Iatrogenic Right Sided Infective Endocarditis in Children with CHD
H.S.Natraj Setty*, Vijayalakshmi IB, Narasimhan C, Manjunath CN
Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore, Karnataka, India.
*Corresponding Author
Dr. H.S.Natraj Setty MD DM,
H.no 493, 4th cross 7th main JP Nagar,
3rd phase Bangalore 69, Karnataka,
India.
Tel: 09845612322
Fax: 080-22977261
E-mail: drnatrajsetty75@gmail.com
Article Type: Review Article
Received: June 17, 2015; Accepted: July 31, 2015; Published: August 12, 2015
Citation: H.S.Natraj Setty, Vijayalakshmi IB, Narasimhan C, Manjunath CN (2015) Iatrogenic Right Sided Infective Endocarditis In Children With CHD. Int J Cardiol Res. 02(3), 34-36. doi: dx.doi.org/10.19070/2470-4563-150008
Copyright: H.S.Natraj Setty© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Right side infective endocarditis (IE) accounts for 5% -10% of cases of endocarditis. It is estimated that up to 76% of cases of endocarditis among intravenous (IV) drug abusers involve the right heart, compared with only 9% in non-addict patients. But occasionally right sided IE can also occur as a result of contaminated intravascular devices such as pacemakers, central venous lines and IV lines. We report four children aged 1 month to 5 years with right sided IE. The IE was due to IV lines used for parenteral injections and I.V. fluids. The commonest organism isolated was coagulase negative staphylococcus.
2.Background
3.Materials and Results
4.Discussion
5.References
Key Words
Tricuspid Valve; Intravenous Lines; Pulmonary Embolism; Coagulase Negative Staphylococcus; Inferior Vena Cava; Tetralogy of Fallot; Atrial Septal Defect; Ventricular Septal Defect.
Background
Right sided IE is a rare but well defined clinical entity in intravenous drug users, patients with pace makers or central venous line and with CHD [1, 2]. Right side endocarditis accounts for only 5% - 10% of cases of IE. The majority of cases involve tricuspid valve and pulmonary valve [3, 4]. Characteristic of isolated right sided IE in patients without a pacemaker and who are not intravenous drug users are poorly understood [5]. In this small series of four cases, we report children with involvement of the right sided IE secondary to IV lines used for injections and IV fluids. The clinical, microbiological, echocardiographic and prognostic profile is described.
The aim is to report clinical, microbiological and echocardio echocardiographic features of iatrogenic right sided IE in 4 children.
Materials and Results
Four cases of right sided IE who had presented between Sept 2013 to November 2013, age ranging from 1 month to 5 years, three females and one male formed the material. Two cases had VSD, one had a small ASD and one patient had TOF. They were very sick and moribund, presented with fever, breathlessness, chest pain and cough. All the four patients had history of prior admission to local hospitals, 15 days to 1 month prior for various conditions, other than CHD, Two cases were admitted and treated for lower respiratory tract infections (LRTI), one was for acute gastroenteritis and another for dengue fever. Anemia and leucocytosis was present in 3 children and the one patient of TOF with dengue fever had polycythemia, leucopenia and thrombocytopenia and was treated in children’s hospital with IV fluids, blood and platelet infusions. On admission to our hospital they were examined thoroughly, meticulously investigated and detailed echocardiography was carried out. The bacteria detector (Vitek 2 Compact Biomerieux) detected coagulase negative staphylococcus in two patients and gram negative bacilli in the one patient. In another case multiple blood samples were negative. The diagnosis of tricuspid valve endocarditis (Figure 1, Video 1) was established by transthoracic echocardiography (TTE) in all the four patients. One patient had vegetation in IVC (Figure 2) and in another case of VSD, large vegetation was seen closing the VSD (Figure 3, Video 2) and also large highly mobile vegetation (26X20mm) attached to ATL (Figure 4). Two antibiotics were given according to the sensitivity report. In two patients, with very large vegetation were referred for surgery. Only one patient was discharged after 6 weeks of antibiotics while 3 patients died (75%). The demographic details of all the four cases is given in Table I. Hypercoagulopathy work up was not done in any case.
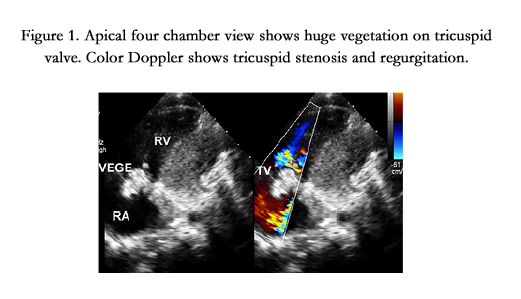
Figure 1. Apical four chamber view shows huge vegetation on tricuspid valve. Color Doppler shows tricuspid stenosis and regurgitation.
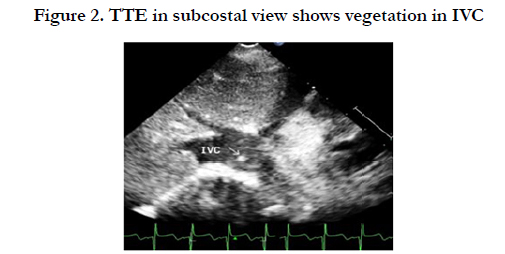
Figure 2. TTE in subcostal view shows vegetation in IVC
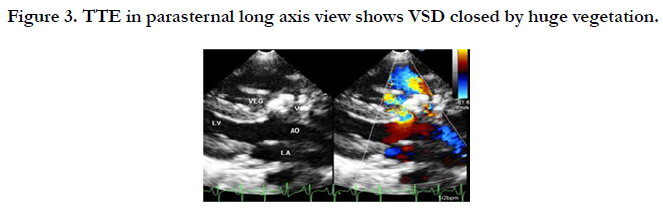
Figure 3. TTE in parasternal long axis view shows VSD closed by huge vegetation.
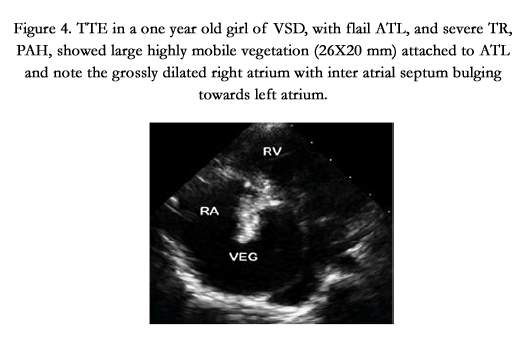
Figure 4. TTE in a one year old girl of VSD, with flail ATL, and severe TR, PAH, showed large highly mobile vegetation (26X20 mm) attached to ATL and note the grossly dilated right atrium with inter atrial septum bulging towards left atrium.
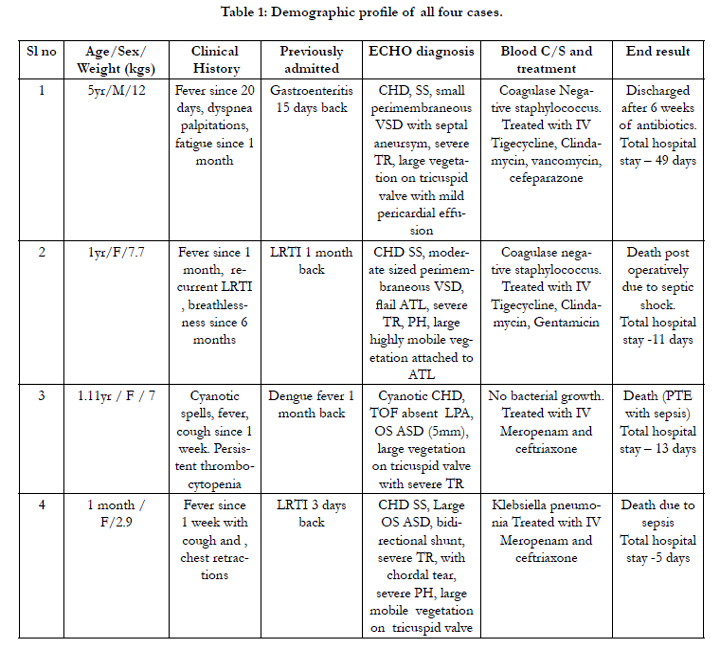

Table 1: Demographic profile of all four cases.
Video 1. Apical four chamber view shows pericardial effusion with large mobile vegetation appearing like bunch of grapes attached to anterior tricuspid and septal leaflets, the color Doppler shows the mosaic pattern caused by tricuspid stenosis and regurgitation.
Video 2. Parasternal long axis view with color Doppler shows, pericardial effusion with small closing in subaortic VSD with mobile vegetation on the right ventricular side of the VSD.
Discussion
Right sided endocarditis accounts for only 5 - 10% of cases of IE. Its clinical presentation differs from left sided IE. It has been estimated that up to 76% of cases of endocarditis among IV drug abusers involve the right heart, compared with only 9% in nonaddict patients. In most series Staphylococcus aureus, accounting for around 70-90 % of infections, with the remainder being caused mainly by streptococcal species. The coagulase negative staphylococcus was isolated in two of our patients. Traditionally surgery is indicated in: 1) Uncontrolled septicemia 2) Fever >3 weeks 3) Intractable CCF 4) Repeated occurrence of pulmonary embolism 5) vegetation > 20 mm 6) Concomitant left sided IE. Though our first patient had many indications for surgery, but was not operated (as consent was not given). But the patient survived and was discharged on the 49th day. Little information is available regarding the recent development of right sided IE [6]. The bacterial endocarditis is extremely rare in cases of ASD and TOF. This series of four cases is notable for the iatrogenic IE of tricuspid valve in children treated in the reputed hospital with IV injections for various unrelated conditions. The infection in this series occurred upon previously normal tricuspid valve. In our patients, IV lines for parental injection or the IV fluids were the probable culprits. In all the four patient TTE clinched the diagnosis of tricuspid valve vegetation causing tricuspid stenosis and regurgitation. These cases illustrate the importance of aseptic IV lines in children with underlying heart disease. Mortality in nosocomial infection is very high. Hence extra care must be taken while administering IV treatment in children with underlying heart diseases. Right sided endocarditis can occur in CHD patients when proper aseptic precautions are not taken while treating with IV injections. Mortality in iatrogenic right sided endocarditis is very high. Hence the timely blood culture and TTE are very important in diagnosis and management on a war footing.
References
- Robbins MJ, Soeiro R, Frishman WH, Strom JA (1986) Right-sided valvular endocarditis: etiology, diagnosis, and an approach to therapy. Am Heart J 111(1): 128-135.
- Cosson S, Kevorkian JP, Milliez P, Beaufils P, Cohen A (2003) A rare localization in right-sided endocarditis diagnosed by echocardiography: A case report. Cardiovascular Ultrasound 1: 10.
- Chan P, Ogilby JD, Segal B (1989) Tricuspid valve endocarditis. Am Heart J 117(5): 1140-1146.
- Frontera JA, Gradon JD (2000) Right-Side Endocarditis in Injection Drug Users: Review of Proposed Mechanisms of Pathogenesis. Clin Infect Dis 30(2): 374-379.
- Revilla A, López J, Villacorta E, Gómez I, Sevilla T, et al. (2008) Isolated right-sided valvular endocarditis in non-intravenous drug users. Rev Esp Cardiol 61(12): 1253-1259.
- Yuan SM (2014) Right sided infective endocarditis: recent epidemiologic changes. Int J Clin Exp Med 7(1): 199-218.





