Giant Condyloma Acuminatum (GCA; Buschke-Löwenstein Tumor): A New Case and Review
Guozhen L1*, Brian N. Parks2
1 Assistant Program Director, Family Practice Residency Program, Genesys Regional Medical Center, USA.
Associate Professor, Department of Family Medicine, School of Human Medicine, Michigan State University, USA.
2 Anesthesiologist, Henry Ford Hospital, USA.
*Corresponding Author
Guozhen Liu MD,
Assistant Program Director,
Family Practice Residency Program,
Genesys Regional Medical Center, USA.
Associate Professor, Department of Family Medicine,
School of Human Medicine, Michigan State University, USA.
Tel: 810-715-4300
Fax: 810-715-4326
E-mail: gliu757@gmail.com
Received: March 03, 2016; Accepted: March 11, 2016; Published: March 21, 2016
Citation: Guozhen L, Brian N. Parks (2016) Giant Condyloma Acuminatum (GCA; Buschke-Löwenstein Tumor): A New Case and Review. J Translational Clin Case Rep Fam Physician.2(2), 13-16.
Copyright: Guozhen L© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Giant Condyloma Acuminatum (GCA; Buschke-Löwenstein Tumor) is a rare sexually transmitted human-papillomavirus (HPV)-induced, large, exophytic, and cauliflower-like lesion of the anogenital region with a potentially fatal course. We report a case on a 57-year-old male with a 9-year history of a large slow-growing right inguinal/abdominal wall giant condyloma acuminatum.
2.Discussion
2.1.Pathology
2.2.Treatment
3.Conclusion
4.References
Case Report
The patient is a 57 year-old obese Caucasian male who presented with a nine-year history of a slow-growing right inguinal/ abdominal wall mass. The patient stated that the mass originally started as a “pimple” and over the course of the following 9 years the lesion grew to its present size. The mass had occasionally been followed by local family physician but the patient had refused previous treatment. The last few months he noted a progressive increase in pain, foul smell and occasional bleeding.
Physical exam revealed an 18.8-cm x 11-cm x 4.9-cm wartyappearing mass, red in color that was oozing serous fluid and some blood (Figure 1-2). The patient was anemic secondary to bleeding with hemoglobin of 7.3, hematocrit 24.3, MCV 64.5 and RDW 18. Two units of PRBC’s were transfused and no further transfusions were needed. Proteus mirabilis sensitive to Bactrim was cultured from the mass. The patients medical history revealed COPD, HTN, CHF, a history of hepatitis c. Patient has a history of smoking but recently quit.
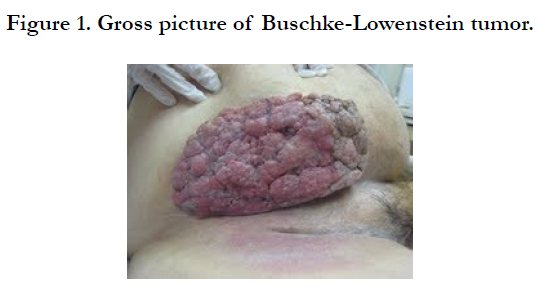

Figure 1. Gross picture of Buschke-Lowenstein tumor.
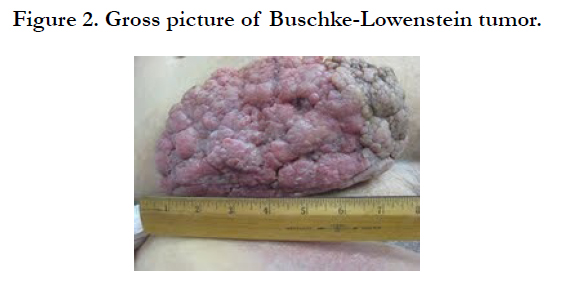

Figure 2. Gross picture of Buschke-Lowenstein tumor.
Surgery was consulted and a wide local excision was performed on a condylomatous, cauliflower-like skin tumor of right groin. The tumor involved the skin and subcutaneous tissue down to the facial plane. A skin graft taken from right upper thigh was used. Only 30% of the graft was taken.
Pathology of the mass showed giant condyloma acuminatum that appeared to be benign with a clear margin and was 18.8-cm x 11-cm x 4.9cm in size and weighed 686 grams. Microscopic description of the mass showed a cauliflower-like tumor characterized by epithelial acanthosis, papillomatosis, squamous epithelium with nuclear atypia, perinuclear clearing, and surface keratosis (Figure 3-6). Margins, where present, and appear free of tumor.
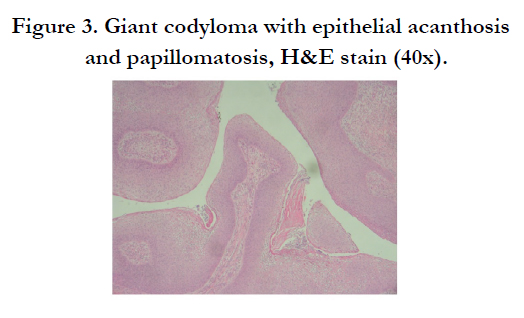
Figure 3. Giant codyloma with epithelial acanthosis and papillomatosis, H&E stain (40x).
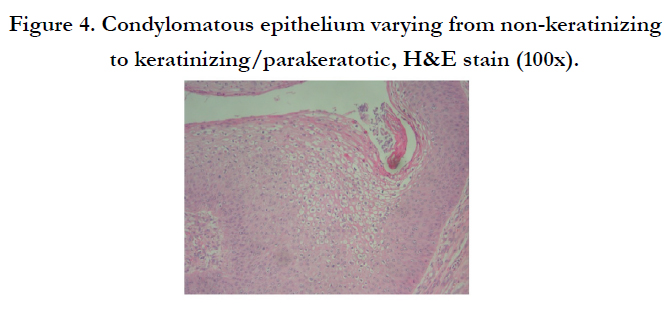
Figure 4. Condylomatous epithelium varying from non-keratinizing to keratinizing/parakeratotic, H&E stain (100x).
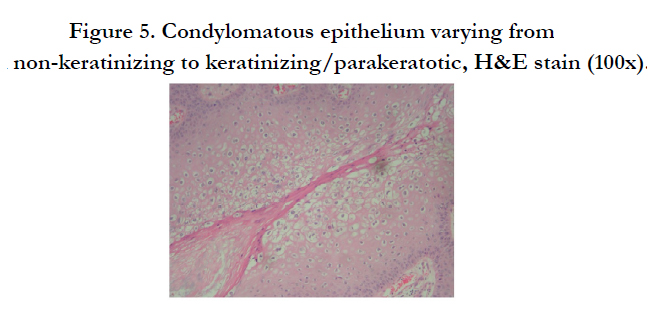
Figure 5. Condylomatous epithelium varying from non-keratinizing to keratinizing/parakeratotic, H&E stain (100x).
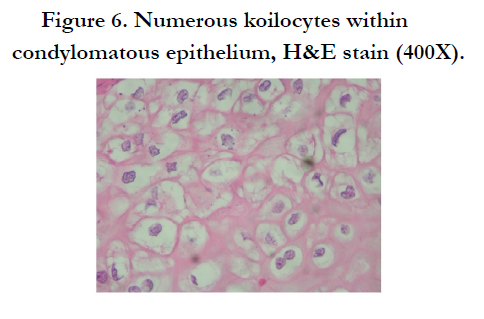
Figure 6. Numerous koilocytes within condylomatous epithelium, H&E stain (400X).
Discussion
Giant condyloma acuminatum (GCA; Buschke-Löwenstein tumor) was first described by Abraham Buschke in 1896. Buschke and Löwenstein (in 1925), further elaborated on GCAs [1]. GCA is an unusual, human-papillomavirus (HPV)-induced, large, exophytic, and cauliflower-like lesion of the anogenital region with a potentially fatal course. Even though GCA shows no histological criteria of malignancy, it is characterized by its size, capability of local infiltration, aggressiveness to underlying tissues, resistance to treatment, and a high recurrence rate [2-4]. The epidemiology, histology, malignant potential, treatment of the tumor and pathologic nature of GCA are still being debated.
In the reported literature there seems to be a predominance of GCA in males and a recent trend toward a younger age at presentation [2-5]. The most common presenting symptoms are anogenital mass, pain, abscess, fistula, bleeding, foul odor, weight loss, and pruritus. The overwhelming majority of cases have been reported on the penis and perianal locations [3, 5]. Other locations include the bladder [6], inguinal [7], pilonidal sinus [8, 9] and vulvar [10] regions.
GCA seems to be a sexually transmitted disease. When GCA or anogenital condylomas are found in children [11] the physician should question the possibility of sexual abuse. GCA has been reported in HIV-positive patients with some of those cases showing aggressive GCA with malignant potential [12, 13]. Sexual orientation or HIV status has been limited in the current literature making it difficult to see associations between HIV and GCA.
When 1st described by Buschke and Löwenstein GCA appeared to be a cytologically benign carcinoma-like variant of condyloma acuminatum. Since then there have been multiple cases where GCA has behaved in a malignant manner, so some authors have classified the GCA as a verrucous carcinoma (VC; a low-grade squamous cell carcinoma (SCC) with minimal metastasis risk). Other authors proposed that GCA is an intermediate entity between condyloma acuminatum and VC or SCC [2, 14].
Ordinary condylomas and GCA share many similarites. Histiologically they include koilocytosis (clear vacuolization of prickle cells in the superficial layer of the epidermis), infrequent mitosis, superficial hyperkeratosis, and acanthosis (epidermal thickening). GCA and simple condyloma acuminatum (anogenital warts) can be differentiated because GCA tends to affect the underlying tissue by characteristically “pushing” and displacing rather than “infiltrating” the basement membrane [15]. Histiologically GCA is also differentiated from common anogenital warts by its marked papillomatosis, thicker stratum corneum, and thickened rete ridges [3, 15].
It is not the malignant histology but the extent of invasion and high recurrence rate of the tumor that has the greatest impact on morbidity. From benign GCA to histologic malignancy the average time of malignant transformation is approximately five years [3]. The definition of GCA has been broadened to include giant condylomas that harbor foci of invasion [2, 3]. These areas of invasion may contain areas of frankly invasive VC or SCC. Although VC and SCC can be found within GCA, they can arise from normal skin. The definition of GCA now encompasses lesions that demonstrate the histologic features of GCA described above whether or not it coexists with areas of VC or SCC. In contrast to VC, GCA and ordinary condylomas have an intact basement membrane without invasion of the stroma and underlying tissue and do not have evidence of malignancy such as distant metastasis and lymphatic or angioinvasion [2, 3, 36].
The low-risk human papilloma virus types 6 and 11 have been frequently demonstrated to be associated with GCA [7, 24, 33-36]. It is unknown what host or viral factors cause the progression of benign condyloma acuminatum to an aggressive GCA phenotype.
It is reasonable when evaluating a patient for GCA to obtain a generous biopsy to see the broad, blunt, and deeply penetrating rete pegs and other histiologic features to help differentiate from condyloma, VC or SCC. In perianal disease with rectal involvement evaluation of rectum by proctoscope or flexible sigmoidoscopy should be used to rule out more proximal disease. If concerned about the extent of the tumor within the pelvis or to identify possible lymphadenopathy, a CT or MRI may be used [22]. GCA has a high recurrence rate [3], therefore vigilant follow up after treatment should occur.
In the literature many treatment strategies have been published (e.g. chemotherapy, excision, radiation) [23]. Most authors recommend complete surgical resection with histologically clear margins with or without adjunct chemotherapy [3, 24]. Early radical surgical excision has been suggested due to the clinical, pathologic and malignant potential of GCA [2, 3, 5, 25]. When there is involvement of the external anal sphincter, abdominoperineal resection should be considered [24, 25]. Resections with carbon dioxide [26, 27] and argon lasers have also been shown to be an alternative first-line treatment. There have also been reports of tumor destruction using cryotherapy or electrocauterization [28]. No further treatment is necessary if the margins are free of tumor, but vigilant follow-up is necessary due to its malignant potential and high recurrence rate.
Many different methods have been described for repairing the often large wounds caused by excision of a GCA tumor. (e.g. secondary healing, mesh-skin grafts, gracilis flap [17], split thickness grafts and S-plasty [29].
With varying success, topical and systemic chemotherapeutic agents with or without radiation therapy have been used as treatment or as adjuvants to surgery. Topical agents such as 5 fluorouracil, podophyllin, interferon have had little success in treatment or prevention of the disease [3, 11, 14]. Topical cidofovir gel 1.5%, intralesional bleomycin and intralesional interferon alpha [30] have shown to have some success. Systemic treatments include a variety of combinations of 5-fluorouracil, mitomycin, interferon alpha, bleomycin, cisplatin, leucovorin and/or methotrexate [23, 31-33].
Radiation therapy (XRT) has been used for successful treatment, salvage and as neoadjuvant treatment [34]. Although the idea has been challenged, radiotherapy was reported to be associated with malignant transformation of oral verrucous carcinoma [35], therefore it has been suggested that radiotherapy is contraindicated in the management for GCA. Chemoradiotherapy has resulted in significant down-staging of the disease allowing for local control and surgery possible [4, 33].
Immunotherapy with autologous vaccination has also shown good results in a few patients [36].
Conclusion
In summary, GCA can be defined as an unusual, humanpapillomavirus (HPV)-induced, large, exophytic, and cauliflower like lesion of the anogenital region with a potentially fatal course. GCA characteristically tends to “push” and displace rather than “infiltrate” the basement membrane and underlying tissue. GCA likely represents an intermediate entity between condyloma acuminatum and VC. Currently, complete surgical resection with clear margins is the treatment of choice. Adjuvant therapy may include chemotherapy, radiotherapy or immunotherapy. Controlled, prospective, multi-institutional studies are necessary to further understand and define the nature and treatment of this rare disease.
*We would like to extend a special thanks to Timothy Branigin MD for the histology slides.
References
- Buschke A, Löwenstein L (1925) Über carcinomähnliche condylomata acuminata des penis. Klin Wochenschr 4(36): 1726-1728.
- Creasman C, Haas PA, Fox TA Jr, Balazs M (1989) Malignant transformation of anorectal giant condyloma acuminatum (Buschke-Lowenstein tumor).Dis Colon Rectum 32(6): 481-487.
- Chu QD, Vezeridis MP, Libbey NP, Wanebo HJ (1994) Giant condyloma acuminatum (Buschke-Lowenstein tumor) of the anorectal and perianal regions.Analysis of 42 cases. Dis Colon Rectum 37(9): 950-957.
- Bertram P, Treutner K, Rübben A, Hauptmann S, Schumpelick V (1995) Invasive squamous-cell carcinoma in giant anorectal condyloma (Buschke-Löwenstein tumor). Langenbecks Arch Chir 380(2): 115-118.
- Trombetta LJ, Place RJ (2001) Giant Condyloma Acuminatum of the Anorectum: Trends in Epidemiology and Management: Report of a Case and Review of the Literature. Dis Colon Rectum 44(12): 1878-1886.
- Wiedemann A, Diekmann WP, Holtmann G, Kracht H (1995) Report of a case with giant condyloma (Buschke-Löwenstein tumor) localized in the bladder. J Urol 153(4): 1222-1224.
- Ergün SS, Kural YB, Büyükbabani N, Verim L, Akbulut H, et al. (2003) Giant Condyloma Acuminatum. Dermatol Surg 29(3): 300-303.
- Norris CS (1983) Giant condyloma acuminatum (Buschke-Lowenstein tumor) involving a pilonidal sinus: a case and a review of the literature. J Surg Oncol 22(1): 47-50.
- Mentes O, Akbulut M, Bagci M (2008) Verrucous carcinoma (Buschke- Löwenstein) arising in a sacrococcygeal pilonidal sinus tract: report of a case. Langenbecks Arch Surg 393(1): 111-114.
- Tewari M, Shukla H (2005) Giant Condylomata Acuminate Vulva in an adolescent girl. Indian J Surg 67(5): 278-279.
- Ambriz-González G, Escobedo-Zavala LC, Carrillo de la Mora F, Ortiz- Arriaga A, Cordero-Zamora A, et al. (2005) Buschke-Löwenstein tumor in childhood: a case report. J Pediatr Surg 40(9): e25-27.
- Valenzuela N, Barnadas MA, Matias-Guiu X, Curell R, de Andres L, et al. (2004) Lethal perianal Buschke-Löwenstein tumor in a female patient with AIDS. Dermatology 208(4): 349-350.
- Handisurya A, Rieger A, Bago-Horvath Z, Schellenbacher C, Bankier A, et al. (2009) Rapid Progression of an anal Buschke-Lowenstein tumour into a metastasising squamous cell carcinoma in an HIV-Infected patient. Sex Transm Infect 85(4): 261-263.
- Bogomoletz WV, Potet F, Molas G (1985) Condylomata acuminatum, giant condyloma acuminatum (Buschke-Lowenstein tumor) and verrucous squamous carcinoma of the perianal and anorectal region: a continuous precancerous spectrum? Histopathology 9(11): 1155-1169.
- Hull MT, Eble JN, Priest JB, Mulcahy JJ (1981) Ultrastructure of Buschke- Lowenstein tumor. J Urol 126(4): 485-489.
- Renzi A, Brusciano L, Giordano P, Rossetti G, Izzo D, et al. (2004) Buschke- Löwenstein tumor. Successful treatment by surgical electrocautery excision alone: a case report. Chir Ital 56(2): 297-300.
- Gholam P, Enk A, Hartschuh W (2009) Successful surgical management of giant condyloma acuminatum (Buschke-Löwenstein tumor) in the genitoanal region: a case report and evaluation of current therapies. Dermatology 218(1): 56-59.
- Lehn H, Ernst T, Sauer G (1984) Transcription of episomal papillomavirus DNA in human condylomata acuminata and Buschke-Löwenstein tumors. J Gen Virol 65: 2003-2010.
- Boshart M, zur Hansen H (1986) Human Papillomavirus in Buschke- Löwenstein tumors: physical state of the DNA and identification of a tandem duplication in the non-coding region of a human papillomavirus 6 subtype. J Virol 58(3): 963-966.
- Rubben A, Beaudenon S, Favre M, Schmitz W, Spelten B, et al. (1992) Rearrangements of the upstream regulatory region of human papillomavirus type 6 can be found in both Buschke-Lowenstein tumours and in condylomata acuminata. J Gen Virol 73(Pt 12): 3147-3153.
- Asato Y, Taira K, Yamamoto Y, Uezato H (2008) Detection of human papillomavirus type 11 in a case of Buschke-Löwenstein tumor. Eur J Dermatol 18(3): 329-331.
- Takezawa Y, Shimizu N, Kurokawa K, Suzuki K, Yamanaka H (1996) Appearance on magnetic resonance imaging of Buschke-Lowenstein tumor. Br J Urol 78(2): 308-309.
- Ilkay AK, Chodak GW, Vogelzang NJ, Gerber GS (1993) Buschke-Lowenstein tumor: therapeutic options including systemic chemotherapy. Urology 42(5): 599-602.
- Gingrass PJ, Bubrick MP, Hitchcock CR, Strom RL (1978) Anorectal verrucose squamous carcinoma: report of two cases. Dis Colon Rectum 21(2):120-122.
- Elliot MS, Werner ID, Immelman EJ, Harrison AC (1979) Giant condyloma (buschke-lowenstein tumor) of the anorectum. Dis Colon Rectum 22(7): 497-500.
- Frega A, Stentella P, Tinari A, Vecchione A, Marchionni M (2002) Giant condyloma acuminatum or buschke-Lowenstein tumor: review of the liturature and report of three cases treated by CO2 laser surgery. A long-term follow-up. Anticancer Res 22(2B): 1201-1204.
- Perisic Z, Lazic JP, Terzic B, Perisic S, Rasic R (2003) Condyloma gigantea in anal and perianal region: surgical and CO2 laser treatment. Arch Gynecol Obstet 267(4): 263-265.
- Renzi A, Giordano P, Renzi G, Landolfi V, Del Genio A, et al. (2006) Buschke- Lowenstein tumor successful treatment by surgical excision alone: a case report. Surg Innov 13(1): 69-72.
- De Toma G, Cavallaro G, Bitonti A, Polistena A, Onesti M, et al. (2006) Surgical management of perianal giant condyloma acuminatum (Buschke-Löwenstein tumor). Report of three cases. Eur Surg Res 38(4): 418-422.
- Geusau A, Heinz-Peer G, Volc-Platzer B, Stingl G, Kirnbauer R (2000) Regression of deeply infiltrating giant condyloma (buschke-löwenstein tumor) following long-term intralesional interferon alfa therapy. Arch Dermatol 136(6): 707-710.
- Zachariae H, Larsen PM, Søgaard H (1988) Recombinant interferon alpha- 2A (Roferon-A) in a case of Buschke-Löwenstein giant condyloma. Dermatologica 177(3): 175-179.
- Schwartz RA, Nychay SG, Lyons M, Sciales CW, Lambert WC (1991)Buschke-Löwenstein tumor: verrucous carcinoma of the anogenitalia. Cutis 47(4): 263-266.
- Tytherleigh MG, Birtle AJ, Cohen CE, Glynne-Jones R, Livingstone J, et al. (2006) Combined surgery and chemoradiation as a treatment for the Buschke-Löwenstein tumour. Surgeon 4(6): 378-383.
- Sobrado CW, Mester M, Nadalin W, Nahas SC, Bocchini SF, et al. (2000) Radiation-induced total regression of a highly recurrent giant perianal condyloma: report of case. Dis Colon Rectum 43(2): 257-260.
- Perez CA, Kraus FT, Evans JC, Powers WE (1966) Anaplastic transformation in verrucous carcinoma of the oral cavity after radiation therapy. Radiology 86(1): 108-115.
- Eftaiha MS, Amshel AL, Shonberg IL, Batshon B (1982) Giant and recurrent condyloma acuminatum: appraisal of immunotherapy. Dis Colon Rectum25(2): 136-138.





