Diode Laser Assisted Management of Massive Fibromatous Vestibulum Fissuratum: Current Treatment Perspective
Kumar D1*, Soni BW2, Bhandari S3, Kumar V4, Rattan V5
1 Ex- Senior Resident, Oral and Maxillofacial Surgery, PGIMER, Chandigarh, India.
2 Senior Resident, Prosthodontics, PGIMER, Chandigarh, India.
3 Assistant Professor, Prosthodontics, PGIMER, Chandigarh, India.
4 Junior Resident, Oral and Maxillofacial Surgery, PGIMER, Chandigarh, India.
5 Head and Professor, Oral and Maxillofacial Surgery, PGIMER, Chandigarh, India.
*Corresponding Author
Dr. Dinesh Kumar MDS,
Ex-Senior Resident, Oral and Maxillofacial Surgery,
PGIMER, Chandigarh,India.
Tel: +91 9855995525
E-mail: dr_dinesh78@yahoo.com
Recieved: October 15, 2015; Accepted: October 26, 2015; Published: November 03, 2015
Citation: Kumar D, et al., (2015) Diode Laser Assisted Management of Massive Fibromatous Vestibulum Fissuratum: Current Treatment Perspective., J Translational Clin Case Rep Fam Physician. 01(1), 1-5.
Copyright: Kumar D© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The aim of this study was to present a case report of surgical removal of hyperplasia in the oral cavity using diode laser radiation and rehabilitation with a complete denture. Epulis fissuratum is a pseudotumor growth located over the soft tissue of the vestibular sulcus caused by the chronic irritation from the poorly adapted dentures. The case discussed in the present study reported with the massive fibrous mass (5x2x1 cm) with multiple folds located in the maxillary vestibular sulcus extending bilaterally from canine to canine region. This massive lesion was excised using diode laser and new complete dentures with proper peripheral extensions were fabricated and delivered to the patient. Patient was kept on regular follow up and clinical examination revealed normal vestibular mucosa and functionally sufficient prosthesis.
2.Introduction
3.Case Report
3.1.Postoperative care
3.2.Histopathology
4.Discussion
5.Conclusion
6.References
Keywords
Epulis Fissuratum; Diode Laser; Hyperplastic; Ill Fitting Dentures.
Introduction
Hyperplasia refers to the tissue growth into the oral cavity, located over the alveolar ridges or the soft tissues of the vestibular sulcus. The gingival mucosa is most venerable to such hyperplasia as it is exposed to constant irritation. There are numerous irritating factors that result in such reactive lesions such as ill fitting prostheses, inadequate chewing forces, entrapment of food debris, dental calculus, or other iatrogenic factors. Gingival tissue can react to these irritating factors by developing a lesion commonly known as epulis in dental practice [1, 2].
Epulis fissuratum is an inflammatory fibrous hyperplasia located over the soft tissues of the vestibular sulcus caused by the chronic irritation from poorly adapted dentures [Figure 1] [3]. Clinically, this adaptive lesion presents as a raised sessile lesion in the form of folds, with a normal coloured mucosa and a smooth surface [4]. This growth is often split by the edge of the denture, one part of the lesion lying under the denture and the other part lying between the lip or cheek and the outer denture surface [Figure 2]. This lesion may extend either on one or both sides of the denture.
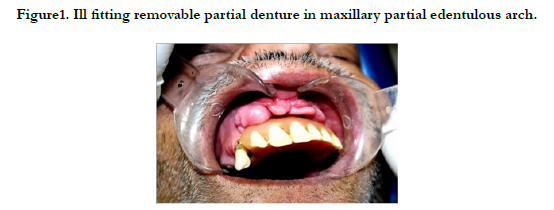

Figure1. Ill fitting removable partial denture in maxillary partial edentulous arch.
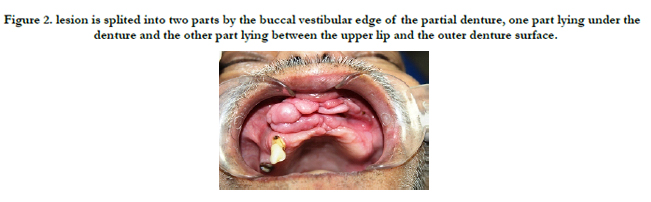

Figure 2. lesion is splited into two parts by the buccal vestibular edge of the partial denture, one part lying under the denture and the other part lying between the upper lip and the outer denture surface.
The treatment of this kind of mass/tissue includes elimination of the etiological factors, surgical excision of the hyper-plastic tissue by surgical scalpel, electrical scalpel or laser followed with appropriate prosthetic reconstruction [3, 4].
In the current scenario, lasers are the preferred means of executing soft tissue surgery in the oral cavity. The increased efficiency of surgical procedure combined with decreased morbidity and no electrical shortening even in the conductive environment are some of the reasons for transition towards laser assisted procedures over electrocautery in most of the soft tissue lesions in the oral cavity.
Here is presented a step by step protocol for the massive maxillary epulis fissuratum treatment of a patient with diode laser surgery and prosthetic rehabilitation.
Case Report
A seventy years old male reported in the unit of prosthodontics, postgraduate institute of medical education and research (PGIMER), Chandigarh, with the chief complaint of ill fitting dentures which he was wearing for past 10 years. Patient had a history of controlled diabetic mellitus and paralysis since 10 and 7 years respectively. The clinical examination showed partially edentulous maxillary and mandibular arches with a hyperplastic lesion over the maxillary alveolar ridge extending to the vestibular sulcus in maxillary anterior region. His overall oral hygiene status was poor.
In maxillary arch, right canine and root stump of 2nd premolar were the only teeth present while in mandibular arch bilateral canines, root stumps of right 1st premolar, left 1st and 2nd premolars were present. The maxillary partial denture was retained by only one C-clasp on right canine leading to inadequate retention and stability of the prosthesis. The labial flange of maxillary partial denture was over extended and impinging into the vestibule. Patient managed to use this ill fitting partial denture for past 10 years which ultimately lead to massive growth. A fibrous mass with multiple folds was located in the maxillary vestibular sulcus extending bilaterally from canine to canine region. Based upon the clinical examination and patient’s history provisional diagnosis of epulis fissuratum was made.
The complete treatment plan of excising the tissue under LA followed by conventional complete denture was explained and informed consent was taken from the patient before the treatment execution. The lesion was treated under local anaesthesia (2% lidocaine with 1:100,000 epinephrine) with aseptic technique using class IV diode laser (BIOLITEC, Germany) 980nm, fibre diameter 200 micron meter. The laser beam was applied in contact type mode through a malleable tip that could be bent desirably, on top of a straight hand piece. Power setting for the diode laser was 5-10 watt in continuous wave form and was adjusted according to the ease of use. Usual laser safety precautions for protecting the operator, patient, and assistant were strictly followed.
First, hyperplastic tissue was peripherally delimited using the diode laser in a focused mode. Then, using a suture to hold the lesion, tension was applied on each area of the lesion and the surrounding tissue to obtain a clean cut in the excision procedure. A fibrous mass of 5x2x1cm with multiple folds was excised [Figure 3]. At the end of the surgery the beam was used on a defocused mode to promote better haemostasis. Neither sutures nor dressings were used postoperatively and the wound was allowed to heal by secondary intention. Immediately after the surgery, remaining teeth and root stumps were extracted. Excised tissues were submitted for routine histopatological examination.


Figure 3. Images of the extirpated specimen showing an elongated lobulated mass with central splited line.
Postoperatively, no antibiotics were prescribed to patient. Analgesic was prescribed as and when required in the form of Acetaminophen 500mg. Mucopain gel was advised for local application. Patient was also advised to have cold and soft diet preferably semi-solid on the day of the procedure and to rinse with warm saline water 3-4 times after 24 hours. After one week, wound healing was in progress [Figure 4]. No postoperative pain or edema was reported.
The new complete dentures with proper peripheral extensions were fabricated and delivered to the patient. Patient was recalled after one month and clinical examination showed a normal vestibular mucosa and functionally sufficient prosthesis [Figure 5 & 6].
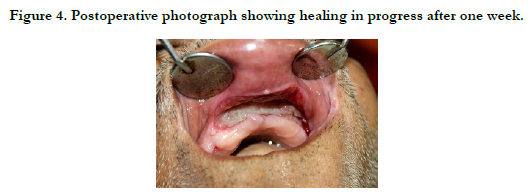

Figure 4. Postoperative photograph showing healing in progress after one week.
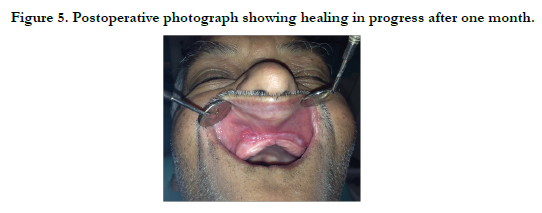
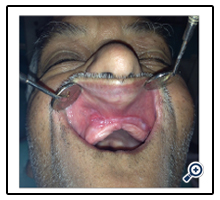
Figure 5. Postoperative photograph showing healing in progress after one month.


Figure 6. Photograph showing the complete denture.
Hematoxylin and eosin stained section showed polypoidal lesion with stratified squamous lining epithelium and focal ulceration. The ulcer bed was covered with fibrinous exudates and neutrophilic infiltrate. Subepithelial examination showed dense fibrocollagenous tissues with scattered lymphocytic infiltrate. Hisopathologic features were suggestive of non neoplastic, fibrous epulis fissuratum [Figure 7a, 7b and 7c].
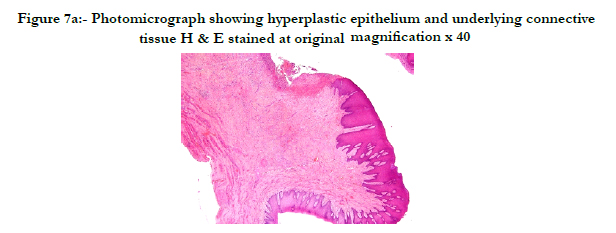
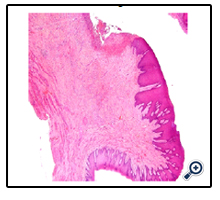
Figure 7a: Photomicrograph showing hyperplastic epithelium and underlying connective tissue H & E stained at original magnification x 40
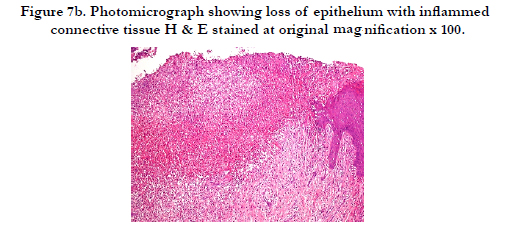
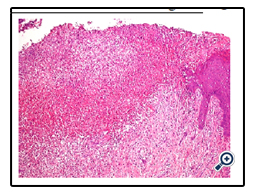
Figure 7b. Photomicrograph showing loss of epithelium with inflammed connective tissue H & E stained at original magnification x 100.
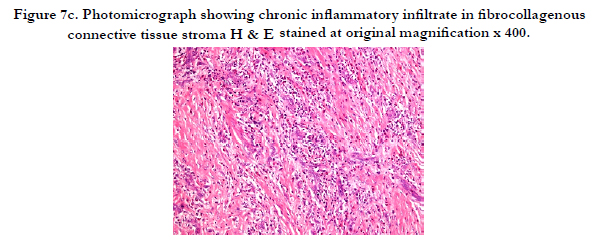
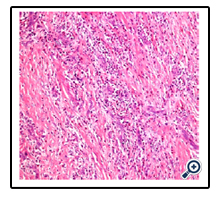
Figure 7c. Photomicrograph showing chronic inflammatory infiltrate in fibrocollagenous connective tissue stroma H & E stained at original magnification x 400.
Discussion
Majority of patients often manage to use ill fitting dentures for years without any major complaints. Only when some growth like ‘epulis’ arises then patients seeks attention for any dental treatment.
Epulis fissuratum is not a true tumour but an adaptive fibroepithelial response due a chronic low-grade irritation from poorly adapted prostheses with variable degrees of hypertrophy and hyperplasia. An epidemiological survey has found that it is more common in middle aged group females with an incidence of 3.5% in males and 4.4% in females [5].
The etiology of epulis fissuratum is mainly attributed to ill-fitting dentures which results in excessive pressure on the oral tissues, which in turn increases keratinization of epithelium and proliferation of connective tissues. The differential diagnosis of epulis fissuratum includes giant cell fibrous epulis, adamantinoma, burkitt’s lymphoma and fibrosarcoma [6]. Careful clinical examination and biopsy are indispensably important in the definitive diagnosis of the epulis [7]. The basic treatment available is the surgical excision of the lesion which can be performed by using conventional excisional biopsy, electro surgery or laser excision. Recent approach is laser therapy that is widely used for soft tissue surgery in the oral cavity [8]. Diode laser is a solid state semiconductor laser that typically uses a combination of gallium, arsenic, aluminium and indium to change electrical energy into light energy. The most commonly used wavelengths are 810, 940 and 980 nm, because
these wavelengths are well absorbed by pigmented tissues, haemoglobin and melanin, which makes the diodes suitable for soft tissue surgery, endodontics, periodontics and low level laser therapy [9]. At a wavelength of 980nm, the optical penetration is less which is potentially beneficial for treatment of superficial and interstitial lesions.
Amongst the different types of lasers available in dentistry, diode lasers are of relatively small size and have lower cost [10-12]. Goharkhay et al., [8] observed that with use of diode laser, neither lateral tissues were damaged nor charring of underlying bone was seen. On the other hand, several authors have reported that the use of CO2 laser can result in possible damage to the underlying bone [13]. Contrary to other investigations [14], deeper incisions could be achieved with the diode laser than that achieved by the other authors with CO2 or Nd:YAG laser. Romanos & Nentwig [15] found that the incision margins using the diode laser was more precise as compared with other systems, including CO2 and Nd: YAG lasers. Diode lasers account for its cutting precision and the uniqueness of its contact technique which offers the advantages like minimal intra-operative bleeding, thus rendering a clear surgical field and less operational time, disinfection of surgical site, rapid healing without scarring and minimal or no postoperative pain [16].
Laser treatment leads to sealing of blood, lymphatic vessels and nerve endings and thereby preventing the extravasations of fluids responsible for inflammation and pain and thus subsequent reduced post operative pain Surgical excision with scalpel and suturing leads to decreased vestibular depth [7, 17] while the wounds created by laser therapy contain fewer myofibroblasts, which are responsible for less wound contracture [18]. As expected, in the present case excellent postoperative vestibular depth was maintained which is important for achieving a correct peripheral seal for dental prosthesis retention and stability and preventing further recurrences.
The clinical results of the case report presented are coinciding with other studies utilizing laser for soft tissues. In the present case, the diode laser was used in continuous mode to control the extension of thermal damage using a focused beam to reduce its intensity.
Prosthesis with proper extension on a healthy site decreases the likelihood for recurrence. However, patient was kept under regular follow up and extensions of the prosthesis were also checked regularly. Therefore, patient should be properly educated and motivated before undertaking any treatment.
Conclusion
Diode laser is an excellent tool for the treatment of intraoral benign soft tissues. They offer several advantages over conventional modalities like allowing complete removal of the tissue without excessive bleeding, lesser wound contracture and decreased post operative discomfort. In contrast to CO2 lasers, diode laser don’t damage the underlying bone and deeper incisions may be achieved. Also the incisions margins are more precise as compared to CO2 and Nd:YAG lasers. The case presented demonstrates the ease of use along with better predictable results and patient can resume their regular activities with new prosthesis in comparatively less time than conventional surgery.
References
- Eversole LF, Rovin S (1972) Reactive lesions of the gingiva. J Oral Pathol Med 1(1): 30-38.
- Kfir Y, Buchner A, Hansen LS (1980) Reactive lesions of the gingival. A clinicopathological study of 741 cases. J Periodontol 51(11): 655-661.
- Tamarit-Borrás M, Delgado-Molina E, Berini-Aytés L, Gay- Escoda C (2005) Removal of hyperplastic lesions of the oral cavity. A retrospective study of 128 cases. Med Oral Patol Oral Cir Bucal 10(2): 151-162.
- Niccoli-Filho W, Neves AC, Penna LP, Seraidarian PI, Riva R (1999) Removal of epulis fissuratum associated to vestibuloplasty with carbon dioxide laser. Lasers Med Sci 14(3): 203-206.
- Mills JH, Lewis RJ (1981) Adamantinoma-histogenesis and differentiation from the periodontal fibromatus epulis and squamous cell carcinoma. CanVet J 22(5): 126-129.
- Dallas BM (1963) Hyperplasia of the oral mucosa in an edentulous epileptic. N Z Dent J 59: 54.
- Keng SB, Loh HS (1992) The treatment of epulis fissuratum of the oral cavity by CO2 laser surgery. J Clin Laser Med Surg 10(4): 303-306.
- Goharkhay K, Moritz A, Wilder-Smith P, Schoop U, Kluger W, et al. (1999) Effects on oral soft tissue produced by diode laser in vitro. Lasers Surg Med 25(5): 401-406.
- Gutknecht N (2007) Proceedings of the 1st international workshop of evidence based dentistry on laser in dentistry. Quintessence Publishing Co. Ltd, UK.
- Coleton S (2004) Lasers in surgical periodontics and oral medicine. Dent Clin North Am 48(4): 937-962.
- Andreana S (2005) The use of diode lasers in periodontal therapy. Literature review and suggested technique. Dent Today 24(11): 130-135.
- Deppe H, Horch HH (2007) Laser applications in oral surgery and implant dentistry. Lasers Med Sci 22(4): 217-221.
- Wilder-Smith P, Arrastia AM, Liaw LH, Berns M (1995) Incision properties and thermal effects of three CO2 lasers in soft tissue. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 79(6): 685-691.
- Perry D, Goodis H, White J (1997) In vitro study of the effects of Nd:YAG laser probe parameters on bovine oral soft tissue excision. Lasers Surg Med 20(1): 39-46.
- Romanos G, Nentwig G (1999) Diode laser (980 nm) in oral and maxillofacial surgical procedures: Clinical observations based on clinical applications. J Clin Laser Med Surg 17(5): 193-197.
- Gargari M, Autili N, Petrone A, Ceruso FM (2011) Using laser diodes for removal of the lesion of the oral mucosa. Case report. Oral Implantol (Rome) 4(1-2): 10-13.
- Pogrel MA (1989) The carbon dioxide laser in soft tissue preprosthetic surgery. J Prosthetic Dent 61(2): 203-208.
- Fisher SE, Frame JW (1984) The effects of the carbon dioxide surgical laser on oral tissues. Br J Oral Maxillofac Surg 22(6): 414-425.





