Association Between Dietary Diversity and Lipid Indices among Kho-Kho Players Belonging to Different Regions of India
Kommi Kalpana1*, Gulshan Lal Khanna1, Akanksha Yadav2, Vatsala Saharan2, Renu Shresta2
1 Department of Sports, Faculty of Sports Manav Rachna International Institute of Research and Studies, Faridabad – 121004, Haryana, India.
2 Department of Nutrition and Dietetics, Faculty of Allied Health Sciences, Shree Guru Gobind Singh Tricentenary University, Gurgaon -122006, Haryana India.
*Corresponding Author
Prof. (Dr.) Kommi Kalpana,
Department of Sports, Faculty of Sports Manav Rachna International Institute of Research and Studies, Faridabad – 121004, Haryana, India.
Tel: +91-9701408969
E-mail: kommikalpana80@gmail.com
Received: July 07, 2022; Accepted: October 13, 2022; Published: October 25, 2022
Citation: Kommi Kalpana, Gulshan Lal Khanna, Akanksha Yadav, Vatsala Saharan, Renu Shresta. Association Between Dietary Diversity and Lipid Indices among Kho-Kho Players Belonging to Different Regions of India. Int J Food Sci Nutr Diet. 2022;11(6):634-641.
Copyright: Kommi Kalpana© 2022. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Dietary diversity is a proxy indicator of nutrient adequacy and has been propagated as a health beneficial component of dietary
behaviour. The present study was aimed to understand dietary diversity and its association with lipid indices among Kho-Kho
playersbelonging to Different Regions of India. Fifty Indian Kho-Kho players aged between 16-31yrs belonging to different
regions of India were recruited. Dietary diversity score (DDS; food groups/day) and food variety score (FVS; number of food
items/day) were considered to assess the dietary diversity (DD). The United Nations Food and Agricultural Organization
food frequency questionnaire was used as a tool. Serum total cholesterol (TC), triglycerides (TG), LDL, VLDL and HDL were
measured using an automatic clinical chemistry analyser following the standard protocols. The total DDS and FVS showed no
significant difference among players belonging to different regions of India, but individual food groups and number of variety
of green leafy vegetables, nuts and oilseeds, seafood and egg consumption showed a significant difference (p<0.01). LDL was
positively associated (p<0.01) with DDS. TG and VLDL were significantly positively associated with DDS of milk and milk
products (p<0.01), eggs (p<0.01) and FVS of spices and condiments (p<0.01) and inversely significantly associated with DDS
of meat (p<0.01) and nuts (p<0.01). An inversely significantly association was observed between DDS of vit-A rich vegetables
and LDL and also between DDS of roots and tubers and HDL.Dietary diversity was higher among athletes as compared to
non-athletes. Lipid indices other than LDL were not associated with DDS and FVS, but individual DDS were associated with
TG, VLDL, LDL and HDL.
2.Introduction
3.Materials and Methods
4.Results and Discussions
5.References
Keywords
Kho - Kho; Dietary Diversity; Lipid Indices; Indian Athletes.
Introduction
Kho-Kho is a popular traditional team sport in India, dating back
to prehistoric India. The origin of the sport is very difficult to
trace, but some of the empirical evidence shows that it is originated
from Maharashtra, India [1, 2]. In prehistoric India, it was
played on Indian chariots (raths), known as Rathera and emerged
in the modified form of ‘run-and-chase’ tag sport. In India, the
Kho-Kho competitions are held at the school, college and university
level apart from the national level. It is also played in South
Asia and South Africa [2]. Kho-Kho is a vigorous and combative
sport, requires the variables of agility, endurance, strength, power,
skills of dodging, feinting and bursts of speed at the individual
level to chase/pursue and touch the opponent [1].
An optimised sporting performance of athletes strongly relies
upon multiple factors such as physical, physiological, nutritional,
metabolic and cognitive factors [3]. Athletes, especially elite athletes
are encouraged to follow sound sports nutrition strategies
to meet the energy demands, macro and micronutrient requirements
and, maintain ideal body composition during training and
competition, reduce injury risk and optimize physical as well as
mental performance [3, 4]. Nutrient adequacy is one of the factors
that are crucial in maintaining the optimum level of health
and performance among athletes [3] for which, selection of foods
is important [4]. Designing nutritional interventions in order to
improve the nutrient adequacy of athletes requires an understanding
of the habitual dietary intake of athletes [5, 6].
Diverse diets have shown beneficial health effects, protecting
against chronic diseases such as diabetes,[7, 8] cardiovascular diseases,
[8-10] cancer [11] and longevity [12]. Dietary diversity can
be calculated by Dietary Diversity Scores (DDS) and Food Variety
Scores (FVS)[13]. DDS is based on food groups whereas FVS is
based on the number of food items consumed which are useful in
predicting nutrient adequacy [7]. The dietary diversity indicators
are very attractive as they are relatively simple and easy to measure
and reflects nutrient adequacy [14]. The perceived importance of
dietary diversity for health and nutrition has increased in the recent
past [15, 16]. To our knowledge, there are no studies available
on dietary diversity and its association with lipid indices in the athletic
population in Indian as well in the international setting. The
present study aimed to measure dietary diversity through DDS
and FVS and their association with lipid indices among Kho-Kho
Players belonging to different regions of India.
Materials And Methods
Participants
The cross sectional study includes fifty healthy male Indian Kho
- Kho players in the age group of 16-31 years undergoing training
in a national camp (Jan – Feb 2021) were recruited for the
study. Based on their domicile, the players were divided into four
groups; East, West, North and South regions. Kho-Kho players
from Indian states such as Bihar, Jharkhand, Odisha and West
Bengal and north east states were included in the East region;
Goa, Gujarat and Maharashtra were included in the West region;
Jammu & Kashmir, Himachal Pradesh, Punjab, Uttarakhand,
Haryana, Delhi, Rajasthan and Uttar Pradesh were included in the
North region; Andhra Pradesh, Karnataka, Kerala, Tamil Nadu,
and Telangana and the union territory Puducherry were included
in the South region. Information related socio-economic factors
and demographic characteristics were recorded in questionnaire
based interviews.The socio-demographic characteristics show
that a majority of the Kho-Kho players belonged to West region
(36%), followed by South (20%) and North (20%), East (14%),
Union territory (6%) and North East (4%).
Study Approval
The study was approved by the institutional ethical committee
and conducted according to the guidelines laid down in the declaration
of Helsinki [17]. The players were explained about the
study and the experimental protocol and their written consent
was obtained. The inclusion criteria was absence of any illness or
injury and exclusion criteria included intake of medication.
Dietary Diversity (DD)
Dietary diversity, which is a proxy indicator of nutrient adequacy
[18, 19] hasbeen propagated as a health beneficial component of
dietary behaviour [20]. Dietary diversity (DD) was defined as the
number of food groups consumed by an individual during the
dietary assessment period. In the present study, it was assessed
using dietary diversity score (DDS) and food variety score (FVS)
for a day. A structured questionnaire collapsed the food items into
17 food groups according to the United Nations Food and Agricultural
Organization (FAO) food group classification [13] was
used as a tool. Food groups considered were cereals & millets,
pulses, vitamin – A rich vegetables, white roots and tubers, green
leafy vegetables, other vegetables, milk and milk products, nuts
and oilseeds, fats and oils, other fruits, vitamin -A-rich fruits, egg,
seafood, organ meats, meat & poultry, sugars, spices and condiments.
Food items which are frequently consumed by the Indian
population were considered for adapted for the inclusion of food
items in each food group [21]. The questionnaire was administered
by a trained investigators through direct interview.
Dietary Diversity Score (DDS)
It was calculated by summing the number of food groups consumed
in 24 hours to calculate DDS. If an individual consumed
at least one food item from the food group was taken into count.
The minimum and maximum score points ranged from 0-17.
Food Variety Score (FVS)
Individual food items consumed from each food group was
counted to attain the FVS of the respective food group and then
the total FVS was counted summing up the food items consumed
from all the food groups. The maximum achievable FVS score
points were 154. While counting the scores, RTC/RTE foods
were excluded. To attain Food Variety Score (FVS), food items
consumed in 24 hours was counted.
Lipid Indices
Blood sample (5mL) was taken after 8-12 hours of overnight fasting
via vein puncture. Immediately the blood was transferred to a
vacutainer and serum was separated by centrifuging at 4000 rpm
for 10 min. The serum samples were stored at 180C till further
analysis. The test for lipid profile was performed within 72 hours
after obtaining the blood sample. The tests were performed using
an automatic clinical chemistry analyser, Erba (Lachema) XL200,
Germany.
Statistical Analysis
Statistical Package for Social Sciences (SPSS; IBM) version 27.0
was used for the analysis. Mean and Standard deviation were computed
for the DDS and FVS. Percentage was computed for food
choice and food behaviour, socio-economic and demographic
characteristics and commonly consumed foods. To know the difference
across different Indian regions for DDS and FVS, One
way analysis of variance along with Tukey post hoc test was done.
Linear regression was computed to find out the association lipid
indices and dietary diversity. The difference was considered at
p<0.05 and p<0.01.
Results and Discussion
The representation of players from West region states was higher
in the camp (Table 1). The origin of Kho-Kho from Maharashtra
(West India State), India [1] which would have influenced to
participate in the sport and to reach the national level. The prevalence
of non-vegetarianism (86%) was higher among Indian Kho-
Kho players. A similar observation was made by Khanna et al.
(2006) [22] in national Indian female athletes.
Dietary Diversity (DDS) and Food Variety Score (FVS)
The dietary diversity scores of Kho-Kho Players are given in Table
2. DDS showed that players were not consuming a few of the
food groups daily, but players were consuming satisfactory levels
of foods from various food groups as compared to the general
population [10, 21]. Consumption of foods from cereals and millets,
spices and condiments, fats and oils, sugars, other vegetables,
milk and milk products contributed greatly to DDS, but showed
no significant difference among the players belonging to different
regions. However, green leafy vegetables (GLV) (p<0.05), nuts
and oil seeds (p<0.01), egg (p<0.05) and sea foods (p<0.01) consumption
was significantly different across different regions. GLV
consumption was significantly higher (p<0.05) among North region
players followed by West, South, and East region players.
Nuts and oil seeds consumption was significantly higher (p<0.01)
among West region players followed by South, North and east
region players. Egg (p<0.05) and sea foods (p<0.01) consumption
was significantly higher among South region players followed
by West, East and North region players. The DDS showed no
significant difference between the players belonging to different
regions.There is a variation across Indian states in the availability
of a few of the foods especially leafy and other vegetables which
could be the reason for less consumption of foods [24] and some
of the foods were not consumed due to cultural and social beliefs
and food preferences.
The food variety scores of Kho-Kho Players are given in Table
3. The number of foods consumed from food groups such as
spices and condiments, GLV, other vegetables, fats and oils and
other fruits consumption greatly contributed to FVS, but showed
no significant difference among the players belonging to different
regions other than GLV. The consumption of number of foods
from green leafy vegetables (p<0.05), nuts and oil seeds (p<0.01),
egg (p<0.05) and sea foods (p<0.01) was significantly different
across different regions. Consumption of number of GLV was
higher among South region players and also found a significant
difference between than East and North region players. Nuts and
oil seeds consumption was significantly higher (p<0.01) among
West region players than South, North and East region players
and also found a significant difference between East and South
and North region players. Egg (p<0.05) and sea foods (p<0.01)
consumption was significantly higher among South region players
than West, East and North region players and consumption was
not reported by North region players.
The players consumed a variety of foods on a daily basis. Participation
in sports and the recognized importance of diet on sports
performance would have played a role in the consumption of a
wide variety of foods [23]. Dietary diversity and food variety fluctuate
across various seasons. In winter, household food basket is
more diverse and food variety and dietary diversity increase due
to food choices in winter [24], would have influenced higher DD
among players of the study.
Status of Lipid Indices
Regarding the lipid levels, lower HDL (15.3%) levels and higher
serum TC (10.4%), TG (28%), LDL (22%), and VLDL (15.4%)
levels were observed among the players (Fig.1). The majority of
players were having normal lipid profile. Higher dietary diversity
was associated with a lower risk of abnormal levels of blood lipids
[25].
Association of Dietary Diversity with Lipid Indices
The regression analysis showed that total DDS and FVS showed
no association with lipid indices other than LDL(p<0.01)(Table
4).However, serum triglycerides and VLDL were significantly associated
with DDS of milk items (p<0.01), egg (p<0.01), and FVS
of spices (p<0.01).Unfortunately, there is no supporting/ deferring
evidence in this direction on the athletic population. Milk and
milk products have a hypercholesteraemic effect due to saturated
fatty acid content,[26] larger quantities of milk and milk products
may be avoided on a daily basis. The study showed a positive association of daily egg consumption with TG and VLDL. Empirical
evidence suggests that consumption of two eggs/day for 12
weeks would change the apolipoproteins and would not adversely
affect the blood lipids in trained women [27]. The information
on the number of eggs consumption/day would have provided a
better understanding of its effect on lipid indices.
The health benefits of Indian spices have been reported [40, 41],
but in the present study the intake of spices and condiments were
significantly associated with TG and VLDL. Spicy food was positively
associated with serum TAG [42, 43]. High energy and fat
intake act as mediators along with spicy food in increasing the
risk of abdominal obesity [44]. We also assume that the players
consuming high energy and fat diets could have mediated an increase
in TG and VLDL. Additional studies on mechanisms that
are involved in the potential role of spicy food consumption in
lipid metabolism may support the findings.
In the present study, TG and VLDL were inversely associated
(p<0.01) with DDS of meat. Meat is rich in protein, lipoic acids,
creatinine, zinc, iron and B-vitamins etc, the scientific evidence
suggests reducing consumption of meat and meat products due
to high saturated fat content and its link with chronic diseases
[28-31]. But, Protein, Lipoic acid, creatinine, vitamins and minerals
are beneficial for active trained men [32, 33] and would have
influenced a decrease in TG and VLDL.
The players showed a significantly inversely association (p<0.01)
with DDS of nuts with TG and VLDL. Nuts have high levels of
unsaturated fatty acids and bioactive compounds (minerals, polyphenols,
Phyto esters, fibre) may improve cardiometabolic health,
endothelial function, improved glycemic control, lower blood
pressure and body weight [34]. Nuts lower the serum cholesterol
levels by lowering the absorption of cholesterol, inhibiting HMGCoA
reductase and increasing bile acid production by stimulation
of 7-α hydroxylase [35]. Consumption of >5g/day to < 25g/day
of nuts showed a positive association in reducing the cardiovascular
disease risk in the untrained population [36].
DDS of other vegetables were inversely associated (p<0.01) with
LDL and FVS of roots and tubers was inversely associated with
HDL. Intake of whole grains, vegetables and fruits would provide
adequate intake of vitamins, minerals and antioxidants, beneficial
for reducing CVD risk factors [37, 38], increase skin carotenoids
and reduce body fat in athletes [39]. Increasing the dietary diversity
score with a wide variety of seasonal vegetables and fruits
and controlling the energy intake as per the requirement may be
beneficial for improving blood lipid indices.
Food Choices and Behaviour of Kho-Kho Players
Food choice is influenced by various factors physiological, psychological,
social and economic factors and also varies within
and between individuals and populations [23]. Foods choices and
food behaviour of players showed that 44% of the players consumed
other than home foods once or twice a week, and the top
consumed foods were chicken items (48%), followed by Samosa
(18%) (Indian savory), Indian sweets (16%), Noodles(16%), Mutton
items(16%), Fish items(14%), Ice cream (12%), Biryani (12%)
and Momo’s (10%). There is a strong link between food availability
and food choice [45]. The commonly consumed foods in
the present study represent the factors related to the availability
of foods, cost, taste and social and cultural beliefs in making food
choices (Table 5).
Athletes have nutrition knowledge for healthy food choices [46]
and are aware of consuming foods before, during and after exercise
[47]. A majority of players (82 %)reported that they consume
foods before an exercise program,but 60.8%playersreported that
they do not follow the timings. 52% of the players consume foods
during exercise and the top reported foods were liquid foods such
as water, glucose water, lemon water, fruit juice, tea, energy drink,
whey protein. 62% of the players consume immediately after exercise
program and the reported foods were banana, Bengal gram
whole, milk, biscuits, bread, apple, egg, soya bean, protein shake,
jaggery, upma (an Indian Breakfast recipe). The most disliked
foods were bitter gourd, brinjal, pumpkin, capsicum, ladies finger
and beef (table.5). Athletes have nutrition knowledge for healthy
food choices [46] and are aware of consuming foods before, during
and after exercise [47]. The players may adopt appropriate
sport nutrition strategies that meet the sporting demands before,
during and after exercise and may value convenient foods that are
easy to carry to the training areas. Nutrition education sessions
may be provided to players to make significant food behavioural
changes [48]. DD may be an useful tool to assess and monitor the
food behaviour of players.
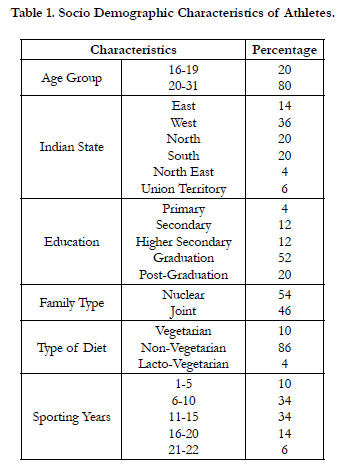

Table 1. Socio Demographic Characteristics of Athletes.
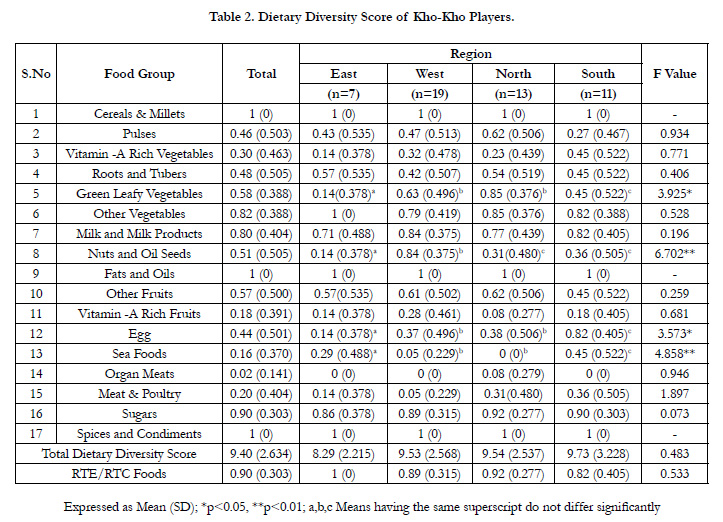
Table 2. Dietary Diversity Score of Kho-Kho Players.
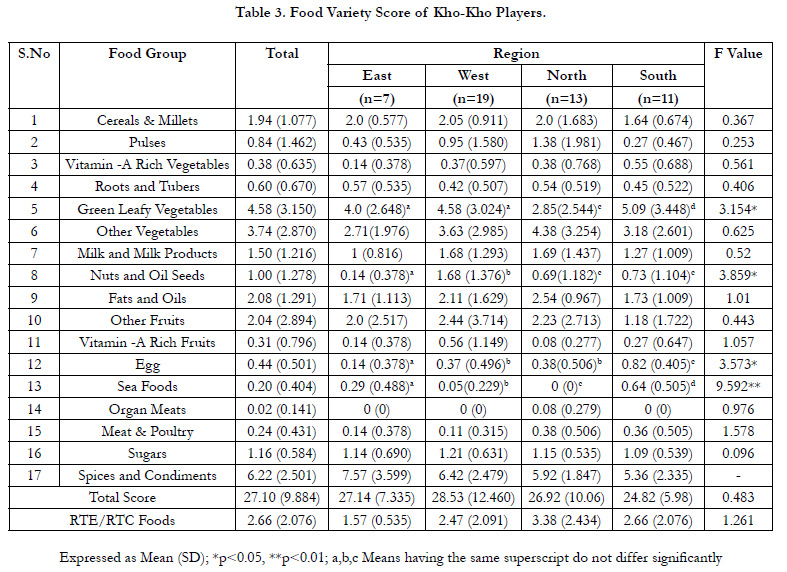
Table 3. Food Variety Score of Kho-Kho Players.
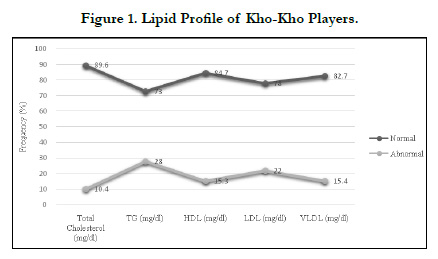
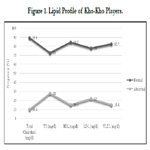
Figure 1. Lipid Profile of Kho-Kho Players.
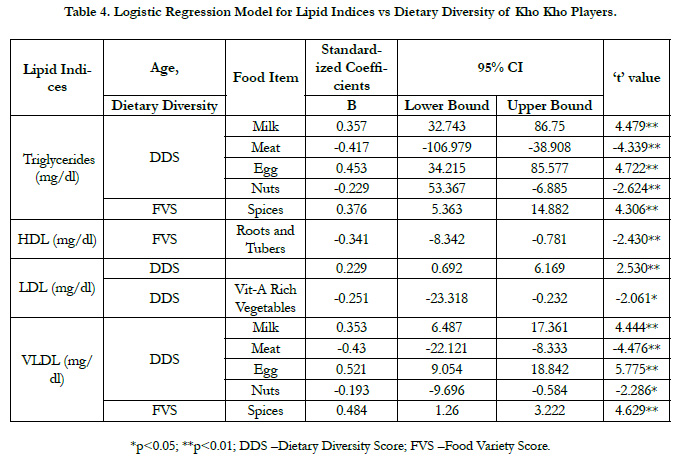
Table 4. Logistic Regression Model for Lipid Indices vs Dietary Diversity of Kho Kho Players.
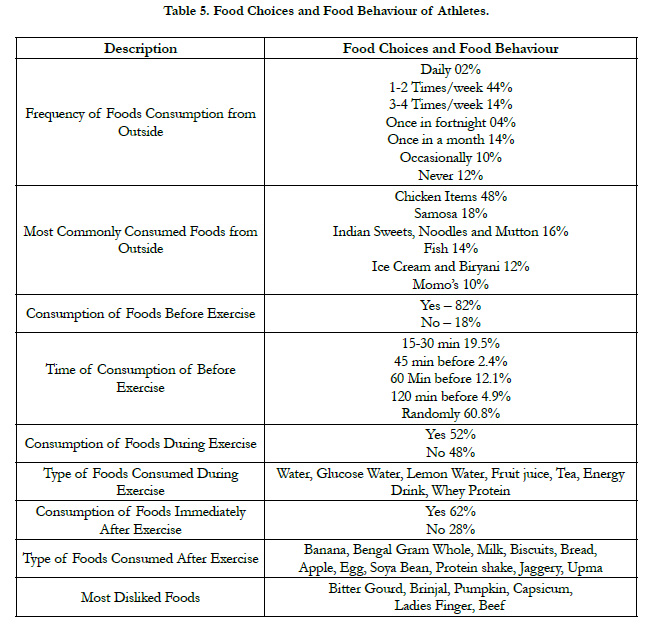
Table 5. Food Choices and Food Behaviour of Athletes.
Table 2. Prescribed and non-prescribed MSG values on labels of different examined chicken meat products(n=10 of each)./strong>
Limitations
The study represents a smaller sample, involving players with differing
physiological requirements (adolescents and adults). Selfreported
dietary intake is prone to recall bias, mis or underreporting
[5, 49, 50]. Quantitative intake of foods and information
on dietary supplements were not recorded. Availability of athletic
specific and country specific diet quality index would have been
a better tool to evaluate dietary diversity and its role on various
biomarkers of players.
Conclusion
Dietary diversity was higher among Kho-Kho players with consumption
of more than nine food groups and more than twenty
seven variety of foods on a daily basis. Lipid indices other than
LDL were not associated with DDS and FVS, but individual DDS
were associated with TG, VLDL, LDL and HDL.TG and VLDL
may decrease with consumption less quantities of whole milk and
milk products, eggs and with daily consumption of meat and nuts.
LDL may decrease with consumption of vitamin- A rich vegetables
and HDL may increase with less intake of roots and tubers.
High energy and fat foods may act as mediators along with spices
intake in increasing TG, and VLDL.
Acknowledgement
The authors would like to thank Kho Kho Federation of India
and SGT University for the support. We would like to thank Dr.
Keren Susan Cherian, National Sports University, Manipur for
her inputs in draft preparation and Dr. Archana Konapur ICMRNIN,
Hyderabad for providing necessary support in finalizing the
manuscript.
Author Contributions
Conceptualization: KK, GLK; Data Curation: AY, RS, VS and
Formal Analysis: KK; Funding Acquisition: GLK; Investigation,
Methodology: KK, GLK; Project Administration, Supervision:
GLK; Manuscript writing: KK; Review of Manuscript: KK, GLK
Funding information
Financial support was received from Kho Kho Federation of India
(KKFI).
Ethical Approval
This study was approved by theInstitutional Ethical Committee
of Shri Guru Gobind Singh Tricentenary (SGT) University, Gurgaon,
Haryana, India.
References
- PeterAH. Student-Designed Games: Strategies for Promoting Creativity, Cooperation, and Skill Development. Human Kinetics; 2010.
- Jaiswal J. Anthropometric and somatotyping study among the female Kho- Kho players of Pondicherry: A comparative analysis. JGlobal Eco. 2014;2:1- 3.
- Thomas DT, Erdman KA, Burke LM. Nutrition and athletic performance. Med Sci Sports Exerc. 2016 Mar;48:543-68.
- Maughan RJ, Shirreffs SM. Nutrition for sports performance: issues and opportunities. Proc Nutr Soc. 2012 Feb;71(1):112-9. PubMed PMID: 22000743.
- Capling L, Beck KL, Gifford JA, Slater G, Flood VM, O'Connor H. Validity of Dietary Assessment in Athletes: A Systematic Review. Nutrients. 2017 Dec 2;9(12):1313. PubMed PMID: 29207495.
- Beck KL, von Hurst PR, O'Brien WJ, Badenhorst CE. Micronutrients and athletic performance: A review. Food ChemToxicol. 2021 Dec;158:112618. PubMed PMID: 34662692.
- Danquah I, Galbete C, Meeks K, Nicolaou M, Klipstein-Grobusch K, Addo J, et al. Food variety, dietary diversity, and type 2 diabetes in a multi-center cross-sectional study among Ghanaian migrants in Europe and their compatriots in Ghana: the RODAM study. Eur J Nutr. 2018 Dec;57(8):2723- 2733. PubMed PMID: 28948398.
- Kapoor D, Iqbal R, Singh K, Jaacks LM, Shivashankar R, Sudha V, et al. Association of dietary patterns and dietary diversity with cardiometabolic disease risk factors among adults in South Asia: The CARRS study. Asia Pac J ClinNutr. 2018;27(6):1332-1343. PubMed PMID: 30485933.
- Farhangi MA, Jahangiry L. Dietary diversity score is associated with cardiovascular risk factors and serum adiponectin concentrations in patients with metabolic syndrome. BMC CardiovascDisord. 2018 Apr 17;18(1):68. PubMed PMID: 29665770.
- Azadbakht L, Mirmiran P, Esmaillzadeh A, Azizi F. Dietary diversity score and cardiovascular risk factors in Tehranian adults. Public Health Nutr. 2006 Sep;9(6):728-36. PubMed PMID: 16925878.
- Mirjalili F, Rezazadegan M, Jalilpiran Y, Mousavi SM, Jafari A, Mohajeri SAR, et al. The Association between Dietary Diversity Score and Risk of Prostate Cancer: (A Case-Control Study). Nutr Cancer. 2022;74(4):1270- 1278. PubMed PMID: 34278902.
- . Miyamoto K, Kawase F, Imai T, Sezaki A, Shimokata H. Dietary diversity and healthy life expectancy-an international comparative study. Eur J Clin- Nutr. 2019 Mar;73(3):395-400. PubMed PMID: 30104730.
- Kennedy G, Ballard T, Dop MC. Guidelines for measuring household and individual dietary diversity. Food and Agriculture Organization of the United Nations; 2011.
- Hussien FM, Mebratu W, Ahmed AY, Mekonnen TC, Hassen AM, Asfaw ZA, et al. Performance of individual dietary diversity score to identify malnutrition among patients living with HIV in Ethiopia. Sci Rep. 2021 Sep 21;11(1):18681. PubMed PMID: 34548547.
- Ganpule-Rao AV, Bhat D, Yajnik CS, Rush E. Dietary diversity scores, nutrient intakes and biomarkers vitamin B12, folate and Hb in rural youth from the Pune Maternal Nutrition Study. Br J Nutr. 2021 Jul 28;126(2):236-243. PubMed PMID: 33046143.
- Agrawal S, Kim R, Gausman J, Sharma S, Sankar R, Joe W, et al. Socio-economic patterning of food consumption and dietary diversity among Indian children: evidence from NFHS-4. Eur J ClinNutr. 2019 Oct;73(10):1361- 1372. PubMed PMID: 30809007.
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013 Nov 27;310(20):2191-4. PubMed PMID: 24141714.
- Rathnayake KM, Madushani P, Silva K. Use of dietary diversity score as a proxy indicator of nutrient adequacy of rural elderly people in Sri Lanka. BMC Res Notes. 2012 Aug 29;5:469. PubMed PMID: 22931957.
- Abizari AR, Azupogo F, Nagasu M, Creemers N, Brouwer ID. Seasonality affects dietary diversity of school-age children in northern Ghana. PLoS One. 2017 Aug 14;12(8):e0183206. PubMed PMID: 28806418.
- Mirmiran P, Azadbakht L, Esmaillzadeh A, Azizi F. Dietary diversity score in adolescents - a good indicator of the nutritional adequacy of diets: Tehran lipid and glucose study. Asia Pac J ClinNutr. 2004;13(1):56-60. PubMed PMID: 15003915.
- Jose SS, Shalini T, Balakrishna N, Radhika MS, Brahmam GN, Reddy GB. A raw food based quantitative food frequency questionnaire to assess longterm dietary-intake among urban adults of South India: Relative Validity and Reproducibility. Indian J NutrDiet. 2018 Jan;55(1):1.
- Khanna GL, Lal PR, Kommi K, Chakraborty T. A comparison of a vegetarian and non-vegetarian diet in Indian female athletes in relation to exercise performance. JExerSciPhy. 2006 Jan;2:27-34.
- Birkenhead KL, Slater G. A Review of Factors Influencing Athletes' Food Choices. Sports Med. 2015 Nov;45(11):1511-22. PubMed PMID: 26243016.
- Hussain A, Zulfiqar F, Saboor A. Changing food patterns across the seasons in rural Pakistan: analysis of food variety, dietary diversity and calorie intake. Ecol Food Nutr. 2014;53(2):119-41. PubMed PMID: 24564189.
- Guo Q, Ma Z, Zhu C, Zeng Q. Dietary diversity and physical activity associations with lipid indices among Beijingese: A cross-sectional study. Asia Pac J ClinNutr. 2020;29(3):628-637. PubMed PMID: 32990624.
- Chi D, Nakano M, Yamamoto K. Milk and milk products consumption in relationship to serum lipid levels: a community-based study of middle- aged and older population in Japan. Cent Eur J Public Health. 2004 Jun;12(2):84-7. PubMed PMID: 15242025.
- Wilson T, Clark L, Dellogono M. Consumption of Two Eggs Daily Increases Serum Leptin in Amenorrheic Runners With Low Energy Availability Without Changes in Lipid Profile. CurrDevNutr. 2021 Jun;5(Supplement_2):1298.
- Pan A, Sun Q, Bernstein AM, Manson JE, Willett WC, Hu FB. Changes in red meat consumption and subsequent risk of type 2 diabetes mellitus: three cohorts of US men and women. JAMA Intern Med. 2013 Jul 22;173(14):1328-35. PubMed PMID: 23779232.
- Micha R, Wallace SK, Mozaffarian D. Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: a systematic review and meta-analysis. Circulation. 2010 Jun 1;121(21):2271-83. PubMed PMID: 20479151.
- Wu J, Zeng R, Huang J, Li X, Zhang J, Ho JC, et al. Dietary Protein Sources and Incidence of Breast Cancer: A Dose-Response Meta-Analysis of Prospective Studies. Nutrients. 2016 Nov 17;8(11):730. PubMed PMID: 27869663.
- Guasch-Ferré M, Satija A, Blondin SA, Janiszewski M, Emlen E, O'Connor LE, et al. Meta-Analysis of Randomized Controlled Trials of Red Meat Consumption in Comparison With Various Comparison Diets on Cardiovascular Risk Factors. Circulation. 2019 Apr 9;139(15):1828-1845. PubMed PMID: 30958719.
- Isenmann E, Trittel L, Diel P. The effects of alpha lipoic acid on muscle strength recovery after a single and a short-term chronic supplementation - a study in healthy well-trained individuals after intensive resistance and endurance training. J IntSoc Sports Nutr. 2020 Dec 1;17(1):61. PubMed PMID: 33261642.
- Hall M, Manetta E, Tupper K. Creatine Supplementation: An Update. Curr Sports Med Rep. 2021 Jul 1;20(7):338-344. PubMed PMID: 34234088.
- Kim Y, Keogh J, Clifton PM. Nuts and Cardio-Metabolic Disease: A Review of Meta-Analyses. Nutrients. 2018 Dec 6;10(12):1935. PubMed PMID: 30563231.
- Kim Y, Keogh JB, Clifton PM. Benefits of Nut Consumption on Insulin Resistance and Cardiovascular Risk Factors: Multiple Potential Mechanisms of Actions. Nutrients. 2017 Nov 22;9(11):1271. PubMed PMID: 29165404.
- Becerra-Tomás N, Paz-Graniel I, WC Kendall C, Kahleova H, Rahelić D, Sievenpiper JL, et al. Nut consumption and incidence of cardiovascular diseases and cardiovascular disease mortality: a meta-analysis of prospective cohort studies. Nutr Rev. 2019 Oct 1;77(10):691-709. PubMed PMID: 31361320.
- Joaquim DP, Juzwiak CR, Winckler C. Diet Quality Profile of Trackand- Field Paralympic Athletes. Int J Sport NutrExercMetab. 2019 Nov 1;29(6):589-595. PubMed PMID: 31034250.
- Mellendick K, Shanahan L, Wideman L, Calkins S, Keane S, Lovelady C. Diets Rich in Fruits and Vegetables Are Associated with Lower Cardiovascular Disease Risk in Adolescents. Nutrients. 2018 Jan 27;10(2):136. PubMed PMID: 29382069.
- Jontony N, Hill EB, Taylor CA, Boucher LC, O'Brien V, Weiss R, et al. Diet Quality, Carotenoid Status, and Body Composition in NCAA Division I Athletes. Am J Health Behav. 2020 Jul 1;44(4):432-443. PubMed PMID: 32553025.
- Ferrucci LM, Daniel CR, Kapur K, Chadha P, Shetty H, Graubard BI, et al. Measurement of spices and seasonings in India: opportunities for cancer epidemiology and prevention. Asian Pac J Cancer Prev. 2010;11(6):1621-9. PubMed PMID: 21338207.
- Kumar V. Seven spices of India—from kitchen to clinic. J Ethnic Foods. 2020 Dec;7:23.
- Xue Y, He T, Yu K, Zhao A, Zheng W, Zhang Y, et al. Association between spicy food consumption and lipid profiles in adults: a nationwide population- based study. Br J Nutr. 2017 Jul;118(2):144-153. PubMed PMID: 28673367.
- Dong X, Li Y, Yang K, Zhang L, Xue Y, Yu S, et al. Associations of spicy food flavour and intake frequency with blood lipid levels and risk of abnormal serum lipid levels in Chinese rural population: a cross-sectional study. Public Health Nutr. 2021 Dec;24(18):6201-6210. PubMed PMID: 33913411.
- Yang K, Li Y, Xue Y, Wang L, Liu X, Tu R, et al. Association of the frequency of spicy food intake and the risk of abdominal obesity in rural Chinese adults: a cross-sectional study. BMJ Open. 2019 Nov 10;9(11):e028736. PubMed PMID: 31712332.
- Mello JA, Gans KM, Risica PM, Kirtania U, Strolla LO, Fournier L. How is food insecurity associated with dietary behaviors? An analysis with lowincome, ethnically diverse participants in a nutrition intervention study. J Am Diet Assoc. 2010 Dec;110(12):1906-11. PubMed PMID: 21111099.
- Eck KM, Byrd-Bredbenner C. Food Choice Decisions of Collegiate Division I Athletes: A Qualitative Exploratory Study. Nutrients. 2021 Jul 6;13(7):2322. PubMed PMID: 34371832.
- Cherian KS, Gavaravarapu SM, Sainoji A, Yagnambhatt VR. Coaches' perceptions about food, appetite, and nutrition of adolescent Indian athletes - A qualitative study. Heliyon. 2020 Feb 7;6(2):e03354. PubMed PMID: 32072052.
- KaurR, KaurN, KaurA. Influence of sports dietitianon the dietary intake and hydration habits of collegiate athletes.CurrJApplSciTech. 2021;61-75.
- Magkos F, Yannakoulia M. Methodology of dietary assessment in athletes: concepts and pitfalls. CurrOpinClinNutrMetab Care. 2003 Sep;6(5):539- 49. PubMed PMID: 12913671.
- Ferraris C, Guglielmetti M, Trentani C, Tagliabue A. Assessment of Dietary Under-Reporting in Italian College Team Sport Athletes. Nutrients. 2019 Jun 21;11(6):1391. PubMed PMID: 31234276.





