Effects of Flight-Exposure and Age on Cervical and Trunk Musculoskeletal Characteristics in Army Helicopter Pilots
Nagai T1*, Keenan KA1, Abt JP2, Sell TC3, Smalley BW4, Wirt MD5, Lephart SM2
1 Warrior Human Performance Research Center, University of Pittsburgh, Pittsburgh, PA, USA.
2 Sports Medicine Research Institute, University of Kentucky, Lexington, KY, USA.
3 Michael W. Krzyzewski Human Performance Laboratory, Duke University, Durham, NC, USA.
4 US Army Aeromedical Activity, Fort Rucker, AL, USA.
5 Eighth Army, US Army Garrison Yongsan, Korea.
*Corresponding Author
Takashi Nagai, PhD,
Warrior Human Performance Research Center,
University of Pittsburgh, Pittsburgh, PA 15203, USA.
Tel : 412-246-0472
Email: tnagai@pitt.edu
Received: September 02, 2016; Accepted: November 11, 2016; Published: November 16, 2016
Citation: Nagai T, Keenan KA, Abt JP, Sell TC, Smalley BW, et al. (2016) Effects of Flight - Exposure and Age on Cervical and Trunk Musculoskeletal Characteristics in Army Helicopter Pilots. Int J Aeronautics Aerospace Res. 3(5), 123-130. doi: dx.doi.org/10.19070/2470-4415-1600015
Copyright: Nagai T© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Due to flight-exposure and age, cervical and trunk musculoskeletal characteristics of military helicopter pilots may gradually deteriorate, increasing the risk of neck pain/low back pain. The purpose of this study was to compare cervical and trunk strength, flexibility, and posture among groups of pilots based on flight-exposure (total flight-hours) and age. A total of 115 male helicopter pilots participated in laboratory testing and were divided into five exposure-groups (EXP): EXP 1(0 – 999 hours, N=61), EXP 2 (1000 – 1999 hours, N=22), EXP 3 (2000 – 2999 hours, N=17), EXP 4 (3000 – 3999 hours, N=8), and EXP 5 (4000+hours, N=7). For age-related analyses, the same participants were divided into five age-groups (AGE): AGE 1 (20 – 24 years, N=10), AGE 2 (25 – 29 years, N=38), AGE 3 (30 – 34 years, N=26), AGE 4 (35 – 39 years, N=22), and AGE 5 (40+years, N=19). Laboratory testing included cervical and trunk muscular strength, cervical/lumbar spine range-of-motion (ROM), and postures. One-way analysis of variance or Kruskal-Wallis tests with post-hoc analyses were used to compare groups (p<0.05). When compared to the pilots in EXP 1 and 2, the pilots in EXP 3, 4, and 5 had significantly reduced cervical strength, cervical/lumbar spine ROM, and increased pectoralis minor tightness (p=0.001 – 0.049). Based on the analyses among the AGE groups, the pilots in AGE 5 had significantly less cervical/lumbar spine ROM and increased forward head/shoulder posture (p=0.001 – 0.042). The current findings confirmed exposure-/age-related musculoskeletal changes, especially pilots with over 3000 hours and 40+years. It is important for clinicians and pilots to implement strategic intervention programs to minimize exposure-/age-related decrements in an effort to reduce NP/LBP in pilots.
2.Introduction
3.Methods
3.1.Subjects
3.2.Equipment
3.3.Procedures
3.4.Statistical Analyses
4.Results
5.Discussion
7.Conclusion
8.Acknowledgment
9.References
Keywords
Neck Pain; Low Back Pain; Exposure; Age; Total Flight-Hours; Musculoskeletal Characteristics; Risk Factors; Helicopter Pilots; Military.
Introduction
Neck pain (NP) and low back pain (LBP) are the most prevalent musculoskeletal conditions among military helicopter pilots [1, 2]. The prevalence of NP in military helicopter pilots ranges from 56.6% to 84.5% with identified flight-related risk factors including poor posture, use of night vision goggles (NVG), and exposure to whole body vibration (WBV) contributing to NP and muscular fatigue [1]. Similarly, the prevalence of LBP in this population ranges from 50% to 92% with similar identified flight-related risk factors [2]. Associated short - and long-term medical leaves from duty negatively impact force readiness. Further, NP and LBP can negatively influence the quality of work and concentration while flying, potentially increasing mistakes and errors [3, 4].
Another important risk factor for NP/LBP is the cumulative effect of flight-exposure over their career (commonly reported as high total flight-hours and NVG flight-hours) [5, 6]. Pilots with higher total flight-hours and NVG flight-hours tend to be older. In addition to age-related changes in the musculoskeletal system, added stress of being military helicopter pilots (poor sitting posture, use of NVG, exposure to WBV, heavy protective gear (body armor with weapons/ammunitions/medical kits), and prolonged mission under intense stress) amplify muscular fatigue and could deteriorate the cervical and lumbar musculoskeletal systems, ultimately compromising the neuromuscular control and leading to a vicious cycle of chronic NP/LBP over their military careers [1,2].
Musculoskeletal characteristics such as cervical and trunk strength, flexibility, and posture have been investigated as modifiable risk factors of NP/LBP in military helicopter pilots [7,8]. One of the most important reasons for studying musculoskeletal risk factors is that these characteristics are modifiable through specific exercise programs, producing a long-lasting protective effect [9]. Based on a comprehensive testing battery of musculoskeletal characteristics, pilots with a history of NP and LBP had significantly less range-of-motion (ROM) and trunk extension strength when compared to age-matched pilots with no NP/LBP history [7, 8]. No significant differences were found in other characteristics such as cervical proprioception, the upper quadrant posture, scapular muscle strength, and hip ROM [7, 8].
To date, few studies have been conducted to examine effects of military career (age or years of service) on musculoskeletal and physiological characteristics in military populations [10]. Soldiers over 30 years of age or with 11+ years of military service were found to have significantly higher body fat and lower aerobic capacity [10]. These findings, along with those investigating NP/ LBP risk factors, highlight the importance of investigating modifiable musculoskeletal risk factors of NP/LBP among military helicopter pilots with different flight-exposure (total flight-hours) and age. The reason for evaluating pilots with different total flight-hours and age is that total flight-hours vary among older pilots due to their assignments. For example, test/safety pilots have more flight-hours while Commanders/Officers have less flight-hours due to reduced frequency of flight missions (personal communication with senior pilots and flight surgeons). Another reason is that early signs of osteoarthritis progression were found in fighter-jet pilots compared to age-matched non-pilots [11]. Flight-exposure and age may indeed have different effects on musculoskeletal characteristics among military helicopter pilots.
The purpose of the study was to examine the effects of total flight-hours and age on cervical and trunk musculoskeletal characteristics. It is hypothesized that pilots with higher total flighthours and older pilots would exhibit lower strength and flexibility as well as poorer posture when compared to pilots withless flight-hours and younger pilots. If significant exposure- and age-related changes in musculoskeletal characteristics are found, then it is possible to address decrements in these musculoskeletal characteristics through individualized intervention programs based on pilots’ total flight-hours and age, potentially mitigating the incidence and severity of NP/LBP. A similar approach to target specific suboptimal musculoskeletal characteristics through interventions has been proven to effectively reduce musculoskeletal injuries in US Army Soldiers [12].
This cross-sectional cohort study was approved by the Internal Review Board from the Eisenhower Army Medical Center and the University of Pittsburgh. Inclusion criteria were: active flightstatus (passed annual physical exam and no restriction on physical training); aged 18 to 55 years; no history of concussion or mild head injury in the past 12 months; no neurological or balance disorders; and no current spinal, upper limb, or lower limb impairment that could affect test performance. Laboratory testing was conducted in a single two-hour session and included isometric cervical muscular strength and isokinetic trunk muscular strength, cervical/lumbar spine ROM, and forward head/shoulder posture assessment. Convenient sampling was used. A total of 115 pilots were tested as a part of comprehensive injury prevention and performance optimization research initiative with the University of Pittsburgh and the 101st Airborne Division (Air Assault). Demographic information and flight characteristics were collected for both exposure-and age-related analyses (Tables 1 & 2). Pilots were divided into five groups based on flight-exposure (total flight-hour): EXP 1 (0 – 999 hours, N=61), EXP 2 (1000 – 1999 hours, N=22), EXP 3 (2000 – 2999 hours, N=17), EXP 4 (3000 – 3999 hours, N=8), and EXP 5 (4000+hours, N=7). For agerelated analyses, pilots were divided into five groups based on age: AGE 1 (20–24 years, N=10), AGE 2 (25–29 years, N=38), AGE 3 (30–34 years, N=26), AGE 4 (35–39 years, N=22), and AGE 5 (40+years, N=19). As this study was a preliminary study, only pilots were included in this study, and no control groups (agematched non-pilots) were recruited and examined.
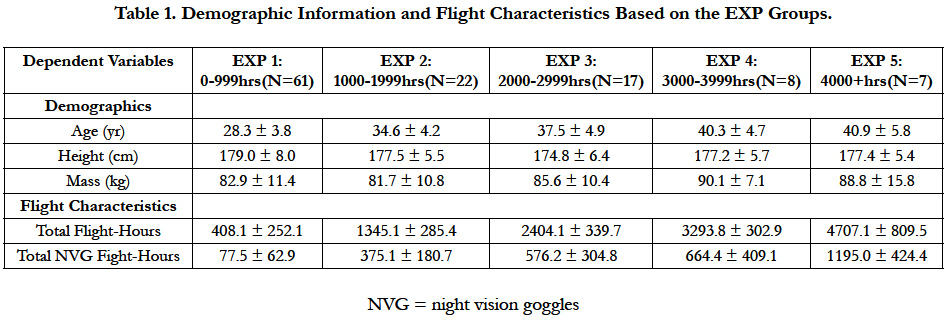

Table 1. Demographic Information and Flight Characteristics Based on the EXP Groups.
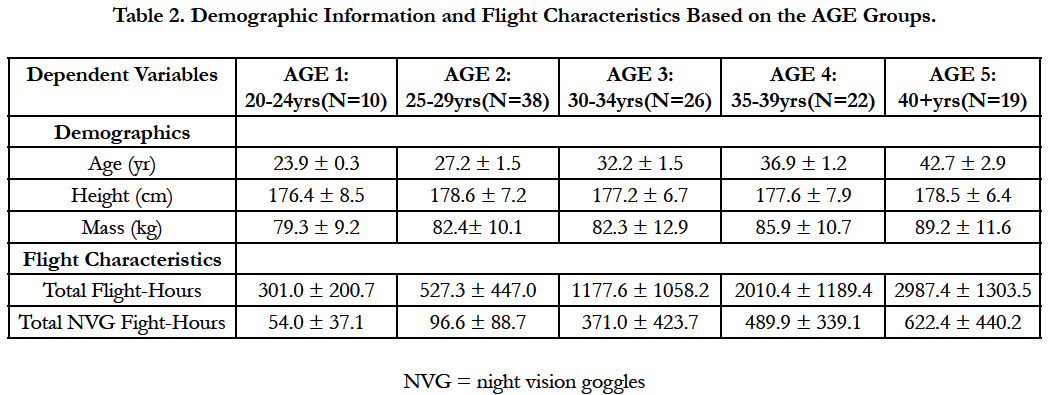
Table 2. Demographic Information and Flight Characteristics Based on the AGE Groups.
Height and body mass were measured using a standard stadiometer and scale (Seca North America, East Hanover, MD). Isometric cervical muscle strength (flexion, extension, right/left lateral flexion, and right/left rotation) was measured using a Lafayette handheld dynamometer (HHD; Lafayette Instruments, Lafayette, IN). Trunk flexion, extension, and rotation strength were measured using the Biodex Multi-Joint System 3 Pro (Biodex Medical Systems, Inc, Shirley, NY). Cervical spine active ROM (flexion, extension, right/left lateral flexion, right/left rotation) and forward head posture were measured using the CROM 3 (Performance Attainment Associates, Lindstrom, MN). Lumbar spine ROM was measured using a digital inclinometer (The Saunders Group Inc, Chaska, MN). Forward shoulder posture and pectoralis minor length were measured with a modified 16 inch Swanson combination square (Swanson Tool Co., Frankfort, Illinois).
Pilots reported to the Warrior Human Performance Laboratory and written informed consent was obtained from each pilot. Selfreported flight characteristics (total flight-hours and total NVGhours) were collected at the same time. Height and mass were measured. Pilots then were asked to perform the cervical/trunk strength, flexibility, and posture testing. The reliability of the testing procedures described here have been examined and reported previously [7, 8].
For cervical flexion, lateral flexion, and rotation strength testing, pilots were supine with the feet hip-width apart, hands resting on the abdomen, and pillows placed under the knees. The HHD was applied on the midline of the forehead, above the ear, or on the temporal line of the frontal bone for cervical flexion,lateral flexion,and rotation strength testing, respectively. For lateral flexion testing, a second examiner stabilized the opposite shoulder during testing. During the cervical extension testing, pilots were prone with a prone pillow under the face and the HHD was applied over the occiput. For all cervical strength testing, pilots performed two warm-up trials at 50% of self-perceived maximal effort for 5 seconds and two trials at 100% effort. Three maximal effort trials were collected with 60 seconds rest between trials, and an average peak force of the three trials was normalized to body weight (% BW) for data analysis.
For trunk flexion, extension, and rotation strength measurements, pilots were seated on the trunk attachment and stabilized according to the manufacturer’s guidelines to ensure proper alignment for testing and to restrict accessory movements. All warm-up and test trials were reciprocal concentric isokinetic trunk extension/ flexion and right/left trunk rotation contractions collected at 60°/sec. Pilots performed three warm-up trials at 50% of selfperceived maximal effort and then three warm-up trials at 100% effort. Five maximum effort trials were collected following a one minute rest. The average peak torque of the five trials for each direction was normalized to body weight (% BW) and used for data analysis.
For cervical active ROM (flexion, extension, lateral flexion, and rotation), pilots were seated in a chair wearing the CROM. The elbows were flexed to 90° and positioned so that the forearms were supported by cushions on top of the chair armrests. Three practice trials were followed by three measured trials. Pilots were instructed to turn the head while following the horizontal line on the wall. An absolute angle (in degrees) from the neutral position was recorded for three trials and an average of three trials was used for analysis.
For lumbar spine flexion ROM, pilots were seated on a chair and were asked to actively forward flex, trying to reach the knees with the nose. For lumbar spine extension ROM, pilots were in the prone position and pushed down on the table with the hands and actively arched the trunk into extension while the anterior superior iliac spines maintained contact with the table. For lumbar spine lateral flexion ROM, pilots were standing and actively slid the hand down the lateral aspect of the thigh. For lumbar spine rotation ROM, pilots were in a stooped position (trunk flexed to 90°). Pilots actively rotated the trunk to the right or the left, with right side rotation operationally defined as rotating the right shoulder up. For all lumbar spine ROM measurements, three practice trials were followed by three measured trials. An average of three trials was used for statistical analyses.
For forward head posture, pilots were seated in a chair with the CROM and the forward head attachment. The foot of the vertical arm was placed on the spinous process of the 7th cervical vertebrae, and the vertical arm intersected with the horizontal arm. An examiner read and recorded the value on the horizontal arm. For standing forward shoulder posture, pilots were in a standing position with the feet together and buttocks just touching the wall. The combination square was placed above the shoulder to measure the horizontal distance between the anterior tip of the acromion process and the wall. For pectoralis minor length testing, pilots were in a supine position and the combination square was placed on the table to measure the vertical distance between the posterior tip of the acromion and the table surface. For all postural assessments, an average of three measures (in centimeters) was calculated and used for analyses.
All statistical analyses were performed using SPSS 20.0 (IBM Corporation, Armonk, NY). Descriptive statistics were calculated for all variables. Each dependent variable within each group was assessed for normality and homogeneity of variance. One-way analysis of variance (ANOVA) or Kruskal-Wallis tests (for nonnormal data) and Bonferroni post-hoc analyses were used to compare between the groups. Statistical significance was set at p < 0.05 a priori.
Results
Means and standard deviations for cervical strength, trunk strength, cervical ROM, lumbar spine ROM, and posture are presented in Tables 3 and 4. A few strength variables (cervical rotation, trunk extension, and trunk rotation), several ROM (cervical flexion, cervical lateral flexion, cervical rotation, lumbar spine flexion, lumbar spine extension, lumbar lateral flexion, and lumbar spine rotation) and postural measurements (forward head posture, forward shoulder posture, and pectoralis minor tightness) were not normally distributed; therefore, Kruskal-Wallis tests were performed (Tables 3 & 4).
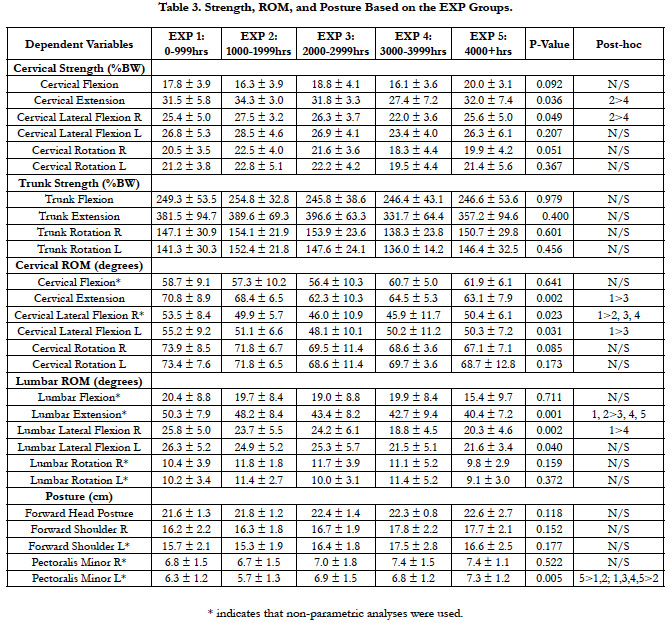
Table 3. Strength, ROM, and Posture Based on the EXP Groups.
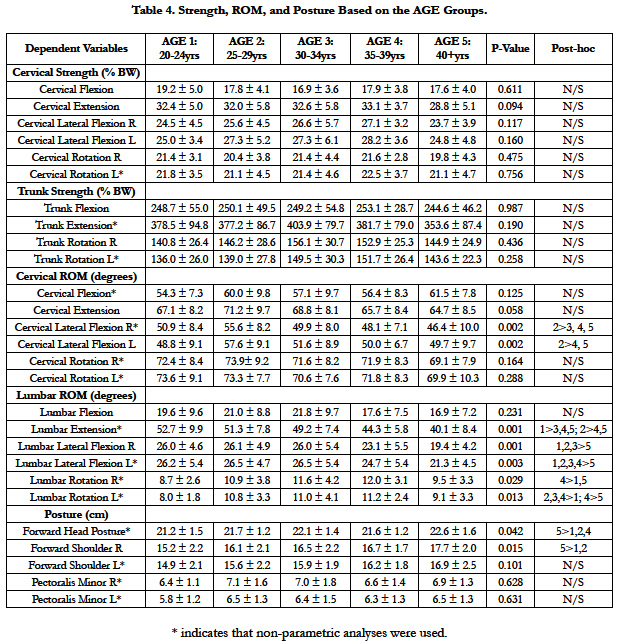
Table 4. Strength, ROM, and Posture Based on the AGE Groups.
Cervical extension and right lateral flexion strength were significantly different among the EXP groups (p = 0.036 and p = 0.049, respectively). Post-hoc analyses revealed that EXP 2 was significantly stronger than EXP 4 for cervical extension strength (p = 0.020) and right lateral flexion strength (p = 0.033). Trunk strength was not significantly different among the EXP groups (p > 0.05). Similarly, there were no significant differences among the AGE groups in cervical or trunk strength (p > 0.05).
Cervical extension ROM and cervical lateral flexion ROM were significantly different among the EXP groups (p = 0.002 – 0.031). Post-hoc analyses revealed that EXP 1 was significantly more flexible than EXP 3 for cervical extension ROM (p = 0.004) and left cervical lateral flexion ROM (p = 0.046). Further, EXP 1 was significantly more flexible than EXP 2, 3, and 4 for right cervical lateral flexion (p = 0.011 – 0.047).
Similarly, cervical lateral flexion ROM were significantly different among the AGE groups (p = 0.002). Post-hoc analyses revealed that AGE 2 was more flexible than AGE 3, AGE 4, and AGE 5 towards the right(p = 0.001 – 0.007) and more flexible than AGE 4 and AGE 5 towards the left (p = 0.015 – 0.017).
Lumbar spine extension ROM and lateral flexion ROM were significantly different among the EXP groups (p = 0.001 – 0.040). Post-hoc analyses revealed that EXP 1and 2 were significantly more flexible than the EXP 3, 4, and 5 for lumbar spine extension ROM (p = 0.001 – 0.048). For right lumbar spine lateral flexion ROM, EXP 1 was significantly more flexible than EXP 4 (p = 0.005). Although the ANOVA was significant for left lateral flexion ROM (p = 0.040), post-hoc analyses did not reveal any significant differences.
Similarly, lumbar spine extension ROM, lateral flexion ROM, and lumbar rotation ROM were significantly different among the AGE groups (p = 0.001 – 0.029). Post-hoc analyses revealed that AGE 1 was significantly more flexible than AGE 3, 4, and 5 for lumbar spine extension ROM (p = 0.002 – 0.049). In addition, AGE 2 was significantly more flexible than AGE 4 and 5 (p = 0.001). For right lumbar spine lateral flexion ROM, AGE 1, 2, and 3 were significantly more flexible than AGE 5 (p = 0.001 – 0.010). For left lumbar spine lateral flexion ROM, AGE 1, 2, 3, and 4 were significantly more flexible than AGE 5 (p = 0.001 – 0.015). For right lumber spine rotation ROM, AGE 4 was significantly more flexible than AGE 1 and AGE 5 (p = 0.005 – 0.015). For right lumbar spine rotation ROM, AGE 2, 3, and 4 were significantly greater than AGE 1 (p = 0.001 – 0.037), while AGE 4 was significantly more flexible than AGE 5 (p = 0.029).
Forward head and forward shoulder postures were not significantly different among the EXP groups (p > 0.05). Pectoralis minor tightness on the left side was significantly different among the EXP groups (p = 0.005). Post-hoc analyses revealed that EXP1 and 2 had significantly less tightness than EXP 5 (p = 0.005 – 0.042). Additionally, EXP 2 had significantly less tightness than all other EXP groups (p = 0.005 – 0.042).
Forward head and right forward shoulder postures were significantly different among the AGE groups (p = 0.015 – 0.042). Posthoc analyses revealed that AGE 1, 2, and 4 had significantly less forward head posture than AGE 5 (p = 0.016 – 0.031). AGE 1 and 2 had significantly less right forward shoulder than AGE 5 (p = 0.019 – 0.042). Other postural variables were not significant among the AGE groups (p > 0.05).
Discussion
This study investigated the effects of flight-exposure and age on cervical and trunk musculoskeletal characteristics. Soldiers from different age (mostly 20-30 years old) enter the flight school to become helicopter pilots, and total cumulative flight-hours can be quite different among the pilots with similar age due to various reasons (deployment schedule, operational tempo, mission frequency/duration, assigned units/tasks, rank/occupations, etc). Therefore, it is important to include both total-flight hours and age in this study. A lack of significant differences on trunk strength among the EXP groups and both cervical and trunk strength among the AGE groups were contrary to the hypotheses. There were few significant differences on cervical strength (two out of six), cervical/lumbar ROM (five out of twelve), and posture (one out of six) among the EXP groups. Similarly, there were few significant differences on cervical/lumbar ROM (seven out of twelve) and posture (two out of six) among the AGE groups. Therefore, the hypotheses were partially supported on those variables. The results are clinically important because it provides normative values of the cervical and trunk musculoskeletal characteristics among military helicopter pilots with different total flight-hours and age. In turn, the results can also be used to formulate exposure-specific intervention programs for this population.
A reduction in cervical extension and lateral flexion strength was reported among a group of fighter-jet pilots with a history of NP when compared to their counterparts without a history of NP [13, 14]. In contrast, no significant differences in cervical strength were found between helicopter pilots with and without a history of NP [8, 14, 15]. Fighter-jet pilots must stabilize the cervical spine in a high acceleration environment; therefore, cervical strength may likely play a larger role in fight-jet pilots. In the current study, based on cervical strength values across the EXP groups, there were no general trends for a decline in strength. Rather, the pilots in EXP 4 (3000 – 3999 hours) seem to demonstrate less strength. It is not clear as to what factors are related to the current findings. One potential reason is influence of drop-outs in this group (EXP 4: 3000 – 3999 hours). Since all pilots had to be medically cleared for flight duty, pilots with severe NP/LBP would not be in our study. Some pilots with consistent NP might have chosen to retire or opted not to fly. Based on the cervical strength values in EXP 5 (4000+hours), the pilots with the highest total flight-hour are as strong (if not stronger) as the pilots with less total flight-hours.
Cervical strength was not significantly different among the AGE groups. However, there was a slight reduction in cervical extension and lateral flexion in AGE 5. When combined with the results based on the EXP groups, pilots and medical care providers can anticipate a reduction in cervical strength in pilots with over 3000 total flight-hours and who are over 40 years. In turn, specific interventions may be beneficial. For future studies, muscular endurance testing and deep muscle testing should be incorporated and may detect those pilots at higher risk of NP as the cervical muscles in helicopter pilots with a history of NP have been shown to fatigue faster when compared to helicopter pilots without a history of NP [14]. Also, from a clinical perspective, two intervention studies that incorporated exercises to strengthen the deep cervical muscle and improve muscular endurance have shown to be effective in reducing NP in helicopter and fighter-jet pilots [9, 16].
Trunk strength did not significantly differ among the EXP and AGE groups in the current investigation. However, when you look at their trunk extension strength values closely, there is a 16% and 10% decrease in EXP 4 (331.7% BW) and EXP 5 (357.2% BW), respectively, when compared to EXP 3 (396.6% BW). In our previous study using the same testing procedures, we have identified that helicopter pilots with a history of LBP had significantly lower trunk extension strength than age-matched pilots without a history of LBP (LBP: 351.3%BW, No-LBP: 405.2% BW, p = 0.008) [7]. Based on these collective findings, trunk extension strength values from EXP 4 and EXP 5 resemble the suboptimal characteristics of pilots with a history of LBP. Based on the AGE groups, the pilots in AGE 5 had less trunk extension strength (353.6% BW): the strength value was similar to those pilots with a LBP history (351.3% BW). Trunk extension strength is important in the development/ prevention of LBP. In civilian prospective studies, weaker trunk extension strength was associated with future incidence of LBP [17, 18]. From a clinical perspective, resistance training to strengthen the trunk extension muscles should be implemented at least prior to reaching 3000 total flight-hours and 40 years of age. Other trunk strength measures seemed to be similar among groups. As stated above, future studies could expand the current findings and examine trunk muscular endurance [19, 20].
Three out of six cervical ROM variables were significantly different among the EXP groups. The pattern of group differences in all cervical ROM measurements seems to be similar. There was a significant reduction in cervical extension and lateral flexion from vEXP 1 to EXP 2 or EXP 3. Based on the mean age for the EXP groups (Table 1), there is only 6.3 years and 9.2 years difference from EXP 1 to EXP 2 and EXP 3, respectively. In other words, in a relatively short period of time, pilots exhibited a 12 – 14% reduction in cervical extension and lateral flexion ROM. Based on the AGE groups, cervical ROM seems to peak between the ages of 25 – 29 years and the declines. Cumulatively, this information indicates that the onset of cervical ROM reduction may occur around the age of 30 years and 2000 total flight-hours. Our previous investigation on cervical ROM between helicopter pilots with and without a history of NP demonstrated overall reductions in cervical ROM in all directions in pilots with a history of NP [8]. A similar finding was reported in fighter-jet pilots with a history of NP [21]. Further, cervical flexion-extension and rotation ROM was sensitive enough to discriminate helicopter pilots with acute ongoing pain on the visual analog scale (VAS: greater than 10 out of 100) and helicopter pilots with subacute pain (VAS: less than 10 out of 100) at the time of testing [22]. Although none of these studies, including the current study, could establish the cause-andeffect relationship, reduced cervical ROM seems to bea common sign among helicopter pilots with higher total flight-hours or a history of NP.
Similar to the cervical ROM results, three out of six lumbar spine ROM variables were significantly different among the EXP groups. Decreased lumbar spine ROM was more noticeable in EXP 4 or EXP 5. The lumbar spine might require longer exposure than the cervical spine to see negative effects in ROM. All lumbar spine ROM except flexion were significantly different among the AGE groups. Noticeably, AGE 5 had significantly less lateral flexion and rotation ROM when compared to AGE 4. Interestingly, both trunk strength and lumbar spine ROM exhibited this ‘delayed onset’ in decline. Although it is ‘delayed onset’ in military helicopter pilots, it could be considered as ‘early onset’ of diminished lumbar spine ROM as significant reductions in lumbar spine ROM typically occur around 50 – 60 years of age in the civilian population [23]. Furthermore, military pilots with a history of LBP exhibit reduced lumbar spine ROM [7]. When the results in the current investigation were carefully examined, the lumbar spine flexion, extension, and lateral flexion ROM values in EXP 4, EXP 5, and AGE 5 were worse than the values in pilots with a history of LBP in our previous investigation [7]. As commented earlier, it is imperative to begin incorporating stretching exercise in pilots’ physical fitness program or as a part of post-flight cool down.
Lastly, for postural measurements, only one variable (left pectoralis minor tightness) was significantly different among the EXP groups. Pectoralis minor tightness had a tendency to get worse (larger values) in EXP 5. Based on the AGE groups, the AGE 5 had poorer forward head posture and forward shoulder posture than younger groups. Poor sitting posture was thought to be a contributing factor of NP in helicopter pilots due to a confined cockpit [24]. As described in the previous review paper [25], helicopter pilots fly with ‘halo hunch’ with their neck retracted and their shoulder/arm tilted down when holding a control lever. This position potentially could explain the current findings. However, the results should be interpreted cautiously as the previous study failed to find the association between the pilots with a history of NP and poor posture [8].
There are limitations in the current study. This study was a crosssectional design. In order to truly track the influence of flight-exposure and age on musculoskeletal characteristics, a longitudinal study design is more appropriate. A longitudinal study also has its limitations such as time, cost, and loss of follow-up. Given the facts on higher NP/LBP prevalence and deteriorating musculoskeletal characteristics among military pilots with higher total flight-hours and age, we believe that the current study design and findings have merit. Another limitation is a small sample size, only male pilots, and a lack of age-matched non-pilot control groups in this study. When recruiting military pilots, their missions must come first, in other words, not many helicopter pilots were available at the time of the study to be tested due to their deployment schedule; therefore, convenient sampling was used in this study. Based on gender differences in musculoskeletal characteristics in the Army helicopter pilots [26], a group of female pilots with different exposures might results in different findings. To address these limitation, more experienced pilots and female pilots should be recruited in future investigations. Lastly, a lack of age-matched non-pilot control groups is a major limitation of the study. It is important to compare age-matched pilots and non-pilots to evaluate if the current findings are related to the occupation (flightexposures) or age.
Conclusion
The current findings confirmed exposure- and age-related musculoskeletal changes, especially pilots with over 3000 hours and 40+years. The current investigation is clinically significant because the results establish normative values for cervical and trunk strength, ROM, and posture among helicopter pilots with different total flight-hours and age, allowing for the incorporation of specific exercise intervention throughout their military career in an attempt to prevent a decrement in these characteristics. Although it is not a part of the study, it is generally accepted that increases in body fat/weight as well as overall physical fitness and health should be monitored and used to develop/design customized intervention programs. A scientifically formulated intervention program has been shown to be effective in reducing musculoskeletal injuries [12]; therefore, we would anticipate similar effectiveness in this population.
Acknowledgment
This study was supported by the U.S. Army Medical Research and Materiel Command under Award No. W81XWH-11-2-0097. Opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by the U.S. Army. The authors do not have a conflict of interest to disclose.
References
- Salmon DM, Harrison MF, Neary JP (2011) Neck pain in military helicopter aircrew and the role of exercise therapy. Aviat Space Environ Med. 82(10): 978-987.
- Gaydos SJ (2012) Low back pain: considerations for rotary-wing aircrew. Aviat Space Environ Med. 83(9): 879-889.
- Thomae MK, Porteous JE, Brock JR, Allen GD, Heller RF (1998) Back pain in Australian military helicopter pilots: a preliminary study. Aviat Space Environ Med. 69(5): 468-473.
- Ang B, Harms-Ringdahl K (2006) Neck pain and related disability in helicopter pilots: A survey of prevalence and risk factors. Aviat Space Environ Med. 77: 713-719.
- Van den Oord MH, De Loose V, Meeuwsen T, Sluiter JK, Frings-Dresen MH (2010) Neck pain in military helicopter pilots: prevalence and associated factors. Mil Med 175: 55-60.
- Bongers PM, Hulshof CT, Dijkstra L, Boshuizen HC, Groenhout HJ, et al. (1990) Back pain and exposure to whole body vibration in helicopter pilots. Ergonomics. 33(8): 1007-1026.
- Nagai T, Abt JP, Sell TC, KeenanKA, Clark NC, et al. (2015) Lumbar spine and hip flexibility and trunk strength in helicopter pilots with and without low back pain history. Work . 52(3): 715-722.
- Nagai T, Abt JP, Sell TC, Clark NC, Smalley BW, et al. (2014) Neck proprioception, strength, flexibility, and posture in pilots with and without neck pain history. Aviat Space Environ Med. 85(5): 529-535.
- Ang BO, Monnier A, Harms-Ringdahl K (2009) Neck/shoulder exercise for neck pain in air force helicopter pilots: a randomized controlled trial. Spine. 34(16): E544-551.
- Abt JP, Perlsweig K, Nagai T, Sell TC, Wirt MD, et al. (2016) Effects of Age and Military Service on Strength and Physiological Characteristics of U.S. Army Soldiers. Mil Med. 181(2): 173-179.
- Petren-Mallmin M, Linder J (1999) MRI cervical spine findings in asymptomatic fighter pilots. Aviat Space Environ Med. 70: 1183-1188.
- Sell TC, Abt JP, Nagai T, Deluzio JB, Lovalekar M, et al. (2016) The Eagle Tactical Athlete Program Reduces Musculoskeletal Injuries in the 101st Airborne Division (Air Assault). Mil Med. 181(3): 250-257.
- Lecompte J, Maisetti O, Guillaume A, Skalli W, Portero P (2008) Neck strength and EMG activity in fighter pilots with episodic neck pain. Aviat Space Environ Med. 79(10): 947-952.
- Ang B, Linder J, Harms-Ringdahl K (2005) Neck strength and myoelectric fatigue in fighter and helicopter pilots with a history of neck pain. Aviat Space Environ Med. 76(4): 375-380.
- Van den Oord M H, De Loose V, Sluiter JK, Frings-Dresen MH (2010) Neck strength, position sense, and motion in military helicopter crew with and without neck pain. Aviat Space Environ Med. 81(1): 46-51.
- Lange B, Toft P, Myburgh C, Sjogaard G (2013) Effect of targeted strength, endurance, and coordination exercise on neck and shoulder pain among fighter pilots: a randomized-controlled trial. Clin J Pain. 29(1): 50-59.
- Cho KH, Beom JW, Lee TS, Lim JH, Lee TH, et al. (2014) Trunk muscles strength as a risk factor for nonspecific low back pain: a pilot study. Ann Rehabil Med. 38(2): 234-240.
- Lee JH, Hoshino Y, Nakamura K, Kariya Y, Saita K, et al. (1999) Trunk muscle weakness as a risk factor for low back pain. A 5-year prospective study. Spine. 24(1): 54-57.
- Biering-Sorensen F (1984) Physical measurements as risk indicators for lowback trouble over a one-year period. Spine. 9(2): 106-119.
- McGill S, Grenier S, Bluhm M, Preuss R, Brown S, et al. (2003) Previous history of LBP with work loss is related to lingering deficits in biomechanical, physiological, personal, psychosocial and motor control characteristics. Ergonomics. 46(7): 731-746.
- De Loose V, Van den Oord M, Burnotte F, Van Tiggelen D, Stevens V, et al. (2009) Functional assessment of the cervical spine in F-16 pilots with and without neck pain. Aviat Space Environ Med. 80(5): 477-481.
- Ang BO (2008) Impaired neck motor function and pronounced pain-related fear in helicopter pilots with neck pain - a clinical approach. J Electromyogr Kinesiol. 18(4): 538-549.
- Intolo P, Milosavljevic S, Baxter DG, Carman AB, Pal P, et al. (2009) The effect of age on lumbar range of motion: a systematic review. Man Ther. 14(6): 596-604.
- Forde KA, Albert WJ, Harrison MF, Neary JP, Croll J, et al. (2011) Neck loads and posture exposure of helicopter pilots during simulated day and night flights. Int J IndErgon. 41: 128-135.
- Pelham TW, White H, Holt LE, Lee SW (2005) The etiology of low back pain in military helicopter aviators: prevention and treatment. Work . 24(2): 101-110.
- Nagai T, Keenan KA, Abt JP, Sell TC, Smalley BW, et al. (2016) A comparison of cervical and trunk musculoskeletal characteristics between female and male Army helicopter pilots. Int J Aviat AeronauticsAerospace. 3(3): 1-14.





