4.Case Report
5.Discussion
6.Conclusion
7.References
Keywords
Cryptococcal Lymphadenopathy; Cryptococcal Meningitis; Disseminated Cryptococcosis; Opportunistic infections.
Abbreviations
CSF: Cerebrospinal Fluid; ADA: Adenosine Deaminase; PAS: Periodic Acid-Schiff; MRI: Magnetic Resonance Imaging; UBO: Unidentified Bright Objects; AmB: Amphotericin B; CNS: Central Nervous System; FNAC: Fine Needle Aspiration Cytology; PLHIV: People Living with HIV.
Introduction
Cryptococcal infection or cryptococcosis is caused by infection of Cryptococcus neoformans, a dimorphic fungus. It can infect subjects ranging from the apparently immunocompetent to severely immunocompromised patients, like persons suffering from HIV infection, malignancy or recipients of organ transplantation. From asymptomatic colonization in respiratory tracts to severe fatal disseminated disease, cryptococcosis covers a wide spectrum of manifestation. Particularly important are the opportunistic infections seen in the HIV infected population. Cryptococcal meningitis is a very common, albeit fatal infection seen in these patients. Besides meningitis, infection of skin, respiratory tract, bone marrow, eyes are common. Lymphadenopathy due to cryptococcal infection is a rare manifestation.
Case Report
A 38 year old female patient attended the outpatient department with complaints of fever for 14 days and swelling over the right side of neck for 14 days. Her fever was low grade and continuous, without any chills or rigors. The swelling on the neck started insidiously, was gradually progressive and was painless. On further interviewing, she also complained of mild headache which occurred occasionally.
On examination, she was found to have 3 discreet cervical lymph nodes on the right side, which were mobile, firm, non-tender and free from skin and underlying structures. No other lymph nodes were palpable anywhere. She had subtle neck stiffness. However Kernig’s sign and Brudzinski’s sign were negative. Other systemic examinations were essentially normal.
Laboratory investigations showed Hemoglobin 7.7 g%, a total leukocyte count of 6,600/cumm, with 89% neutrophils, 8% lymphocytes, 2% eosinophils and 1% monocytes. Her liver function test, serum urea, creatinine, electrolytes were normal. CSF study from lumbar puncture showed 10 cells, of which 60% were lymphocytes and the rest neutrophils. CSF glucose was 48 mg/100 ml and protein was 36 mg/ 100 ml, with ADA being 2.0 U/L. India Ink stain of the CSF showed buddying yeast cells resembling Cryptococcus neoformans. A serum cryptococcal antigen assay was done before the CSF reports were available. It was reactive with a titre of 1:1024. Fine needle aspiration from cervical lymph node stained with PAS also showed buddying yeast cells with surrounding halos, suggestive of Cryptococcal species. A MRI of brain was done which showed generalized cerebellar atrophic changes with small areas of hyperintensities in subcortical parieto-frontal region likely nonspecific signals/ UBOs. She was also diagnosed as HIV infected with CD4 count of 50 cells/cu mm.
A diagnosis of cryptococcal meningitis with cryptococcal lymphadenopathy was made and amphotericin B along with fluconazole was started before the report for CSF culture was available. On the 4th day of admission, culture report confirmed the growth of Cryptococcus neoformans. Treatment with AmB and fluconazole was continued. During this course of therapy patient complained of increasing headache and she was managed with therapeutic drainage of CSF by lumbar puncture on 3 occasions. On the 15th day of AmB, another lumbar puncture was done and the CSF was sent for fungal culture which again showed growth of Cryptococcus.
AmB with high dose fluconazole was reinitiated for another 2weeks. However she developed hepatitis along with renal failure after 7th day of therapy. She also faced electrolyte abnormalities, with serum sodium being 160 mEq/L and serum potassium being 3.2 mEq/L. Despite aggressive management, she succumbed to death from multiorgan dysfunction syndrome after 2 days.
Discussion
Cryptococcal infection or cryptococcosis is an opportunistic infection
caused by Cryptococcus species (C. neoformans being most common.) which is present in soil contaminated with pigeon excreta [1]. It is distributed all over the world. The organisms easily get into the respiratory tract of human beings through inhalation of dust contaminated by spores of Cryptococcus, but dissemination occurs thereafter to CNS, skin, bone, lymph node, kidney and other viscerae [2]. Cryptococcal meningitis and disseminated cryptococcosis have gained importance recently because of rise in incidence of HIV infection worldwide. Cryptococcal lymphadenitis is an uncommon form of cryptococcosis which is an AIDS defining condition according to the centre for disease control and prevention guideline [2].
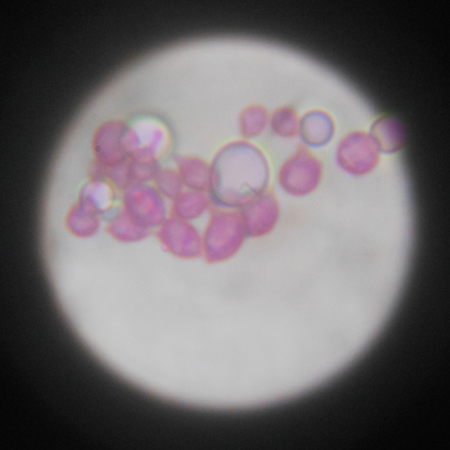
Figure
Cryptococcus has been reported from cytological specimens of CSF, sputum, bronchial lavage and FNAC smears of the lymph nodes, thyroid, spleen, adrenal gland, bones and the lung [3]. The organism is capsulated with a meucopolysacharide and measures 5-15μm in diameter. Special stains (Gomori’s Methanamine Silver, PAS and Mucicarmine) facilitate the identification of this organism. Granulomatous inflammation, which may be slight or absent, can be caused by cryptococci [4]. Although, in the developing countries, tuberculosis remains the most common cause of meningitis in PLHIV [1], cryptococcal meningitis happens to be the most common, life threatening, opportunistic CNS infection in HIV infected individuals in developed countries.
The clinical presentation in this case with cervical lymphadenopathy and neck stiffness made tuberculosis the first differential diagnosis, especially with its high prevalence in India. CSF examination revealed pleocytosis with lymphocytic predominance along with increased protein and decreased glucose. Budding yeasts like organisms were also observed in the CSF. India ink preparation revealed capsulation of yeast cells. Fine needle aspiration cytology of cervical lymph node revealed amorphous granular background with scattered epithelioid cell and many encapsulated forms of cryptococci along with lymphocyte and histiocytes. PAS stained smear was positive for budding yeasts.
Cryptococcosis carries a poor prognosis even with antifungal therapy. In patients with compromised immunity, the prognosis is worse. Cryptococcal meningitis tends to have a lower chance of survival if CSF pressure is high, with positive smear for yeast cells (evidence of high fungal burden), low CSF glucose level, and high CSF cryptococcal antigen titre (≥1:1024) [5]. Cryptococcus recovered from extraneural sites increases chance of mortality in a case of diagnosed cryptococcal meningitis. Our patient carried multiple poor prognostic factors and her chance of survival was slim from the very outset. Most of the guidelines on treatment of opportunistic infections prophesy the use of liposomal amphotericin B along with flucytosine as the ideal treatment regimen for cryptococcal meningitis. However due to resource poor setting and unavailability of flucytosine in India, we had to treat our patient with amphotericin B deoxycholate along with fluconazole.
Conclusion
Cryptococcal disease is commonly encountered among the immunocompromised patients. Although the most common form of the disease is meningitis, dissemination to extraneural sites can be seen and they usually carry grave prognosis. Even with optimum treatment rate of mortality remains high. In resource poor setting, treatment options remain very limited which further add to the failures in treating these patients.
References
- Das BP, Panda PL, Mallik RN, Das B (2002) Cryptococcal lymphadenitis and meningitis in human immunodeficiency virus infection: A case report. IndianJournal of Pathology Microbiology 45(3): 349-351.
- Suchita S, Sheeladevi CS, Sunila R, Manjunath GV (2008) Fine needle aspiration diagnosis of cryptococcal lymphadenitis; A window of opportunities. Journal of Cytology 25(4): 147-149.
- Wright CA, Leiman G, Bevatar B (2000) Fine needle aspiration of cryptococcal lymphadenitis: further observations using Autofluorescence. Actacytologica 44(2): 281-282.
- Lee MY, Chung JH, Shin JH, Hwang TJ, Kim KS, et al. (2001) Lymphonodular cryptococcosis diagnosed by fine needle aspiration cytolgy in hyper-IgM syndrome: A case report. ActaCytologica 45(2): 241-244.
- Lu CH, Chang WN, Chang HW, Chuang YC (1999) The prognostic factors of cryptococcal meningitis in HIV-negative patients. JHosp Infect 42(4):313-20.





