Changes in Glycosylation of Pituitary Gonadotropins in Polycystic Ovary Syndrome
Hernandez-Valencia M*, Hernández-Quijano T, Sandoval A, Miriam Ruiz Albarrán, Vargas-Giron A, Marion DH Rosas, Luis MB Sanchez, Renata Saucedo Gracía, Zárate A
Unit of Endocrine Diabetes and Metabolism Research, Specialties Hospital, National Medical Center, Instituto Mexicano del Seguro Social, Mexico city, Mexico.
*Corresponding Author
Dr. Marcelino Hernandez-Valencia M.D., PhD,
Unit of Endocrine Diabetes and Metabolism Research, Specialties Hospital,
National Medical Center, Instituto Mexicano del Seguro Social,
Mexico city, Mexico.
E-mail: mhernandezvalencia@prodigy.net.mx
Article Type: Case Report
Recieved: October 07, 2014; Accepted: November 05, 2014; Published: November 07, 2014
Citation: Hernández-Valencia M, et al., (2014) Changes in Glycosylation of Pituitary Gonadotropins in Polycystic Ovary Syndrome Int J ReprodFertil Sex Health, 1(4), 20-24. doi: dx.doi.org/10.19070/2377-1887-140004
Copyright: Hernández-Valencia M© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim: PCOS has endocrine and metabolic implications leading to a multicausal approach in pathogenesis. We assessed whether PCOS is conditioned by changes in glycosylation of pituitary gonadotropins.
Methods: Nested case-control cohort study. Gynecology/Obstetrics Hospital 3-A and Unit of Endocrine Research, Mexico City. Forty women in reproductive age were divided in two groups: patients who received treatment with no involution of the cyst and patients who received treatment but showed cyst regression. Hormone concentrations and glycosylation percentage of molecular isoforms of gonadotropins during opsomenorrhea and at 6 months of treatment were determined along with comparison of variables among groups using ANOVA.
Result(s): Molecular forms of FSH in women who persisted with ovarian cysts showed an increase in the firmly bound fraction, with forms of high glycosylation content (p <0.05). Determination of LH isoforms showed a lower percentage of weakly bound forms in women who persisted with ovarian cysts (p <0.05).
Conclusion(s): Minimal changes were observed in the distribution profile, which may be based on a process of hormonal dysregulation seen only in women who persisted with ovarian cysts. This indicated involvement of the isoforms of gonadotropins on functional changes in the ovary, allowing opportunity to establish new diagnostic criteria and intervention.
2.Introduction
3.Materials and Methods
3.1.Statistical Analysis
4.Results
5.Discussion
6.Acknowledgments
7.References
Keywords
Gonadotropins; Glycosylation; Polycystic Ovary Syndrome.
Introduction
The clinical features of polycystic ovary syndrome (PCOS) are comprised of obesity, hirsutism and amenorrhea, with the presence of pearly-appearing enlarged ovaries with multiple follicular cysts [1-2]. Both the initial description of this syndrome and the diagnosis have continuously evolved; therefore, the pathogenesis is a source of contradictions and theories [3-4]. These changes are due to the incorporation of continuous improvements in the methods and techniques of hormonal measurements as well as imaging methods, particularly vaginal ultrasound [5-7]. There is no consistent hormonal profile because the measurement of circulating hormones with the current analytical methods yields varying results, which in many cases are difficult to interpret [8-10].
PCOS has multiple endocrine and metabolic implications that have created a multicausal approach in its pathophysiology. Among the multiple causes is the reported central nervous system (CNS) involvement, with the control regulation center of gonadotropin-releasing hormone (GnRH), the pituitary with the gonadotrope and the portal system connected to the hypothalamus, the participation of the insulin resistance complex and hyperinsulinemia with consequent hyperandrogenism status, degree of obesity, the genetic component along the endocrine system and the involvement of adrenal glands with late-onset congenital adrenal hyperplasia [11-14]. Because we are dealing with gonadotropins in this study, it is important to note the regulatory links between the CNS and the ovaries with their estrogen hormone production [15,16]. Gonadotropins are synthesized and secreted by specialized cells called gonadotropes, which are found in the anterior pituitary and synthesize both FSH and LH [17,18]. It is known that the molecular forms of gonadotropins can vary in relation to hormonal status that predominates at each stage of life and typically correspond to changes in estrogen levels during physiological conditions such as puberty and the ovarian cycle, indicating that the FSH pleomorphism is a hormonally regulated phenomenon [19]. The clinical manifestation of this is that circulating FSH and LH have greater biological activity when they have incorporated a smaller amount of sialic acid. On the other hand, they have a longer half-life when they have incorporated a larger amount of sialic acid due to the protection offered to the molecule and thus have a prolonged biological effect. Thus, isoforms with less sialization are more potent than strongly sialized forms to induce proliferation of granulose cells and to prevent follicular atresia [20,21], this could have some participation in the formation of the ovarian cysts for regression lack due to a bigger sialization of the gonadotropins. The aim of this study was to assess whether the presence of ovarian cysts is related to changes in glycosylation of pituitary gonadotropins.
Materials and Methods
We included women of reproductive age (between 18 and 35 years) who were seen at the Obstetrics and Gynecology Hospital 3-A of the IMSS. We performed a nested case-control cohort study with a total of 40 patients. The case group was comprised of 20 patients who received combination therapy of chlormadinone at doses of 2 mg daily and metformin 850 mg at day [22,23] for a 6-month period, and there was no regression or disappearance of the cyst, with final resolution using the surgical approach for risk of torsion, pelvic pain or pelvic inflammatory disease. The other group consisted of 20 patients who also received the treatment regimen established in the first group but who showed regression of the ovarian cyst. A blood sample was taken from all patients to determine hormone levels and percentage of glycosylation of gonadotropins during the period of opsomenorrhea and again to the sixth cycles of treatment with PCOS. Transvaginal ultrasound was performed under established ultrasonographic criteria to determine the likelihood of benign ovarian cyst. This study was repeated every month to measure the speed of regression or growth or to stage size and characteristics of the cyst. In this manner, the data allowed for definition of satisfactory or unsatisfactory treatment response. When surgical intervention was necessary, preoperative examinations were performed along with surgical case review and cardiovascular and anesthesiology preoperative evaluation. All patients in this group were operated on by the same team from the gynecological endocrinology service. This was done in order to standardize laparoscopic excision procedure to reduce surgical damage and to obtain completely the cyst for intraoperative histopathological diagnosis to verify the nature of the cyst in each surgery, with subsequent follow-up care until resolution of their surgical procedure. All patients received a letter of informed consent explaining the motives for the study, its objectives, scope, benefits and risks, making resolution of the pathology a priority for medical treatment.
Hormonal blood determinations were carried out in the Unit of Endocrine Diabetes and Metabolism Research of the National Medical Center, Specialty Hospital in Mexico City. We used the technique previously described [24-26], using concanavalin-A (Con-A) in glass columns (0.6 x 15 cm) containing 2.5 ml of immobilized lectin gel (ConA conjugated to Sepharose 4B, Sigma, St. Louis, MO) equilibrated with Con-A buffer (Tris-HCl 50 mM, pH 7.4, containing NaCl 0.5 M, MgCl2 1 mM, CaCl2 1 mM, MnCl2 1 mM). Con-A allows separation of gonadotropin molecular forms into three fractions according to their degree of glycosylation:
1) forms that bind firmly to the lectin (FB),
2) forms that bind weakly to lectin (WB) and
3) molecular forms unbound to lectin (UB).
The elusions containing FB, WB and UB gonadotropin isoforms were concentrated using Centriprep membranes (Amicon, Beverly, MA). In each were determined FSH and LH concentrations by chemiluminescence assay using an automated system (Immulite, Diagnostic Products, Los Angeles, CA). The whole procedure was conducted at 4°C [27-28]. This method has a sensitivity of 0.7 mIU/mL for LH and 0.1 mIU/mL for FSH with an intra- and inter-assay coefficient of variation of 2.7 and 6.7% for LH, 2.8 and 3.7% for FSH, respectively.
Statistical Analysis
Simple frequencies and measures of central tendency and dispersion were used to describe the molecular isoforms of the gonadotropins. For between-group comparisons, two-way analysis of variance (ANOVA) was used, where way one represented the study group and way two represented changes in molecular isoforms. Data are expressed as mean±SD. Differences were considered statistically significant if p < 0.05.
Results
Characteristics of women enrolled at the moment of PCOS diagnosis, and at the end of the treatment are shown in (table 1) as responder and no-responders. The molecular isoforms of FSH determined at time of diagnosis of PCOS (basal) showed a distribution pattern described as normal in young women [29], with predominance of molecular forms UB to lectin by its low content of glycosylation with a decline in the rest of the glycoforms WB and FB. In women who persisted with ovarian cysts despite medical treatment, there was an increase in the FB fraction, with forms with a high content of glycosylation that showed a statistically significant difference (p <0.05) when compared with women who responded to the administered treatment. In these women, the distribution profile of glycoforms was observed to be similar to that obtained in the baseline measurement, albeit with different percentages of distribution. This may be interpreted as a lack of progression in abnormal changes in glycosylation of gonadotropins (Figure 1).
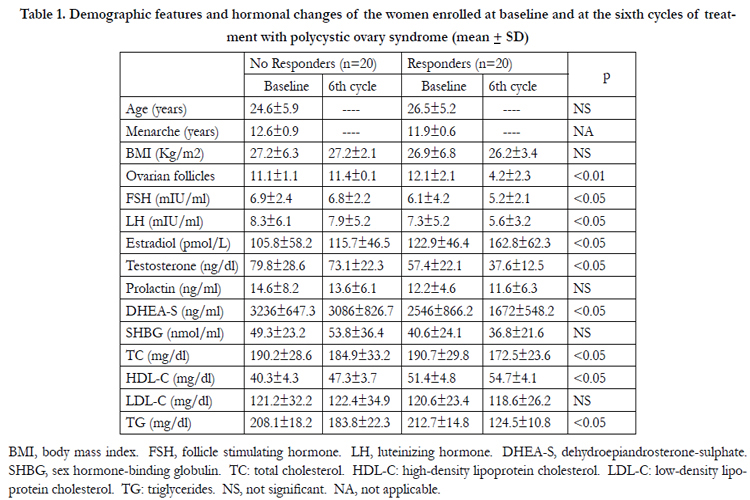

Table 1. Demographic features and hormonal changes of the women enrolled at baseline and at the sixth cycles of treatment with polycystic ovary syndrome (mean ± SD).
BMI, body mass index. FSH, follicle stimulating hormone. LH, luteinizing hormone. DHEA-S, dehydroepiandrosterone-sulphate. SHBG, sex hormone-binding globulin. TC: total cholesterol. HDL-C: high-density lipoprotein cholesterol. LDL-C: low-density lipoprotein cholesterol. TG: triglycerides. NS, not significant. NA, not applicable.
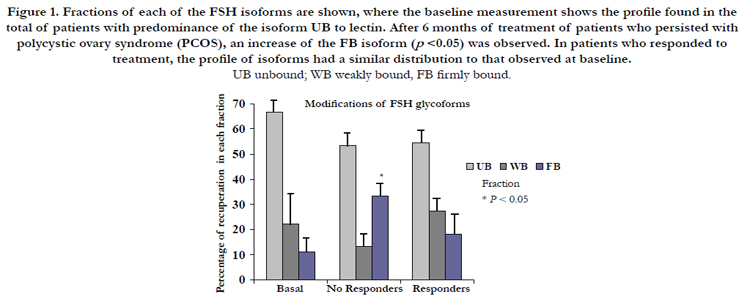
Figure 1. Fractions of each of the FSH isoforms are shown, where the baseline measurement shows the profile found in the total of patients with predominance of the isoform UB to lectin. After 6 months of treatment of patients who persisted with polycystic ovary syndrome (PCOS), an increase of the FB isoform (p <0.05) was observed. In patients who responded to treatment, the profile of isoforms had a similar distribution to that observed at baseline.
Baseline determination of LH showed an ascending distribution profile with a predominance of isoform FB bound to lectin, which is also considered as a normal distribution in women with regular menstrual cycles. When comparing the distribution of isoforms in women who persisted with ovarian cysts, there was a lower percentage observed of WB forms(p <0.05) , which have an intermediate amount of glycosylation. This was consequently reflected in an increase in the FB forms compared with baseline measurements and in women who responded to the administered treatment because both profiles show a similar distribution but with different isoforms percentages (Figure 2).
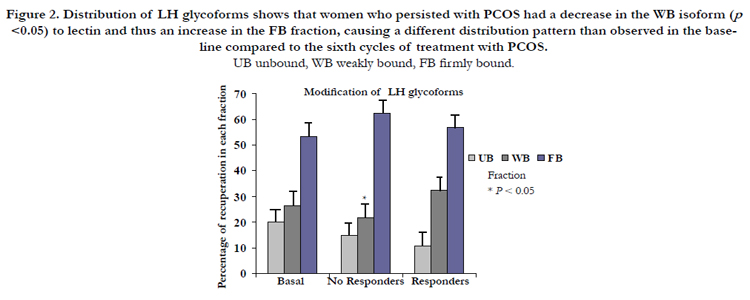
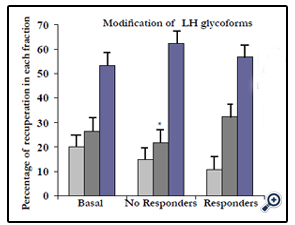
Figure 2. Distribution of LH glycoforms shows that women who persisted with PCOS had a decrease in the WB isoform (p <0.05) to lectin and thus an increase in the FB fraction, causing a different distribution pattern than observed in the baseline compared to the sixth cycles of treatment with PCOS.
Discussion
In the determination of both gonadotropins, minimal changes were observed in the distribution profile, which may be based on a process of hormonal dysregulation. It was seen only in women with persistence of ovarian cysts and may be interpreted as a lack of progress towards the changes in the distribution of glycoforms observed in women who responded to treatment.
These results provide the characteristics of a clinical profile associated with a hormonal profile in blood serum showing involve ment of the isoforms of gonadotropin on ovarian functional
changes. This affords the opportunity to establish new diagnostic criteria for intervention and medical hormonal management, including expectant management.
Knowledge of the degree of involvement of glycosylation allows us to provide additional insights into the pathophysiology of PCOS and useful results to initiate other lines of research on cell bioactivity and hormonal expression at the systemic level to provide insights into the inhibin-activin-follistatin way, leading to a better understanding of the causation of PCOS. It is well known that these qualitative changes are regulated by estrogen and oligosaccharides incorporated into the glycoprotein hormones, important to some unique aspects of hormonal function [30].
These are transcendent changes because granulose cells are target cells for FSH action and are only the type of cells expressing the FSH receptor. In the ovary, FSH regulates the function of granulose cells including development and selection of ovarian follicles, oocyte maturation and, together with LH, the ovulatory process [31,32]. Activation of protein receptors initiate a cascade of events that are amplified in each of the relay signals from the way of communication and culminate in a highly sensitive and specific cellular response [33]. In addition to steroid hormones, follicular fluid also contains a glycoprotein hormone, inhibin, which is produced by granulose cells. The effect of inhibin is the suppression of FSH but does not affect LH production. It is believed that thesuppression of other follicles is the result of inhibin produced by the active and dominant follicle. In this regard, inhibin may also be related with the process of follicular atresia. Increase in circulating estrogens 24 h prior to ovulation initiates the sudden increase in LH that causes ovulation. At 40 years of age, FSH levels begin to rise, even in women who ovulate regularly due to altered ovarian response or a decreased production of inhibin that inhibits FSH but not LH [33,34]. Aside from the inhibins, ovarian follicular fluid also contains substances called activins that can stimulate pituitary FSH secretion. In general, the actions of inhibin and activin are opposite to each other. The presence of a protein fraction that specifically suppresses pituitary FSH secretion, called follistatin, has also been noted, which probably depends on the degree of glycosylation of the polypeptide chain [35,36]. However, the mechanisms of action of activin and follistatin have not yet been well studied. Also, the ability of different isoforms of FSH to induce accumulation of cAMP in cultured mouse cumulus-oocyte-complexes has been evaluated, were the results demonstrate that FSH isoforms more acidic induced significant biological responses and that prolonged exposure caused attenuated signal transduction, what represents in the context of the pulsatile characteristics of FSH release from the pituitary and the half-life of less acidic isoforms possess important physiological functions during the periovulatory period [37]. Recently, has been described that in the ovaries of polycystic ovary syndrome patients, epimerase activity is enhanced, leading to a local myo-inositol deficiency which in turn is responsible for the poor oocyte quality, caused by the depletion of this FSH second messenger [38], settling down the resistance of the ovary to respond to FSH, that will eventually lead to the disbalance observed in our results. Using Sephadex-gel chromatography, gonadotropins of women with normal ovulatory cycles were analyzed, noting changes in the predominant molecular forms at different stages of the cycle. There is a heterogeneous distribution in women with anovulation, demonstrating the importance of the gonadotropins isoforms to trigger the cyclical ovulation process and therefore, maintain an ovulatory state [39].
Multiple therapeutic options for the treatment of ovarian cysts have been applied, but with little consistency in most cases. In addition, with this present pattern of glycoforms in our results we could have a parameter that indicates which patient with ovarian cyst, should have good answer to the treatment in terms of favorable prediction. In many of these women, total or partial resection of the ovary is carried out as a treatment of last resort. In order to reconcile the different views of the characteristics of PCOS, it has been proposed that the core components are the occurrence of an anovulatory state with a complex clinical features of hyperandrogenism. This establishes a broad construct and leaves obesity and morphological characteristics of the ovaries as simple nonspecific aggregates whose absence does not exclude this diagnosis [6,7]. Thus, the use of molecular biology has helped establish the characteristics of the interaction of FSH with its receptor. Therefore, identification of signal translation is important to extend it and apply it to the clinical area. It may enable the development and production of a variety of potentially useful analogues or antagonists to regulate exogenous gonadal function.
Acknowledgments
The important work in the laboratory determinations and monitoring of patients in the study by personnel from the Unit of Endocrine Research, as well as the participation of Mr. Jose Arturo Palacios and Ms. Lourdes Guevara Azato in the study is recognized. We also acknowledge the National System of Researchers (SNI) for the support given to the authors.
References
- Stein IF, Leventhal ML. (1935) Amenorrhea associated with bilateral polycystic ovaries.Am J Obstet Gynecol 29:181-191.
- Zárate A, Morán C, Hernández-Valencia M, Ochoa R. (2003) Stein-Leventhal syndrome, a metabolic-hormonal systemic dysfunction. Rev Med IMSS 41:165-174.
- Zrgher F, Ibañez L. (2009) Early origens of polycystic ovary syndrome: hypotheses may change without notice. J Clin Endocrinol Metab 94:3682-3685.
- Doret M, Raudrant D. (2001) Functional ovarian cysts and the need to remove them. Eur J Obstet Gynecol 100:1-4.
- Ehrmann DA. (2005) Polycystic ovary syndrome. N Engl J Med 352:1223- 1236.
- Belen AH, Laven JS, Tan SL. (2003) Ultrasound assessment of the polycystic ovary: international consensus definitions. Human Reproduction Update 9:505-514.
- Atiomo WU, Pearson S, Shaw S, Prentice A, Dubbins P. (2000) Ultrasound criteria in the diagnosis of polycystic ovary syndrome (PCOS). Ultrasound Med Biol 26:977-980.
- Pasquali R, Stener-Victorin E, Yildiz BO, Duleba AJ, Hoeger K, et al. (2011) PCOS Forum: research in polycystic ovary syndrome today and tomorrow. Clin Endocrinol 74:424-433.
- Rotterdam ESHRE/ASRM sponsored PCOS consensus workshop group. (2004) Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Human Reproduction 19:41-47.
- Azziz R, Woods KS, Reyna R, Key TJ, Knochenbaur ES, et al. (2004) The prevalence and features of the polycystic ovary syndrome in a unselected population. J Clin Endocrinol Metab 89:2745-2749.
- Kumar A, Woods KS, Bartolucci AA, Azziz R. (2005) Prevalence of adrenal androgen excess in patients with the polycystic ovary syndrome (PCOS).Clin Endocrinol 62:1-6.
- Winters SJ, Talbott E, Guzick DS, Zborowski J, McHugh KP. (2000) Serum testosterone levels decrease in middle age in women with the polycystic ovary syndrome. Fertility and Sterility 73:724-729.
- Stener-Victorin E, Holm G, Labrie F. (2010) Are there any sensitive and specific sex steroid markers for polycystic ovary syndrome?. J Clin Endocrinol Metab 95:810-819.
- Martínez-Onsurbe P, Ruiz VA, Sanz AJM, Valenzuela RPL. (2001) Aspiration cytology of 147 adnexal cysts with histologic correlation. Acta Cytol 45:941-947.
- Lansdown A, Rees DA. (2012) The sympathetic nervous system in polycystic ovary syndrome: a novel therapeutic target?. Clin Endocrinol 77:791-801.
- Crespigny LCH, Robinson HP, Davoren RAM, Fortune D. (1989) The simple ovarian cyst: aspirate or operate? Br J Obstet Gynaecol 96:1035-1039.
- Cappel SC, Ulloa-Aguirre A, Coutifaris C. (1983) Biosynthesis and secretion of follicle-stimulating hormone.Endocr Rev 4:179-184.
- Stanton PG, Burgon PG, Hearn MTW, Robertson DM. (1996) Structural and functional characterisation of FSH and LH isoforms. Mol Cell Endocrinol 125:133-141.
- Diamanti-Kandarakis E, Katsikis I, Piperi C. (2008) Increased serum advanced glycation end-products is a distinct finding in lean women with polycystic ovary syndrome (PCOS). Clinical Endocrinology 69:634-641.
- Dighe RR, Murthy GS, Kurkalli BS, Moudgal NR. (1990) Conformation of the alpha-subunit of glycoprotein hormones: a study using polyclonal and monoclonal antibodies. Mol Cell Endocrinol 72:63-70.
- Timossi C, Barrios-de-Tomasi J, Zambrano E, Ulloa-Aguirre A. (1998) A naturally occurring basically charged human follicle-stimulating hormone (FSH) variant inhibits FSH-induced androgen aromatization and tissue-type plasminogen activator enzyme activity in vitro. Neuroendocrinology 67:153-163.
- Zárate A, Hernández-Valencia M, Fonseca ME, Ochoa R. (1997) Metformine administration as therapy in young women with ovarian cystic syndrome. Ginecol Obstet Mex 65:504-507.
- Hoeger K, Davidson K, Kochman L. (2008) The impact of metformin, oral contraceptives, and lifestyle modifications on polycystic ovary syndrome in obese adolescent women in two randomized, placebo-controlled clinical trials. J Clin Endocrinol Metab 93:4299-4306.
- Allen HF, Mazzoni C, Heptulla RA. (2005) Randomized controlled trial evaluating response to metformin versus standard therapy in the treatment of adolescent with polycystic ovary syndrome. J Ped Endocrinol Metab 18:761-768.
- Creus S, Chaia Z, Pellizzari EH, Cigorraga SB, Ulloa-Aguirre A, et al. (2001) Human FSH isoforms: carbohydrate complexity as determinant of in-vitro bioactivity. Mol Cell Endocrinol 174:41–49.
- Ziping Y, Hancock WS. (2004) Approach to the comprehensive analysis of glycoproteins isolated from human serum using a multi-lectin affinity column. J Chromat A 1053:79-88.
- Papandreou MJ, Asteria C, Pettersson K, Ronin C, Beck-Peccoz P. (1993) Concanavalin A affinity chromatography of human serum gonadotropins: evidence for changes of carbohydrate structure in different clinical conditions. J Clin Endocrinol Metab 76:1008-1013.
- Baenziper JU, Green ED. (1988) Pituitary glycoprotein hormone oligosacharides: structure, synthesis and function of the asparagines-linked oligosaccharides on lutropin, follitropin and thyrotropin. Biochim Biophys Acta 947:287–306.
- Hernandez-Valencia M, Zarate A, Sandoval A, Miriam R, Timossi C, et al. (2007) Conjugated estrogens and tibolone modify the gonadotrophin glycosylation pattern in postmenopausal women. Gynecol Obstet Invest 63:22-27.
- Bousfield GR, Butnev VY, Gotschall RR. (1996) Structural features of mammalian gonadotropins. Mol Cell Endocrinol 125:3-19.
- Robertson DM, Foulds LM, Fry RCm Cummings JT, Clarke I. (1991) Circulating half-lives of follicle-stimulating hormone and luteinizing hormone in pituitary extracts and isoform fractions of ovariectomized and intact ewes. Endocrinology 129:1805-1813.
- Emmanouel DS, Stavropoulos T, Katz AI. (1984) Role of the kidney in metabolism of gonadotropins in rats. Am J Physiol 247:786- 792.
- Spanos WJ. (1973) Preoperative hormonal therapy of cystic adnexal masses. Am J Obstet Gynecol 116:551-556.
- McNeilly AS, Swanston IA, Crow W, Tsonis CG, Baird DT. (1989) Changes in the plasma concentrations of inhibin throughout the normal sheep oestrous cycle and after the infusion of FSH. J Endocrinol 120:295-298.
- Rivier C, Vale W. (1989) Immunoneutralization of endogenous inhibin modifies hormone secretion and ovulation in the rat. Endocrinology 125:152-157.
- Shimasaki S, Koga M, Buscaglia ML, Simons DM, Bicsak TA, et al. (1989) Follistatin gene expression in the ovary and extragonadal tissues suggests possible functions besides regulation of pituitary FSH secretion. Mol Endocrinol 3:651-654.
- Andersen CY, Leonardsen L, Ulloa-Aguirre A, Barrios-De-Tomasi J, Kristensen KS, et al. (2001) Effect of different FSH isoforms on cyclic-AMP production by mouse cumulus-oocyte-complexes: a time course study. Mol Hum Reprod 7:129-135.
- Carlomagno G, Unfer V, Roseff S. (2011) The D-chiro-inositol paradox in the ovary. Fertil Steril 95:2515-2516.
- Hernández-Valencia M, Mason M, Fonseca ME, Mendoza C, Ochoa R, et al. (1998) FSH and LH glycoform changes in women with ovarian failure treated with estrogens. Rev Med IMSS 36:435-439.





