Hairy Cell Leukemia with Atypical Presentation
Awale R1, Maji R1, Chhabra G1*, Chandra D2, Pati HP2, Mukhopadhyay AK1
1 Department of Laboratory Medicine,All India Institute of Medical Sciences, New Delhi, India.
2 Department of Hematology, All India Institute of Medical Sciences, New Delhi, India.
*Corresponding Author
Dr. Gaurav Chhabra,
Department of Laboratory Medicine,All India Institute of Medical Sciences,
New Delhi, India.
Tel: 9873651420
E-mail: gauravchhabra2001@gmail.com
Received: December 18, 2015; Accepted: January 06, 2016; Published: January 09, 2016
Citation: Chhabra G et al., (2016) Hairy Cell Leukemia with Atypical Presentation. J Translational Clin Case Rep Fam Physician. 2(1), 6-8.
Copyright: Chhabra G© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Hairy cell leukemia is a rare chronic lymphoproliferative disorder characterized by presence of characteristic hairy cell in peripheral blood or bone marrow, pancytopenia and splenomegaly. The diagnosis of hairy cell is usually based on presence of characteristic clinical features, morphology and immunophenotypic studies by flow cytometry. Hairy cell leukemia can sometime present with unusual characteristic clinical features therefore it is important to recognize these atypical presentations and associations in order to correctly diagnose and differentiate from other lymphoproliferative disorders.
2.Introduction
3.Case Report
4.Discussion
5.References
Keywords
Hairy Cell Leukemia; Leukemic Reticuloendotheliosis; Lymphoproliferative Disorders.
Introduction
Hairy cell leukemia or leukaemic reticuloendotheliosis is a rare chronic B cell malignant disorder characterized by infiltration of bone marrow and presence of typical hairy cells which are clone of mature B cells with cytoplasmic hairy projections in peripheral blood and bone marrow. Hairy cell is a rare disorder accounting for around 2% [1] of all leukemias and is characterized by insidious onset, pancytopenia and massive splenomegaly. Recurring infections are frequent and a major cause associated with poor prognosis in patients with hairy cell leukemia. Other unusual complications associated with hairy cell leukemia include lymphadenopathy, lytic bone lesions and skin lesions. We present a case of hairy cell leukemia with an atypical presentation with normal leukocyte counts, cellular marrow, lymphadenopathy and lytic bone lesions.
A 45 years old lady presenting with back pain and nodular skin lesions over extensor and flexor aspect of bilateral lower legs along with heaviness of abdomen for 45 days. Subsequent history of loss of appetite was also present. Physical examination revealed left cervical, right axillary and bilateral inguinal lymphadenopathy. On per abdomen examination spleen was markedly enlarged and palpable up to umbilicus. Liver was also enlarged and palpable 4 cm below costal margin.
Laboratory Investigations revealed Hemoglobin of 6.0gm %, Total leucocyte count of 4200/mm3, Differential cell count - 40% hairy cells (Figure1), Neutrophils-28%, Lymphocytes-30%, monocytes, eosinophils and basophils 1% each. Bone marrow aspirate was fairly (Figure 2) cellular with infiltration by 70 % hairy cells showing strong tartrate resistant acid phosphatase (TRAP) positivity (Figure 3) while biopsy was hypercellular with infiltration by hairy cells (Figure 4). Reticulin stain showed increase in pericellular fibrosis (Figure 5). Flow cytometric immunophenotyping was done and was found to be characteristically positive for CD 19, CD20, CD 11c, CD25 CD103 and FMC 7.
Skin biopsy from the nodular lesions showed features compatible with erythema induratum. Cervical lymph node biopsy showed involvement by hairy cell leukemia.
CECT showed diffuse septal thickening in both lungs with perilymphatic nodules, enlarged mediastinal nodes with few showing areas of necrosis. Scan revealed osteopenia with multiple ill defined lytic lesions in spine and pelvis. Thus a definitive diagnosis of HCL was made and in view of CECT findings anti tubercular treatment was started empirically along with treatment for HCL.
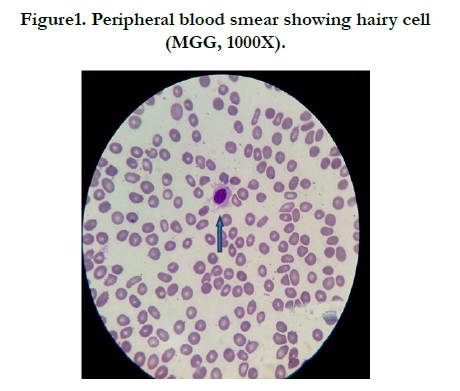
Figure1. Peripheral blood smear showing hairy cell (MGG, 1000X).
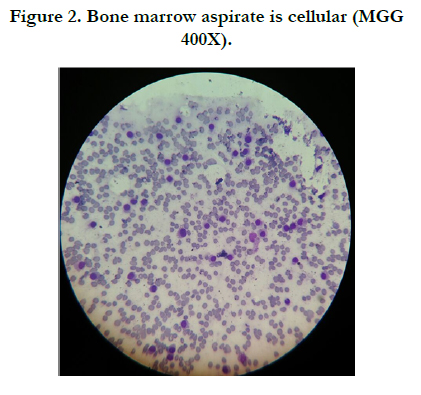
Figure 2. Bone marrow aspirate is cellular (MGG 400X).
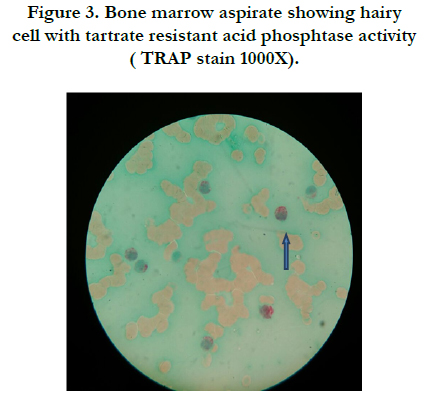
Figure 3. Bone marrow aspirate showing hairy cell with tartrate resistant acid phosphtase activity ( TRAP stain 1000X).
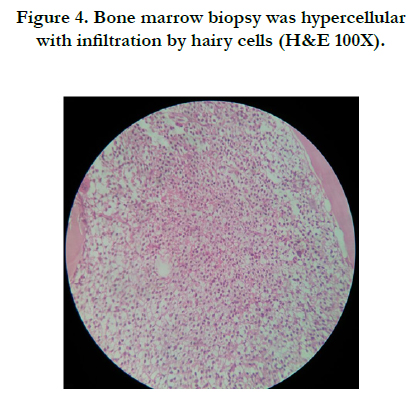
Figure 4. Bone marrow biopsy was hypercellular with infiltration by hairy cells (H&E 100X).
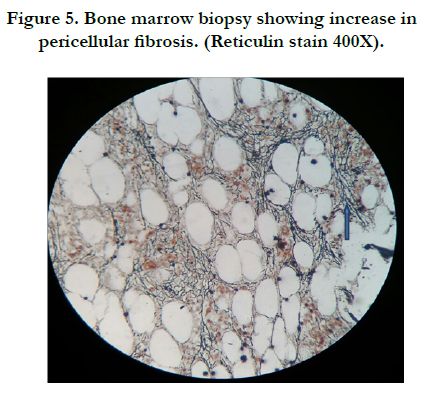
Figure 5. Bone marrow biopsy showing increase in pericellular fibrosis. (Reticulin stain 400X).
Discussion
Hairy cell leukemia is an indolent neoplasm of small mature B lymphoid cells and comprises 2% of lymphoid cells and it occurs more frequently in men (male:female - 4:1) [1, 2]. Common presenting features are splenomegaly, pancytopenia. Bone marrow aspirate is usually dry tap with increased reticulin fibrosis, immunophenotypic markers expression is characteristic [3]. The complications include lytic bone lesions, infections, multiple lymphadenopathy[4]. Among infections; mycobacterium tuberculosis is more common particularly in an endemic area. Mycobacterium tuberculosis infection was also strongly suspected in this case and patient was put on empirical treatment for tuberculosis. Similar findings were also reported by Arslan et al., [5] and Venkatesan et al., [6].
Present case is different in the sense that it presented with skin lesions and bone pain along with multiple lymphadenopathy.
In spite of lymph node and bone marrow involvement during presentation the patient did not have pancytopenia [6]. Bone marrow aspirate was cellular even when the biopsy showed fibrosis.
To summarize, HCL presentation can be without the typical feature but a high index of suspicion along with confirmation by ancillary techniques can attain proper and on time diagnosis and thus management of the patient.
References
- Goodman GR, Bethel KJ, Saven A (2003) Hairy cell leukemia: An update. Curr Opin Hematol 10(4): 258-266.
- Malfuson JV, Gisserot O, Cremades S, Doghmi K, Fagot T, et al. (2003) Hairy-cell leukemia: 30 cases and a review of the literature. Ann Med Interne (Paris) 154(7): 435-440.
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, et al. (2008) WHO classification of tumours of hematopoietic and lymphoid tissues. IARC, Lyon.
- Gaman AM (2013) Hairy cell leukemia- a rare type of leukemia. A retrospective study on 39 patients. Rom J Morphol Embryol 54(3): 575-579.
- Arslan F, Batirel A, Ozer S, Cağan Aktaş S (2013) A predisposing clinical condition for disseminated tuberculosis: Hairy cell leukemia. Mikrobiyol Bul 47(2): 346-350.
- Venkatesan S, Purohit A, Aggrawal M, Manivannan P, Tyagi S, et al. (2014) Unusual presentation of hairy cell leukemia: a case series of 4 clinically unsuspected cases. Indian J Hematol Blood Transfus 30(Suppl 1): 413-417.





