Prevalence of Diabetes and Pre-Diabetes in a Cohort of High Risk Undiagnosed Patients
Mortada D1, Wehbe T2*, Abou Jaoude E3
1 Faculty of Agricultural Sciences, The Holy Spirit University, Kaslik, Jounieh, Lebanon.
2 Department of Hematology, The Lebanese Canadian and Notre Dame University Hospitals, Jounieh, Lebanon.
3 Department of Endocrinology, Middle East Institute, Bsalim, Lebanon.
*Corresponding Author
Wehbe Tarek, M.D,
Department of Hematology, The Lebanese Canadian and Notre Dame University Hospitals, Jounieh, Lebanon.
E-mail: twwehbe4@gmail.com
Received: January 04, 2018; Accepted: January 22, 2018; Published: January 29, 2018
Citation: Mortada D, Wehbe T, Abou Jaoude E. Prevalence of Diabetes and Pre-diabetes in a Cohort of High Risk Undiagnosed Patients. Int J Food Sci Nutr Diet. 2018;7(1):372-376. doi: http://dx.doi.org/10.19070/2326-3350-1800066
Copyright: Wehbe T© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Type 2 diabetes (T2D) is a silent disease that progresses sometimes for years before diagnosis. Several methods of screening of diabetes have been suggested. Screening those at high risk periodically may be the most cost effective. Our primary objective is to evaluate the usefulness of a simple questionnaire in evaluating undiagnosed subjects at risk, in order to determine the prevalence of pre-diabetes (PD) and T2D in high risk patients.
A group of 200 Lebanese subjects were randomly selected from different areas of Bekaa, aged 18 to 65 years, not diagnosed with pre-PD or T2D. A questionnaire was used to assess gender, history of gestational diabetes, family history of diabetes, presence of hypertension, level of physical activity and anthropometry. Participants who had a total score greater than or equal to five were selected for laboratory tests for diabetes.
The prevalence of PD and T2D was 8.5% and 26% respectively. 34.5% in total. A significant positive correlation was found between diabetes risk factors and the risk of developing the disease. Indicators were age (p<0.001), history of gestational diabetes (p = 0.004), family history of diabetes (p<0.001), presence of hypertension (p< 0.001), physical inactivity (p<0.001) and overweight/obesity state (p=0.001).
In Conclusion, using a simple practical tool consisting of a questionnaire is highly effective in uncovering undiagnosed T2D and PD. Early detection of PD and T2D is associated with tremendous health benefits including prevention of the irreversible diabetic complications and their dreaded quality-of-life altering effects.
2.Introduction
3.Material and Methods
4.Statistical Analysis
5.Results
6.Discussion
7.Conclusion
8.References
Keywords
Pre-Diabetes; Type 2 Diabetes; Diabetes Risk Factors.
Introduction
Type 2 diabetes is a state of hyperglycemia due to dysfunction of the pancreatic beta cells. It is a chronic silent disease that progresses over years. According to the International Diabetes Federation, the prevalence of diabetes is increasing worldwide. Metabolic deregulation associated with T2D causes a series of complications including micro- and macro-angiopathic anomalies [1-4].
No specific data and statistics are available in Lebanon, to estimate the prevalence of T2D and PD in rural areas such as Bekaa. Therefore, we undertook the mission of conducting this cross sectional study of 200 individuals aged 18 to 65, randomly selected from different regions of the Bekaa.
The objectives of our study were to determine the prevalence of T2D and PD in high-risk patients, not known diabetics, and correlate the incidence with the known risk factors and their effects on developing T2D and PD. The risk factors studied were age, hypertension, obesity, family history of diabetes, history of gestational diabetes, and sedentary lifestyle [5-7].
Material and Methods
A cross-sectional study was conducted to determine the prevalence of PD and T2D in high-risk patients in the Bekaa region. The design of the study was approved by the Ethics Committee of the Department of Human Nutrition and Dietetics of the Faculty of Agricultural and Food Sciences - The Holy Spirit University, Lebanon.
A group of 200 Lebanese individuals were randomly selected for the study. Individuals aged 18 to 65 were selected from different areas of Bekaa. A diabetes risk test, in the form of a questionnaire, was conducted including age, gender, history of gestational diabetes, family history of diabetes, presence of hypertension, level of physical activity and anthropometry. Participants with a total score greater than or equal to five were selected for laboratory tests to establish the diagnosis of diabetes or pre-diabetes. Subjects were excluded if they had known PD or T2D, or if they were Women with gestational diabetes at the time of the study.
Participants were considered to have PD if they had a glycated hemoglobin (HbA1C) level between 5.7 and 6.4% and/or a fasting blood glucose level between 100 and 125 mg/dL. While those diagnosed with T2D, had to have HbA1c ≥ 6.5% and/or fasting blood glucose ≥126 mg/dL. The weight and height were measured by a dietician, using a digital scale and a height scale respectively.
Statistical Analysis
Data capture and statistical analysis were performed using the Statistical Package for Social Science (SPSS) version 20.0. The confidence interval (CI) was set at 95% and a value of p <0.05 was considered significant. Continuous quantitative variables were described as mean and standard deviation and qualitative variables as numbers and percentages. A bi-variate analysis was conducted. The Chi-square test (χ2) was used to study the relationship between qualitative variables. This test was replaced by Fisher's exact test if in one of the boxes of the table; expected numbers were less than five. Student's t-test was used to compare two means. The medians between three groups were compared using the Kruskal-Wallis test because the condition of normality was not satisfied.
Results
The characteristics of the study population are summarized in Table 1. Ninety five were aged below 40 years of age, 37 participants were 40-49 years old, 45 participants were between 50 and 59 years of age and 23 participants were 60 years or older. Among the 12 areas of Bekaa, the distribution of our subjects was as follows: Zahlé: 23 participants, Rayak: 48, Ksarnaba: 1, Aliel Nahri: 27, Chtaura: 5, Ablah: 21, Baalbek: 19, Ferzol: 13, Ain Kfarzabad: 12, Riit: 13, Sariine: 15 and Chmestar: 3 participants. The participants were randomly selected out of those who came to Rayak- Hospital, so the number of participants was not the same in all the regions but they were chosen randomly, nevertheless. Of the total population studied (N = 200), 77 (39%) of the participants were at high risk of developing diabetes and 123 (61%) were not. The use of the questionnaire made it possible to detect individuals at high risk in a simple approach. Of the participants at risk using the diabetes risk test score (n = 77), 69 (89.5%) subjects were actually diagnosed to have PD or T2D. Of the subjects satisfying the high risk profile, seventeen participants were diagnosed with PD, 52 were diabetic and 8 had neither (Figures 1 and 2).

Table 1. Study population charectiristics.
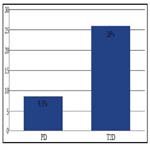
Figure 1. Prevalence of PD and T2D Among Subjects Meeting the any Risk Factor.
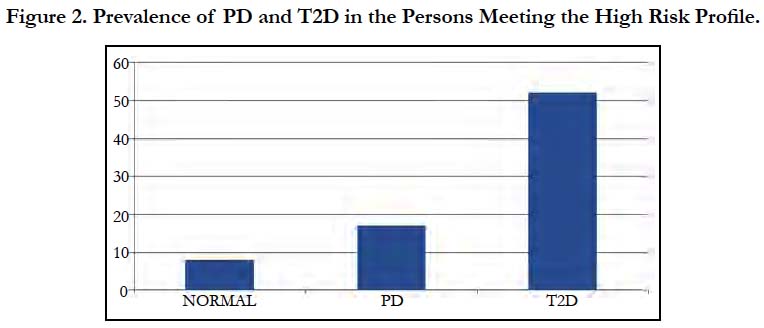
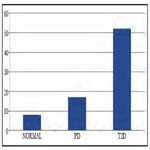
Figure 2. Prevalence of PD and T2D Among Subjects Meeting the High Risk Profile.
Among the study population (N = 200) and according to the ADA criteria, the prevalence of undiagnosed diabetes was 26%, and that of PD was 8.5% (Table 1).
Of 17 PD patients, 8 (47%) had an HbA1C value of 5.7 to 6%, and 9 (53%) had a value greater than 6. For diabetics (n = 52), 12 (23%) had HbA1c less than 7%, 33 (63.4%) had a HbA1C between 7% and 10%, while 7 (13.6%) had a HbA1C greater than 10 %.( Figure 3).
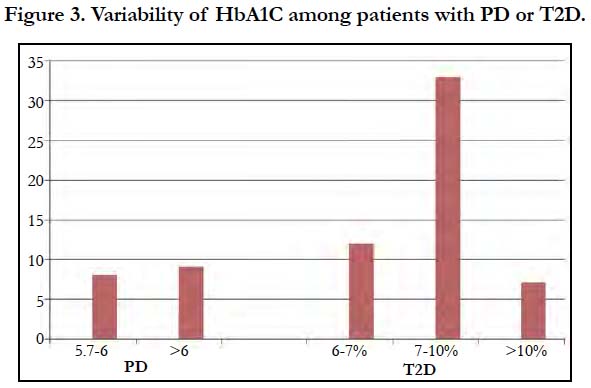
Figure 3. Variability of HbA1C among patients with PD or T2D.
The mean age of the participants diagnosed at risk of developing diabetes was 51.3 years ± 9.4 while those to be at risk was 34.1 ± 12.8 years. This statistical difference was very highly significant between the two groups (p <0.001) corresponding to the role of age as a risk factor for the disease. Looking at the gender of the participants (N = 200), 63 (51.2%) were women and 60 (48.8%) were men. Gender did not have an impact on developing diabetes. The difference in the incidence of PD and T2D between the two genders was not statistically significant (p = 0.66).
Among women in our cohort, 6 (7.8%) had a history of gestational diabetes and were diagnosed later on with diabetes. In contrast, among women without that risk (n = 123), according to the questionnaire, none developed diabetes. This difference was statistically significant (p = 0.004). Using a Chi-square test (χ2), we studied the influence of family history of diabetes on the risk of developing the disease. Of the subjects who did not have a risk of developing diabetes, 47 (38.2%) had a family history of the disease. As for the subjects who had that risk, 65 (84.4%) reported a family history of diabetes. This factor correlated significantly with the increased incidence of T2D development (p<0.001).
A proportional and very highly significant relationship was found between the presence of hypertension and the risk of having T2D (p<0.001). Of those at risk (n = 77), 46 (59.7%) hypertensive participants were diagnosed with PD or T2D. Only 11 (8.9%) of those with no hypertension had T2D. Tables 2 and 3 list the characteristics differentiating the subjects with risk factors and those with T2D.
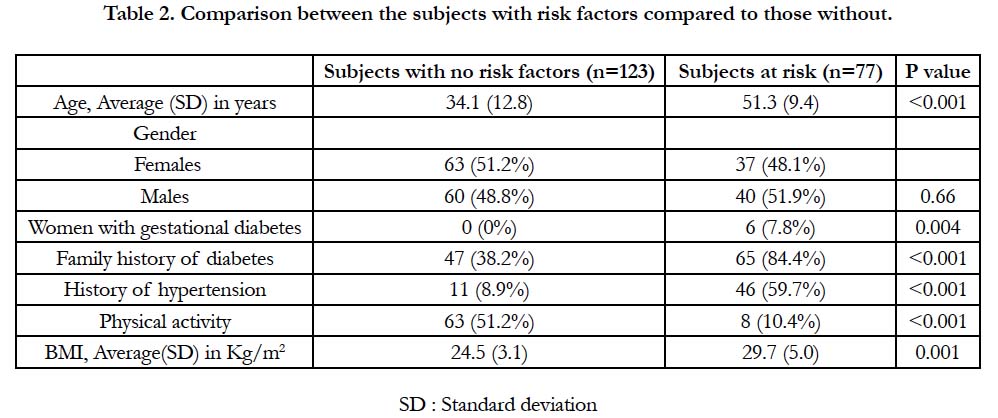
Table 2. Comparison between the subjects with risk factors compared to those without.
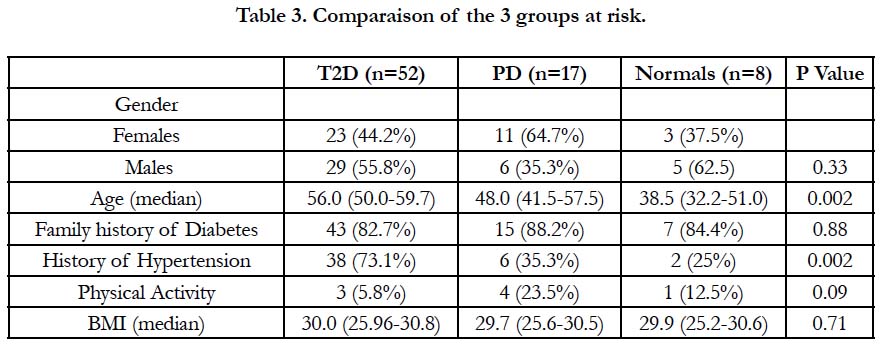
Table 3. Comparaison of the 3 groups at risk.
Persons at a lower risk of diabetes (n = 123), 63 (51.2%) were active, while 60 (48.8%) were sedentary. In contrast, only 8 (10.4%) of those at risk (n = 77) were physically active while 69 (89.6%) were sedentary. Statistical analyzes have shown a very highly positive relationship between regular sport and the absence of PD and T2D (p <0.001).
Participants who met the risk for T2D had an average BMI of 29.7 Kg/m2 ± 5.0 (Table 4) corresponding to overweight or obesity status. In contrast, the risk-free subjects were more likely to be normal-weight (BMI around 24.5 Kg/m2). These results were of highly significant (p = 0.001).
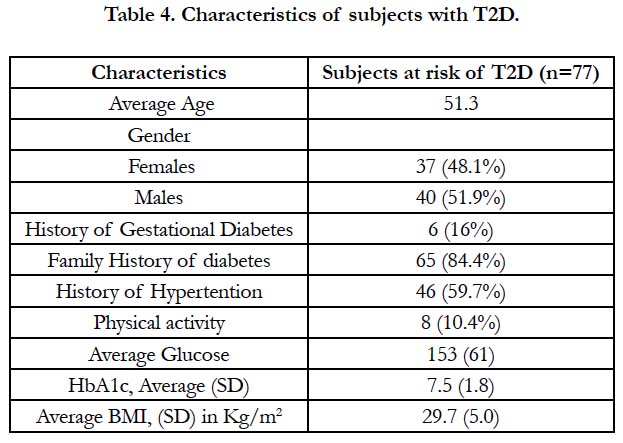
Table 4. Characteristics of subjects with T2D.
Discussion
Our finding are in agreement with those of other studies, proving the effectiveness of the questionnaire as a means of screening populations and assessing the risk of developing PD and T2D [8-10]. According to Rowan et al., a direct correlation was found between increased risk and increased HbA1c values leading to the diagnosis of PD and T2D. This was demonstrated in our study where most of the subjects screened at risk had an elevated HbA1c value leading to the diagnosis of PD or T2D [11]. Wu et al., found An incidence of 50% of undiagnosed T2D similar to our study [12].
In our study, the results obtained were similar to those presented by many others. The increased risk of developing diabetes increased with age, obesity, hypertension and physical inactivity, family history of diabetes and history of gestational diabetes [13, 14]. The equal risk among the genders has been reported by Çevik et al.. In contrast, Leahy et al., found that diabetes was more common among men than women, while pre-diabetes was similar for both sexes [15, 16]. His results were also in concert with our findings that participants who adopted a sedentary lifestyle had a high risk of diabetes compared to those who engaged in regular physical activity.
Our results on gestational diabetes as a risk factor are similar to a study by Chaudhry et al., which showed that women with a history of diabetes during pregnancy were at greater risk of developing T2D. According to Capula et al., this finding could be explained by the fact that gestational diabetes may represent an early stage in the natural history of T2D where pregnancy is a para-physiological condition of acquired insulin resistance. In addition, the pancreatic β-cell defect that characterizes gestational diabetes is chronic and not acquired during pregnancy and therefore this may explain the high risk of diabetes in women who have a history of gestational diabetes [17, 18]. Similar to the studies reported in the literature, we found that parental history of diabetes was positively associated with the incidence of T2D [8-10, 19].
According to the literature, and similar to our findings, hypertension was strongly associated with pre-diabetes and T2D [13, 20]. Our results were consistent with many other studies that analyzed the influence of physical activity on PD and T2D. For example, the study by Costanian et al., showed that lack of physical activity is an important factor in the development of T2D [15, 20, 21]. The association between weight and the risk of developing T2D was also reported in the literature. BMI was positively associated with the likelihood of diabetes and the prevalence of T2D was significantly increased with increasing BMI [20, 21].
Conclusion
This cross sectional study looks into the prevalence of PD and T2D in high-risk, undiagnosed patients. PD and T2D were very common among our subjects. Older age, personal history of gestational diabetes, family history of diabetes, the presence of hypertension, lack of physical activity and being overweight, were the factors that increased the risk of the disease significantly.
Our epidemiological study was the first conducted in Lebanon to assess the prevalence of PD and T2D in a rural population, using a questionnaire as a screening tool. It provided important data that the health authorities and physicians can use to reveal undiagnosed individuals who need medical attention.
However, limitations such as the disinterest and refusal of some people to participate in such assessments, as well as the bias of the questionnaire may be impediments to screen and discover everyone with undiagnosed T2D and PD.
Since the prevalence of diabetes is currently very high, it is advisable to apply this questionnaire at a broader or even national level: schools, social institutions and various businesses. This will contribute to the early discovery of diabetes in high-risk individuals and as a result to reduce the tremendous medical and financial burden of the disease and its complications.
References
- American Diabetes Association . Classification and diagnosis of diabetes. In Standards of Medical Care in Diabetes. Diabetes Care.2016;39(1):S13–S22. PubMed PMID:26696675.
- Naja F, Hwalla N, Itani L, Salem M, Azar ST, Zeidan MN, et al. Dietary patterns and odds of Type 2 diabetes in Beirut, Lebanon: A case–control study. Nutr Metab (Lond). 2012 Dec 27;9(1):111. PubMed PMID:23270372.
- Deepa M, Grace M, Binukumar B, Pradeepa R, Roopa S, Khan HM, et al. High burden of prediabetes and diabetes in three large cities in South Asia: The Center for cArdio-metabolic Risk Reduction in South Asia (CARRS) Study. Diabetes Res Clin Pract. 2015 Nov;110(2):172-82. PubMed PMID:26432412.
- Pillon F, Tan K, Jouty P, Frullani Y. Type 2 diabetes: the essentials on pathology. Pharmaceutical News. 2014 Dec 31;53(541):18-22.
- Van Ackerbroeck S, Schepens T, Janssens K, Jorens PG, Verbrugghe W, Collet S , et al. Incidence and predisposing factors for the development of disturbed glucose metabolism and Diabetes mellitus After Intensive Care admission: the DIAFIC study. Crit Care. 2015 Oct 2;19:355. PubMed PMID:26428846.
- Adegbija O, Hoy WE, Wang Z. Corresponding waist circumference and body mass index values based on 10-year absolute type 2 diabetes risk in an Australian Aboriginal community. BMJ Open Diabetes Res Care. 2015 Sep 16;3(1). PubMed PMID:26405557.
- Aguiar EJ, Morgan PJ, Collins CE, Plotnikoff RC, Callister R. Characteristics of men classified at high-risk for type 2 diabetes mellitus using the AUSDRISK screening tool. Diabetes Res Clin Pract. 2015 Apr;108(1):45-54. PubMed PMID:25707921.
- Zhang Y, Sun J, Pang Z, Gao W, Sintonen H, Kapur A, et al. Evaluation of two screening methods methods for undiagnosed diabetes in China: an costeffectiveness study. Prim Care Diabetes. 2013 Dec;7(4) :275 -82. PubMed PMID:24021478.
- Zhang L, Zhang Z, Zhang Y, Hu G, Chen L. Evaluation of Finnish Diabetes Risk Score in screening undiagnosed diabetes and prediabetesamong U.S. adults by gender and race. 2014 May 22;9(5) :e97865. PubMed PMID :24852786.
- Saaristo T, Moilanen L, Jokelainen J, Korpi-Hyövälti E, Vanhala M, Saltevo J, et al.Cardiometabolic profile of people screened for high risk of type 2 diabetes in a national diabetesprevention programme (FIN-D2D).Prim Care Diabetes. 2010 Dec;4(4):231-9. PubMed PMID:21134669.
- Rowan CP, Miadovnik LA, Riddell MC, Rotondi MA, Gledhill N, Jamnik VK. Identifying persons at risk for developing type 2 diabetes in a concentrated population of highrisk ethnicities in Canada using a risk assessment questionnaire and point-of-care capillaryblood HbA1c measurement.BMC Public Health. 2014 Sep 8;14:929. PubMed PMID:25196023.
- Wu Y, Ding Y, Tanaka Y, Zhang W. Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. Int J Med Sci. 2014 Sep 6;11(11).PubMed PMID :25249787.
- Zhang Y, Sun J, Pang Z, Gao W, Sintonen H, Kapur A, et al. Evaluation of two screening methods for undiagnosed diabetes in China: an cost-effectiveness study. Prim Care Diabetes. 2013 Dec;7(4):275-82. PubMed PMID: 24021478.
- He L, Tuomilehto J, Qiao Q, Söderberg S, Daimon M, Chambers J, et al.Impact of classical risk factors of type 2 diabetes among Asian Indian, Chinese and Japanese populations. Diabetes Metab. 2015 Nov;41(5):401-409. PubMed PMID: 26381573.
- Chevalier N, Fenichel P. Obésité, diabète de type 2 et perturbateurs endocriniens. La Presse Médicale. 2016 Jan 1;45(1):88-97.
- Leahy S, O' Halloran AM, O' Leary N, Healy M, McCormack M, Kenny RA, et al. Prevalence and correlates of diagnosed and undiagnosed type 2 diabetes mellitus and pre-diabetes in older adults: Findings from the Irish Longitudinal Study on Ageing (TILDA). Diabetes Res Clin Pract. 2015 Dec;110(3):241-9. PubMed PMID: 26520567.
- Chaudhry S, Doyle M, Nerenberg K, Malcolm J, & Keely E. The usefulness of the Canadian Diabetes Risk Assessment Questionnaire (CANRISK) in predicting dysglycemia in women with histories of gestational diabetes. Can J Diabetes. 2015 Dec; 39(6): 491-495. PubMed PMID::26162244.
- Capula C, Chiefari E, Vero A, Foti DP, Brunetti A, Vero R. Prevalence and predictors of postpartum glucose intolerance in Italian women with gestational diabetes mellitus. Diabetes Res Clin Pract.2014 Aug;105(2): 223-230. PubMed PMID:24931701.
- Wang R, Panizales M, Hudson M, Rogers S, Schnipper J. Preoperative glucose as a screening tool in patients without diabetes. J Surg Res. 2013 Jan;186(1): 371-378 . PubMed PMID:24148355.
- Ghassibe-Sabbagh M, Deeb M, Salloum A, Mouzaya F, et al.Multivariate epidemiologic analysis of type 2 diabetes mellitus risks in the Lebanese population. Diabetology & Metabolic Syndrome.2014 Dec;6(1):89.
- Costanian C, Bennett K, Assaad S, & Sibai A. Prevalence, correlates and management of type 2 diabetes mellitus in Lebanon: Findings from a national population-based study. Diabetes Res Clin Pract.2014 Jun 23; 105(3): 408-415. PubMed PMID:25005850.





