Restless Legs Syndrome
Najmi S1, Pourabolghasem S2*
1 Assistant Professor of Neurology, Movement Disorders Neurologist, Tabriz University of Medical Science, Iran.
2 Assistant Professor, Tabriz University of Medical Science, Iran.
*Corresponding Author
Shabnam Pourabolghasem,
Assistant Professor,
Tabriz University of Medical Science, Iran.
Tel: +98 9143152339
Fax: +98 4113370976
E-mail: sh.pourabolghasem@gmail.com
Article Type : Review Article
Received: July 16, 2015; Accepted: August 17, 2015; Published: August 19, 2015
Citation: Najmi S, Pourabolghasem S (2015) Restless Legs Syndrome. Int J Chronic Dis Ther 1(1) 1-4.
Copyright: Pourabolghasem S© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
1.1.Definition
1.2.Signs and Symptoms
1.3.Etiology
1.4.Epidemiology
1.5.Pathophysiology
2.Diagnosis
3.Management
3.1.Pharmacologic therapy
3.2.Non-pharmacologic treatment consists of [34]
4.Prognosis
5.Essential Update
7.References
Keywords
Asystole, Laryngoscopy, Neurosurgery.
Introduction
Restless legs syndrome (RLS) is a type of movement disorders that is often associated with a sleep complaint and generally involving the limbs. Persons who suffer from RLS may report unpleasant ill-defined sensations, such as strong not painful urge to move the legs, crawling, creeping, pulling, itching, drawing, or stretching, forceful bothering inner pressure in legs, uncomfortable treading of legs when they lie down for sleep. These intolerable sensations are relieved by movement of the legs or by walking. The feeling usually is bilateral and the arms are rarely involved. Recently, Lang et al. reported Restless Genitalia syndrome (Lang et al. JAMA neural Oct 6 2014).
RLS may lead to significant physical and emotional disability.
Unfortunately, RLS usually is missed during primary exams [3, 7]. Lots of patients are not diagnosed until many years after onset of signs and symptom. RLS commonly starts at middle age or older, although it may begins at any age, even as early as infancy.
- An urge to move the legs usually accompanied by or in response to uncomfortable and unpleasant sensations in the legs, characterized by all of the following:
- The urge to move the legs begins or worsens during periods of restoring activity.
- The urge to move the legs is partially or totally relieved by movement.
- The urge to move the legs is worse in the evening or at night than during the day, or occurs only in the evening or at night.
- The symptoms in Criterion A occur at least three times per week and have persisted for at least 3 months.
- The symptoms in Criterion A are accompanied by significant distress or impairment in social, occupational, educational, academic, behavioral, or other important areas of functioning.
- The symptoms in Criterion A are not attributable to another mental disorder or medical condition (e.g., arthritis, leg edema, peripheral ischemia, leg cramps) and are not better explained by a behavioral condition (e.g., positional discomfort, habitual foot tapping).
- The symptoms are not attributable to the physiological effects of a drug of abuse or medication (e.g., akathisia).
The symptoms of RLS usually are worsen during inactivity and often interfere with sleep, leading to chronic sleep deprivation and stress [8].
Approximately 85% of RLS patients suffer from abnormal periodic limb movements during sleep, that usually involving the legs (periodic leg movements of sleep [PLMS]) [2]. PLMS is characterized by involuntary, forceful dorsiflexion of the foot lasting almost 0.5-5 seconds and occurring every 20-40 seconds throughout sleep.
Other features commonly associated with RLS but not required for diagnosis include the following:
- Sleep disturbances.
- Daytime fatigue.
- Involuntary, repetitive, periodic, jerking limb movements:Either during sleep or while awake and at rest.
The International RLS Study Group (IRLSSG) updated its diagnostic criteria in 2012. The current IRLSSG criteria are nearly identical to the DSM-5 criteria listed above.
RLS may be either primary or secondary. In most instances, RLS is a primary, idiopathic central nervous system (CNS) disorder. Such idiopathic disease can be familial in 25-75% of cases. In these familial cases, RLS appears to follow a pattern of autosomal dominant or recessive inheritance. Various chromosomes have been implicated so far, like 12q, 14q, 9p, 20p, 4q, and 17p.
Patients with familial RLS tend to have an earlier age of onset (< 45 years) and slower disease progression. In some families, a progressive decrease in age of onset with successive generations (i.e. genetic anticipation) has been described. Psychiatric factors, stress, and fatigue can exacerbate symptoms of RLS.
Secondary RLS can develop as a result of certain conditions or factors. The most important and common causes of secondary RLS are iron deficiency and peripheral neuropathy [6, 7]. due to the prevalence of these conditions in the general population, their association with RLS must be keep in mind.
Pregnancy is another important causative factor for RLS, which is estimated to affect 25-40% of pregnant women. The syndrome usually subsides within a few weeks after delivery. A long-term follow-up study reviled that women who develop RLS during pregnancy have a 4 time increased risk of developing chronic primary RLS compared with women without similar history [16].
RLS also occurs in as many as 25-50% of patients who have endstage renal disease; these patients find their symptoms to be particularly bothersome during hemodialysis.
Takaki et.al found that hyperphosphatemia, anxiety, and a high degree of emotion-oriented coping with stress were independently related to the presence of RLS in patients with uremia who were undergoing hemodialysis [9]. RLS may improve after kidney transplantation.
Medication’s side effect is another cause for secondary RLS. The following medications have been known to cause or exacerbate the symptoms of RLS:
- Anti-dopaminergic medications (eg, neuroleptics)
- Diphenhydramine
- Tricyclic antidepressants (TCAs)
- Selective serotonin reuptake inhibitors (SSRIs)
- Serotonin-norepinepherine reuptake inhibitors (SNRIs)
- Alcohol
- Caffeine
- Lithium
- Beta-blockers
Some other uncommon causes of RLS include the following:
- Folate or Magnesium deficiency
- Amyloidosis
- Diabetes Mellitus
- Lumbosacral Radiculopathy
- Lyme disease
- Monoclonal gammopathy of undetermined significance
- Rheumatoid arthritis
- Sjögren syndrome
- Uremia
Estimated prevalence of RLS affects in the United States is almost 5-15%. Although the exact international prevalence of the disease is uncertain, limited studies have indicated that 2-15% of the world’s population may experience symptoms of RLS [6].
Although the prevalence of RLS is increased with age, it has a variable range of onset age, even can occur in children. 33-40% of Patients with severe RLS had their first symptom before the age of 20 years, although the precise diagnosis of RLS was made much later [17]. RLS usually progresses slowly to daily symptoms and severe disruption of sleep after age 50. Individuals with familial RLS tend to have onset of symptoms before age 45 years. [17].
Women are affected more commonly than men, in a ratio of almost 2:1. The increased risk of RLS in women is thought to be related to parity; nulliparous women have the same risk of developing RLS as men age-matched [17].
RLS affects African Americans less commonly than white individuals; this applies even to secondary RLS caused by hemodialysis [18].
The pathogenesis of RLS is not clear [2, 9-11]. Nowadays, Genetic sources are the most accepted mechanism about RLS, which lead to some abnormalities in the central subcortical dopamine pathways and impaired iron homeostasis [12, 13].
Results of single-photon emission computed tomography (SPECT) have shown a deficiency of dopamine D2 receptors in the brain. Iron homeostasis abnormalities have been implicated through cerebrospinal fluid (CSF) iron profile measures [14].
In addition, different researches have shown an increased severity of RLS with decreasing availability of serotonin transporter in the brainstem, which supports the hypothesis that increasing serotonin transmission in the brain may exacerbate RLS [14].
Diagnosis
Any person who suspected for RLS should be tested for iron deficiency [3, 4]. A complete iron panel should be checked, including:
- Iron levels
- Ferritin
- Transferrin saturation
- Total iron binding capacity
At least a Ferritin serum level has to be controlled if we could not check complete Iron profile, but due to falsely elevated level of ferritin in Acute Inflammatory states, complete Iron profile check is strongly recommended.
Other laboratory and para-clinically tests should be ordered If another sources for RLS are suspected according to the patient’s finding in history and general or neurologic examination, or poor response to RLS treatment. The commonest of these tests are:
- A complete blood count (CBC)
- Measurement of levels of the following:
- Blood urea nitrogen (BUN)
- Creatinine
- Fasting blood glucose
- Magnesium
- Thyroid-stimulating hormone (TSH)
- Vitamin B-12
- Folate
- Needle electromyography and nerve conduction studies: (Should be done if polyneuropathy or radiculopathy is suspected on clinical grounds, even if the results of the neurologic examination are apparently normal) [5, 24].
- Polysomnography: (can be done to quantify PLMS or to recognize sleep architecture, especially in children and in patients who continue to have significant sleep disturbances despite relief of RLS symptoms with treatment.)
Management
RLS could be treated and controlled by medications and/or nonpharmacological methods. Complete treatment is possible for secondary PLS, but there is no cure for primary type disease and Drugs with non-drug therapies are mainly symptomatic [8].
Medications used in the treatment of RLS include the following:
- Dopaminergic agents like Promipexole, Ropinirole, and Rotigotine [25-28].
- Benzodiazepines
- Opioids
- L-Dopa
- Anticonvulsants like Gabapentine [29].
- Presynaptic alpha2-adrenergic agonists [30].
- Iron salt [31].
- Glucocorticosteroids [33].
- Sleep hygiene measures
- Avoidance of caffeine, alcohol, and nicotine in patients with mild RLS who are sensitive to these substances
- Discontinuation, when possible, of medications that cause or exacerbate RLS, such as selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinepherine reuptake inhibitors (SNRIs), diphenhydramine, and dopamine antagonists
- Exercise (Physical modalities before bedtime, such as a hot or cold bath, whirlpool bath, limb massage, and vibratory or electrical stimulation of the feet and toes).
Education of patients with RLS and their families should focus on providing a better understanding of the disease and on emphasizing the importance of compliance for alleviating the symptoms [19-21].
Silber MH, Ehrenberg BL, Allen RP, et al. have arranged a useful algorithm for the management of restless legs syndrome[38].
Prognosis
In about two thirds of RLS patients, the symptoms progress over time. The severity of symptoms in patients with RLS ranges from mild to intolerable. In addition to being experienced in the legs, sensations also may occur in the arms or elsewhere. RLS symptoms are generally worse in the evening and night and less severe in the morning.
Whereas RLS may present early in adult life with mild symptoms, by age around 50 it usually progresses to severe symptoms; daily disruption of sleep leading to decreased daytime alertness. RLS has been associated with reduced quality of life in cross-sectional analysis [17, 19].
Patients with RLS and periodic leg movements of sleep (PLMS) may be at increased risk for hypertension. PLMS is associated with an autonomic surge and an increase in blood pressure [20].
Patients may also be more prone to headaches (migraine and tension- type). The headaches are probably secondary to disturbances in sleep associated with RLS and PLMS. Learning and memory difficulties have also been associated with RLS, presumably secondary to disrupted nocturnal sleep [20].
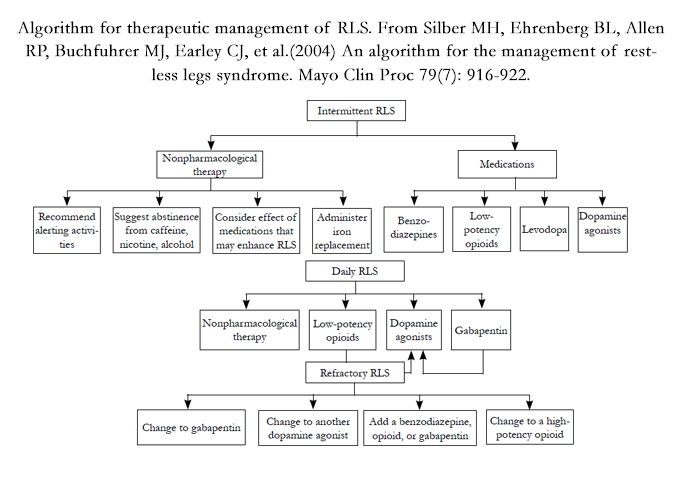
Algorithm for therapeutic management of RLS. From Silber MH, Ehrenberg BL, Allen RP, Buchfuhrer MJ, Earley CJ, et al. (2004) An algorithm for the management of restless legs syndrome. Mayo Clin Proc 79(7): 916-922.
Essential Update
The US Food and Drug Administration (FDA) have cleared a device for improving sleep in patients with primary RLS. It has given commercial clearance to the first device (Relaxis) for improvement of sleep quality in patients with primary RLS. The device, a vibrating pad, delivers vibratory counter-stimulation to the patient’s legs as an individual lies in bed. Approval was based on 2 randomized studies that showed greater improvements in sleep quality with the device than with a placebo pad [37].
References
- American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders. (5th edtn), Arlington. 410-413.
- Krueger BR (1990) Restless legs syndrome and periodic movements of sleep. Mayo Clin Proc 65(7): 999-1006.
- Gamaldo CE, Earley CJ (2006) Restless legs syndrome: a clinical update. Chest 130(5): 1596-1604.
- Hening WA (1999) Restless Legs Syndrome. Curr Treat Options Neurol 1(4): 309-319.
- Ferreri F, Rossini PM (2004) Neurophysiological investigations in restless legs syndrome and other disorders of movement during sleep. Sleep Med 5(4): 397-399.
- National Heart, Lung, and Blood Institute Working Group on Restless Legs Syndrome (2000) Restless legs syndrome: Detection and management in primary care. Am Fam Physician 62(1): 108-114.
- Evidente VG, Adler CH (1999) How to help patients with restless legs syndrome. Discerning the indescribable and relaxing the restless. Postgrad Med 105(3): 59-78.
- Silber MH (1997) Restless legs syndrome. Mayo Clin Proc 72(3): 261-264.
- Takaki J, Nishi T, Nangaku M, Shimoyama H, Inada T, et al. (2003) Clinical and psychological aspects of restless legs syndrome in Uremic patients onhemodialysis. Am J Kidney Dis 41(4): 833-839.
- Walters AS, LeBrocq C, Dhar A, Hening W, Rosen R, et al. (2003) Validation of the International Restless Legs Syndrome Study Group rating scale for restless legs syndrome. Sleep Med 4(2): 121-132.
- Weinstock LB, Walters AS, Paueksakon P (2012) Restless legs syndrome - Theoretical roles of inflammatory and immune mechanisms. Sleep Med Rev 16(4): 341-354.
- Winkelman JW (2006) Considering the causes of RLS. Eur J Neurol 13(Suppl 3): 8-14.
- Allen RP, Earley CJ (2001) Restless legs syndrome: a review of clinical and pathophysiologic features. J Clin Neurophysiol 18(2): 128-147.
- Jhoo JH, Yoon IY, Kim YK, Chung S, Kim JM, et al. (2010) Availability of brain serotonin transporters in patients with restless legs syndrome. Neurology 74(6): 513-518.
- Trenkwalder C, Hogl B, Winkelmann J (2009) Recent advances in the diagnosis, genetics and treatment of restless legs syndrome. J Neurol 256(4): 539-553.
- Cesnik E, Casetta I, Turri M, Govoni V, Granieri E, et al. (2010) Transient RLS during pregnancy is a risk factor for the chronic idiopathic form. Neurology 75(23): 2117-2120.
- Berger K, Luedemann J, Trenkwalder C, John U, Kessler C (2004) Sex and the risk of restless legs syndrome in the general population. Arch Intern Med 164(2): 196-202.
- Kutner NG, Zhang R, Huang Y, Bliwise DL (2012) Racial differences in restless legs symptoms and serum ferritin in an incident dialysis patient cohort. Int Urol Nephrol 44(6): 1825-1831.
- Abetz L, Allen R, Follet A, Washburn T, Earley C, et al. (2004) Evaluating the quality of life of patients with restless legs syndrome. Clin Ther 26(6): 925-935.
- Ekbom K, Ulfberg J (2009) Restless legs syndrome. J Int Med 266(5): 419- 431.
- Simakajornboon N, Kheirandish-Gozal L, Gozal D (2009) Diagnosis and management of restless legs syndrome in children. Sleep Med Rev 13(2): 149-156.
- Kotagal S, Silber MH (2004) Childhood-onset restless legs syndrome. Ann Neurol 56(6): 803-807.
- Lane RM (1998) SSRI-induced extrapyramidal side effects and akathisia: implications for treatment. J Psychopharmacol 12(2): 192-214.
- Hattan E, Chalk C, Postuma RB (2009) Is there a higher risk of restless legs syndrome in peripheral neuropathy? Neurology 72(11): 955-960.
- Montplaisir J, Nicolas A, Denesle R, Gomez-Mancilla B (1999) Restless legs syndrome improved by pramipexole: a double blind Randomized trial. Neurology 52(5): 938-943.
- Ondo W (1999) Ropinirole for restless legs syndrome. Mov Disord 14(1): 138-140.
- Giorgi L, Asgharian A, Hunter B (2013) Ropinirole in patients with restless legs syndrome and baseline IRLS Total Scores ≥ 24: Efficacy and tolerability in a 26-Week, Double-Blind, Parallel- Group, Placebo- Controlled Study followed by a 40-Week Open-Label Extension. Clin Ther 35(9): 1321-1336.
- Baldwin CM, Keating GM (2008) Rotigotine transdermal patch: in restless legs syndrome. CNS Drugs 22(10): 797-806.
- Bogan RK, Bornemann MA, Kushida CA, Trân PV, Barrett RW (2010) Long-term maintenance Treatment of restless legs syndrome with gabapentin enacarbil: a randomized controlled study. Mayo Clin Proc 85(6): 512-521.
- Garcia-Borreguero D, Kohnen R, Silber MH, Winkelman JW, et al. (2013) The long-term Treatment of restless legs syndrome/Willis-Ekbom disease: evidence-based guidelines and clinical Consensus best practice guidance: a report from the International Restless Legs Syndrome Study Group. SleepMed 14(7): 675-684.
- Grote L, Leissner L, Hedner J, Ulfberg J (2009) A randomized, double blind, placebo controlled, multi-center Study of intravenous iron sucrose and placebo in the treatment of restless legs syndrome. Mov Disord 24(10): 1445-1452.
- Shinno H, Yamanaka M, Ishikawa I, Danjo S, Nakamura Y, et al. (2010) Successful treatment of restless legs Syndrome with the herbal prescription Yokukansan. Prog Neuropsychopharmacol Biol Psychiatry 34(1): 252-253.
- Oscroft NS, Smith IE (2010) Oral Glucocorticosteroids: effective in a case of restless legs syndrome resistant to other therapies. Sleep Med 11(6): 596.
- Giannaki CD, Hadjigeorgiou GM, Karatzaferi C, Maridaki MD, Koutedakis Y, et al. (2013) A single blind Randomized controlled trial to evaluate the effect of 6 months of progressive aerobic exercise training in Patients with uraemic restless legs syndrome. Nephrol Dial Transplant 28(11): 2834-2840.
- Anderson P (2013) Restless Legs Syndrome Linked to Higher Mortality. Available at http://www.medscape.com/viewarticle/805712.
- Li Y, Wang W, Winkelman JW, Malhotra A, Ma J, et al. (2013) Prospective study of restless legs syndrome and Mortality among men. Neurology 81(1):52-59.
- Aurora RN, Kristo DA, Bista SR, Rowley JA, Zak RS, et al. (2012) The treatment of restless legs syndrome and periodic limb movement disorder in adults--an update for 2012: practice parameters with an evidence-based systematic review and meta-analyses: an American Academy of Sleep Medicine Clinical Practice Guideline. Sleep 35(8): 1039-1062.
- Garcia-Borreguero D, Kohnen R, Silber MH, Winkelman JW, Earley CJ (2013) The long-term treatment of restless legs syndrome/Willis–Ekbom disease: evidence-based guidelines and clinical consensus best practice guidance: a report from the International Restless Legs Syndrome Study Group. Sleep Med 14(7): 675-684.
- Silber MH, Ehrenberg BL, Allen RP, Buchfuhrer MJ, Earley CJ, et al. (2004) An algorithm for the management of restless legs syndrome. Mayo Clin Proc 79(7): 916-922.





