Unilateral Labial Hypertrophy in Adolescents: when should we Interfere? Two Case Reports
Gihan M. Bareh*, Randal D. Robinson, Sheena Rippentrop, KathrynS. Holloway, Nichole Budrys, Robert S. Schenken
Department of Obstetrics and Gynecology, University of Texas Health Science Center at San Antonio7703 Floyd Curl Drive, San Antonio, TX 78229,USA.
*Corresponding Author
Gihan M. Bareh, M.D, Ph.D.
Department of Obstetrics and Gynecology,
University of Texas Health Science Center at San Antonio,
7703 Floyd Curl Drive, San Antonio, TX 78229, USA.
Tel: 210-567-4920
Fax: 210-567-3093
E-mail: drgihanmansour@yahoo.com
Article Type: Case Report
Recieved: October 27, 2014; Accepted: November 05, 2014; Published: November 07, 2014.
Citation: Gihan M. Bareh, et al., (2014) Unilateral Labial Hypertrophy In Adolescents: When Should We Interfere?Two Case Reports. Int J Reprod Fertil Sex Health, 1(4), 25-27. doi: dx.doi.org/10.19070/2377-1887-140005
Copyright: Gihan M. Bareh© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Synopsis: Adolescent and pre-menarchal patients with symptomatic unilateral labial hypertrophy should be counselled extensively prior to surgical management regarding risks of recurrence or contralateral occurrence.
Purpose:Present the management of two unique cases of adolescent girls with unilateral labial hypertrophy.
Case 1: 9 year-old pre-menarchal patient with a five-month history of unilateral labial hypertrophy causing discomfort that limited daily activities. External pelvic examination revealed grossly asymmetric labia minora. The left labia minora measured 5 cm in length. After counseling, the patient underwent unilateral labioplasty with resolution of symptoms. Patient returned after two years complaining of contralateral labial hypertrophy.The patient again underwent surgical management due to discomfort and interference with normal daily activities.
Case 2: 12 year-old post-menarchal patient with a history of unilateral labial hypertrophy causing irritation and discomfort starting prior to menarche. External pelvic exam revealed grossly asymmetric labia minora. The right labia minora measured 4.5cm in length. The patient underwent unilateral labioplasty with resolution of her symptoms. After 2 years of follow up,patient remained asymptomatic.
Conclusion: Adolescence unilateral labial hypertrophy may represent a normal variant and surgery should be delayed until achieving full puberty. However, when it causes significant discomfort or interferes with normal daily activities, surgical management should be considered after counseling regarding recurrence or contralateral occurrence.
2.Introduction
3.Materials and Methods
3.1.Statistical Analysis
4.Results
5.Discussion
6.Acknowledgments
7.References
Keywords
adolescence; unilateral labial hypertrophy; premenarchal; labioplasty
Introduction
Normal development of the female external genitalia results in a diverse range of anatomy. Labia minora extending beyond the labia majora may represent a normal variant, but excessive tissue may cause irritation, pruritus, dyspareunia, dysuria, andanxiety [1,2]. Surgical resection is the only treatment which alleviates symptoms associated with labial hypertrophy.
Increasing availability and awareness of reductive labioplasty has led to a corresponding increase in case reports. A literature review revealed primarily cases of bilateral hypertrophyin adults (Pubmed search from 1987–2014 of: labial hypertrophy, unilateral labial hypertrophy, adolescent labial hypertrophy, labial reconstruction) [2]. Three case series involved adolescent patients presenting for unilateral labial reduction, but none discuss this condition in pre-menarchal girls [2-4]. We present the management of unilateral labial hypertrophy in two adolescent patients pre and post menarchal.
Case Report 1
A nine-year-old pre-menarchal female presented with an enlarging left labia minora. The patient’s mother reported that her daughter complained of discomfort as that the labial skin had begun to lengthen and appeared irritated and dry. The patient reported that she needed to “tuck in” the excess skin in order to urinate, also was unable to form fitted clothing. Patient had no family history of similar condition. External pelvic examination revealed normal female external genitalia, Tanner stage 2 pubic hair with grossly asymmetric labia minora. The right labial minora measured 0.5cm, consistent with pre-menarchal development. The left labia minora measured five centimeters in length with thickened darkly pigmented skin consistent with chronic irritation (Figure 1A). The patient and family were counseled regarding the risks and benefits of observation versus surgical reduction. The risks of labioplasty were reviewed including infection, bleeding, unsatisfactory cosmetic appearance, and recurrence secondary to continued growth or regrowth.The patient and family requested surgical management.
Labioplasty was performed under general anesthesia in the usual manner. The edges were reapproximated with 3-0 vicryl interrupted sutures.(Figure 1B). The patient tolerated the procedure well and was discharged the same day. Histological examination revealed benign labial tissue with chronic irritation.
Post-operative follow up confirmed that the patient was very satisfied with the outcome; however, she presented with symptomatic right labial hypertrophy 2 years later.She had undergone menarche at the age of 11. After counseling, the patient and parents insisted on surgical management. Labioplasty was performed and bilateral labial symmetry achieved. Follow up revealedno recurrence. The patient and parents were satisfied with the results.
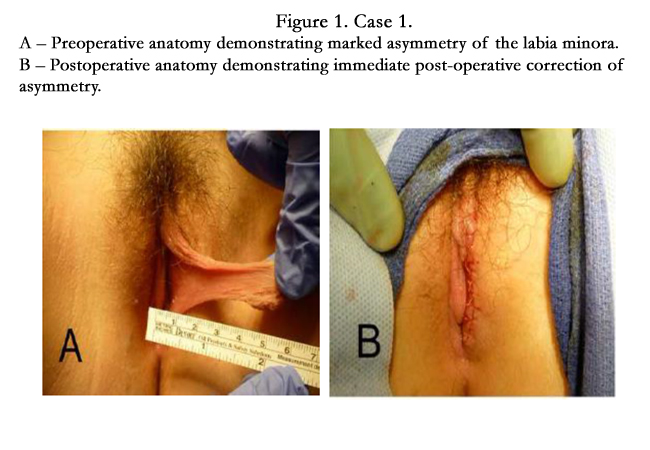

Figure 1. Case 1. A – Preoperative anatomy demonstrating marked asymmetry of the labia minora.
B – Postoperative anatomy demonstrating immediate post-operative correction of asymmetry.
Case Report 2
A twelve-year-old female presented with complaints of excess tissue that had been present for three years pre-menarchal. She described worsening discomfort when the area rubbed on clothing. This was exacerbated by wearing pads during her menses, as the area became inflamed, edematous, and pruritic. The patient was concerned about hygiene and reported that the tissue had become so irritated that she threatened self-mutilation. No family history of similar condition.
Physical exam revealed normal external female genitalia with Tanner stage 4 development. The left labia minora measured 1cmin length and appeared grossly normal. The right labia minora measured 5 cm in length with thickened,darkly pigmented edgesconsistent with chronic irritation (Figure 2A, 2B). Observation versus surgical excision of the excess tissue was offered to the patient. After reviewing the risks of labioplasty,the patient desired surgical intervention.
Labioplasty was performed in the usual mannerunderspinal anesthesia with excellent results(Figure 2C). The patient tolerated the procedure well and was discharged the same day. Histological examination revealed labial tissue with chronic inflammation.
One month later the patient reported satisfaction with the cosmetic and hygienic results. Postoperatively, the labia appeared equal in size.
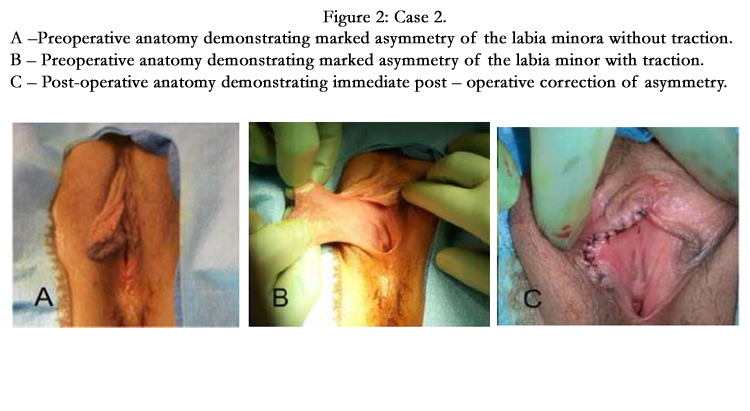
Figure 2. Case 2. A – Preoperative anatomy demonstrating marked asymmetry of the labia minora without traction.
B – Preoperative anatomy demonstrating marked asymmetry of the labia minor with traction.
C – Post-operative anatomy demonstrating immediate post – operative correctio asymmetry.
Discussion
Hypertrophy of the labia minora is defined as labia reaching greater than 4cm from the base of the labia [3,5]. Rouzier et al [3] described a series of 163 women undergoing labial reduction surgery for labial hypertrophy; with a range from 12-67 years of age. Pappis and Hadzihamberis [6] reported 5 girls, 18 months to 14 years old with bilateral labial hypertrophy. Jothilakshmi et al [4] evaluated the management of six adolescents, ages 11 to 16,that under went labial reduction. The patient in our first case represents the youngest reported surgical management of unilateral labial hypertrophy. Our second case demonstrates premenarchal development of unilateral hypertrophy with conservative management through menarche.
Current theories regarding the etiology of labial hypertrophy describe it as a normal variant in the adult; although some advocate that in the peripubertal patient this may represent an underlying hormonal disorder. However, Pappis and Hadzihamberis [6] revealed normal levels of serum estradiol and 24 hour urinary 17-ketosteroids in their evaluations.
Another theory of labial hypertrophy is chronic irritation or manipulation. It may be artificially created as a cultural preference with manual traction or manipulation of the labial skin [7]. Chronic irritation of the labia secondary to chronic urinary incontinence may also lead to chronic dermatitis [8].
Surgical excision of excess tissue is the definitive treatment to alleviate the symptoms associated with labial hypertrophy. Some suggest delayed surgery until completion of puberty since developmentally lagging labia majora may “catch up” to an initially enlarged labia minora [6]. Observation may be a less suitable in patients with progressively worsening symptoms, or as in our second case when the adolescent threatens self-mutilation.Our second patient demonstrated that delay until menarche does not alleviate the symptoms and may add additional discomfort related to adequate hygiene.Patients with labial hypertrophy that causes pain, limits hygiene, or affects the ability to void require more immediate treatment. Potential complications of early intervention include the need for repeat surgery for recurrence on the affected side or for contralateral hypertrophy [2]. Recurrence and contralateral occurrence representa rare event, as evidenced by Pappis and Hadzihamberis’series which had no recurrences at 5 year follow up [6].
The decision to postpone labioplasty until puberty should depend on the extent and severity of the patient’s symptoms. Pre-menarchal patients should be reassured about the typically benign nature of the condition, but that the condition will not resolve spontaneously. Discussion regarding management should include options of observation versus labioplasty,and the possibility of recurrence and contralateral occurrence.
References
- Maas SM, Hage JJ. (2000) Functional and aesthetic labia minora reduction. Plastic and reconstructive surgery 105(4): 1453-6.
- Lynch A, Marulaiah M, Samarakkody U. (2008) Reduction labioplasty in adolescents. Journal of pediatric and adolescent gynecology 21(3): 147-9.
- Rouzier R, Louis-Sylvestre C, Paniel BJ, Haddad B. (2000) Hypertrophy of labia minora: experience with 163 reductions. American journal of obstetrics and gynecology 182(1 Pt 1): 35-40.
- Jothilakshmi PK, Salvi NR, Hayden BE, Bose-Haider B. (2009) Labial reduction in adolescent population--a case series study. Journal of pediatric and adolescent gynecology 22(1): 53-5.
- Friedrich E. (1983) Vulvar Disease (2nd edtn). Philadelphia (PA).
- Pappis CH HP. (1987) Hypertrophy of the labia minora. Pedatr Surg Int 50-1.
- (WHO) WHO. Female genital mutilation. (2000) www.who.int/reproductivehealth/publications;.
- Kato K, Kondo A, Gotoh M, Tanaka J, Saitoh M, et al. (1988) Hypertrophy of labia minora in myelodysplastic women. Labioplasty to ease clean intermittent catheterization. Urology 31(4): 294-9.





