Sitz Bath Vs Iodine Antiseptic (Betadine) Imbibed Gauze for the Management of Perineal and Vaginal Tears
Eko F1*, Vivian V2, Fouelifack Ymele F1, Mbu R1,3,4
1 Obstetrics and Gynaecology Unit of the Yaounde Central Hospital. Higher Institute of Health Technologies Yaoundé, Cameroon.
2 Head of unit of Obstetrics and gynecology unit, District hospital of Cité Verte. Higher Institute of Health Technologies, Yaounde, Cameroon.
3 Obstetrics and Gynaecology Unit of the Yaounde Central Hospital Yaoundé – Higher Institute of Health Technologies, Yaoundé-Cameroon.
4 Head of unit of Obstetrics and Gynecology, Yaounde central hospital. Associate professor and coordinator of specialization cycle, Department of Obstetrics and Gynecology of Faculty of medicine and biomedical sciences-university of Yaounde, Cameroon.
*Corresponding Author
Eko Filbert,
Obstetrics and Gynaecology Unit of the Yaounde Central Hospital.
Higher Institute of Health Technologies Yaoundé,
Cameroon.
E-mail: fileko@yahoo.com
Article Type: Perspective Article
Received: December 26, 2014; Accepted: March 03, 2015; Published: March 09, 2015
Citation: Eko F, Vivian V, Fouelifack Ymele F, Mbu R (2015) Sitz Bath Vs Iodine Antiseptic (Betadine) Imbibed Gauze for the Management of Perineal and Vaginal Tears. Int J Translation Community Dis. 3(2), 59-63.doi: dx.doi.org/10.19070/2333-8385-1500011.
Copyright: Eko F© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aims: Sitz bath is a warm or cold bath used for healing or cleansing purposes. With over 85% of women having a vaginal birth who sustain some form of perineal trauma and placed on Sitz bath without really effectively applying it, we thought of proposing an alternative simpler and relatively effective method: iodine based antiseptic(betadine) imbibed gauze cleansing.
Study design: A randomized prospective trial
Setting and period: January 2009 to June 2009 in the central maternity of the Yaoundé Central Hospital because of the diversity and inflow of patients.
Methodology: All women who suffered a perineal or a vaginal injury during delivery and who gave consent were recruited, into different treatment groups depending on randomization, by filling a pre-established and tested questionnaire. Randomization was done with respect to the day of the week they suffered the injury. They were then followed up with specific appointments for 9days and the parameters of efficacy evaluated and compared among the randomly selected participants. Results were analyzed using the V9 SAS software analytical system and significance value was tested with p <0.05 and CHI square.
Results: We registered a 8% (94/1045) injury prevalence, episiotomies and tears together. After 9 days follow up of the randomized groups, the efficacy (degree of healing, infections, pain) was similar in the different treatment groups although compliance was better in the antiseptic imbibed gauze group than the sitz bath group.
Conclusion: Our results permitted us to conclude that the efficacies are comparable although the compliance was better with betadine gauze cleaning than Sitz bath. We recommend that a large scale with bigger sample size be carried out. While awaiting a broader scale that imbibed gauze cleaning of perineal injuries be used instead of Sitz bath as this will facilitate applicability and reduce perineal infections postpartum.
Limitations: Chronic pathologies like diabetes that could influence healing wasn't screened Same category of patients can be found on similar days particular to a treatment choice Some patients didn't respond correctly due to literacy level.
2.Introduction
3.The Material and Methods
4.Results and Discussions
5.Conclusion
6.Acknowledgement
7.Author's Contributions
8.Consent
9.References
Keywords
Efficacy; Iodine Based Antiseptic; Imbibed Gauze Cleansing; Sitz Bath; Episiotomy; Perineal Tear.
Introduction
A Sitz or hip bath is a warm water bath used for healing or cleansing purposes [1]. The patient sits in the bath and the water containing saline or medication covers only the hips and buttocks. Sitz bath is a European tradition in which only the pelvis and abdominal areas are immersed in water, with the upper body, arms, legs, and feet out of the water. The water can be warm or cold and one or two tubs maybe used [2].
Warm Sitz bath is one of the easiest and more effective ways to ease pain and lessen discomfort associated with a painful condition in the pelvic area. It was first introduced by Louis Kuhne in the late 19th and early 20th centuries in his detox bath methods including the friction Sitz bath [3].
Over 85% of women having a vaginal birth sustain some form of perineal trauma [2], and 60-70% receive stitches [2, 3]. There are wide variations in rates of episiotomy; 8-99 % [4-6].
Perineal trauma affects women’s psychological, physical and social wellbeing in the immediate postnatal period as well as the long term. It can also disrupt breastfeeding, family life and sexual relations. In the UK, about 23-42% of women will continue to have pain and discomfort for 10-12days postpartum and 7-10% will continue to have long term pain (3-18montths) after delivery [2, 3]. Sitting in warm water allows more blood to reach the impacted area, promoting healing and helping with any discomfort.
The efficacy of Sitz bath cannot be under estimated in the relief of pains, improvement of healing, amelioration of comfort. Reduction of inflammation has also been associated to its use. It is very helpful for a woman after childbirth whether or not she had a tear or episiotomy. We belief it is underused by our patients due to application difficulties in our hospital settings (lack of adapted tubs).
With this difficulty, patients find it practically impossible to carryout effectively the Sitz bath as prescribed while in hospital and even at home. We thought an alternative approach would be a common iodized antiseptic (betadine) imbibed warm gauze cleaning associated with simple first line analgesics. A method we belief will be more compliant and efficient compared to the Sitz bath.
Our main objective was to evaluate the efficacy of iodine antiseptic (Betadine®) imbibed gauze combined with first line analgesics in the management of perineal and vaginal injuries. Specifically we were to describe the profile of women with perineal and vaginal injuries, to determine the degree of perineal injuries, to determine the prevalence of perineal and vaginal injuries, to assess the degree of pain using the visual analogues method during the management of perineal and vaginal injuries using either methods, to compare the 2 methods in term of compliance, of rate of infection, of practicability and of the quality of healing. The study was carriedout in 6months in the maternity of the Yaounde Central Hospital because of patient affluence and diversity.
We didn't include patients who refuse giving consent, who didn't come back for control visit and all lost to follow up.
Material and Methods
We needed A4 papers, pen, computer, files, printer, ink, internet etc to carry out the study.
The principal investigator resided in the study site throughout the recruitment period of the study. All women who delivered in the study site were registered and examined after consent formalities. The different perineal and vaginal injuries were recorded. They were assigned to two groups after randomization.
The women enrolled on Mondays and Wednesdays were assigned to group A, the group that used Sitz bath for perineal and vaginal injuries while those who enrolled on Tuesdays, Thursdays and Fridays were assigned to group B. Women in the latter group used betadine imbibed gauze with first line analgesics for management.
They were explained the study objectives and those who did not wish to participate even at this level were excluded from the study.
The first part of the pre-established and pre-tested questionnaire was filled by the principal investigator.
The women who used Sitz bath were recommended to prepare the solution as follows: 1litre of warm water was added 5caps of gynecological betadine or a quantity of table salt to taste. They sat in the bath for 10-20 mins three times a day and after every time they pass stool.
Those who used betadine imbibed gauze were recommended to soak sterile gauze with the solution and clean the vulva three times daily and after every time they pass stool. Both groups combined 1000mg of paracetamol every eight hours or 400mg of Ibuprofen every 8hours for first line analgesic.
The women in the both groups started the respective procedure 6hrs after delivery.
They were evaluated on the 1st, 2nd and 9th day for remission of pain, the state of healing (inflammation, oedema and complete healing), presence of infection and difficulty in applicability.
Pain was evaluated using the Visual Analog Scale (VAS) at every instant. The scaled horizontal line of 100mm graduated from “0” to “10” was presented and explained to the patient. Point “0” signifies No pain while point “10” signified Unbearable pain. The patients placed a vertical mark on the line to indicate how bad they felt pain that particular day throughout the 9days of follow up.
Inflammation was evaluated by the degree of redness and oedema while infection was evaluated by the presence or absence of purulent discharge or gapping of stitches.
Efficacy was evaluated by the degree of healing, discomfort, remission of inflammation and pain.
The partially filled questionnaires were completed at each evaluation until the 9th day post-partum.
Completely filled questionnaires were analyzed using the V9 SAS analytical system and significance was tested if p<0.05 and also CHI Square.
Results and Discussions
We registered 1045 deliveries during the study period in the study setting. 82 had tears, 12 episiotomies totaling 94 (8% of injuries) --1% episiotomy and 7%tears (82% first degree, 18% second degree and no third degree).
More than 75% was of age between 20 and 35years, 56% of whom were married and about 14% were HIV positive (12 values of HIV status missing).70% had more than 1 child with 7% having more than 4 children.
80% compliance with the Betadine group as oppose to 15% of the Sitz bath group giving a p-value of 0.0001
Singles are more compliant than married women no matter the method but we found no relationship between marital status (pvalue =0.06) and parity (p-value = 0.52) and compliance.
We did not find any relationship between mean pain and treatment regimen (p-value= 0.61)
More of patients using betadine gauze (68.9%) got healed by the 9th day as compared to 58.3% of those using the Sitz bath regimen although it wasn’t statistically significant (p-value = 0.32).
We carried out a randomized control trial to evaluate its efficacy and compliance with respect to a simple perineo-vaginal cleaning with betadine soaked gauze.
From 1042 deliveries during the study period we registered 94 genital injuries (that’s 8%) consisting of 82 perineal tears and 12 episiotomies. The incidences are as in figure 1 and 2.
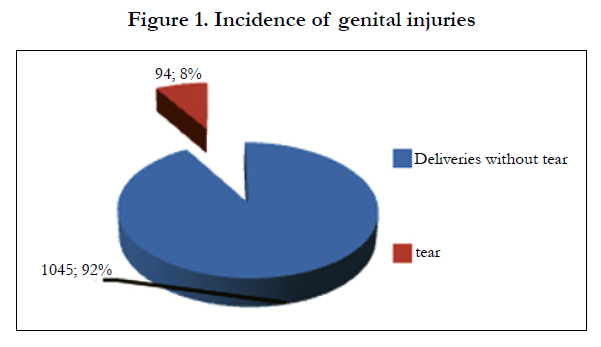
Figure 1. Incidence of genital injuries
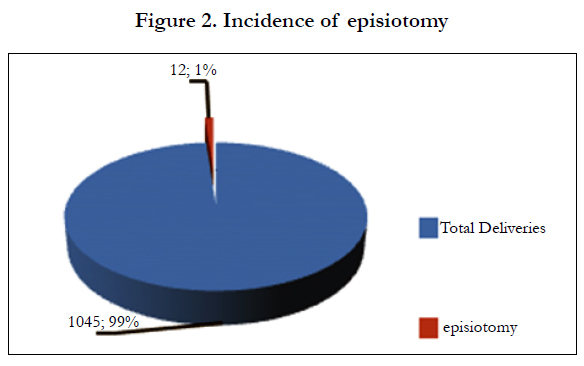

Figure 2. Incidence of episiotomy
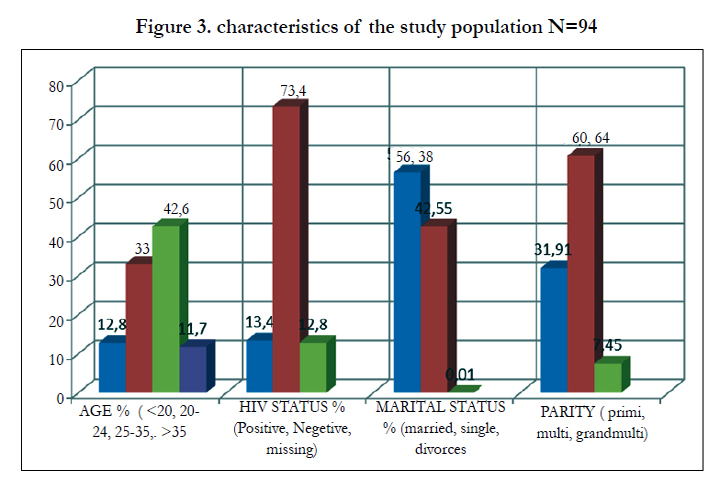
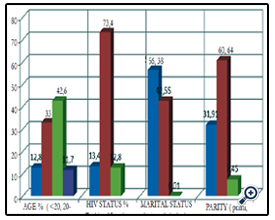
Figure 3. characteristics of the study population N=94
We therefore had a total of 94 women in our study population given us a genital injury percentage of 8% compared to international value of 85% [2]. Difficulty to acquire appropriate bath tubs was a major handicap for the application of the Sitz bath.
A majority of our women were in between the ages of 25 and 35 years (42.6%) and were married women (57%) as in table 1.
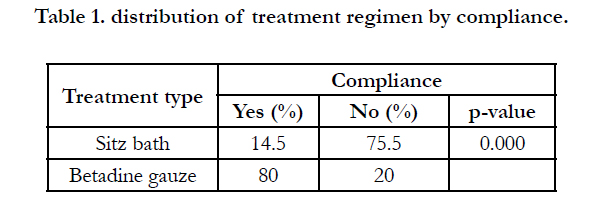

Table 1. distribution of treatment regimen by compliance.
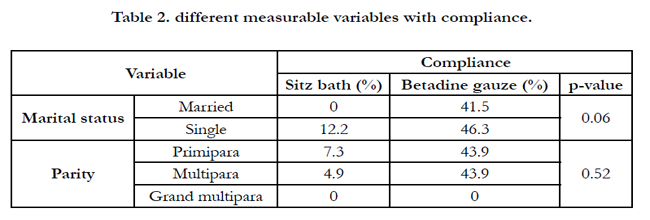
Table 2. different measurable variables with compliance.
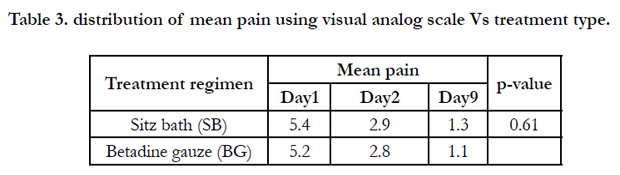
Table 3. distribution of mean pain using visual analog scale Vs treatment type.
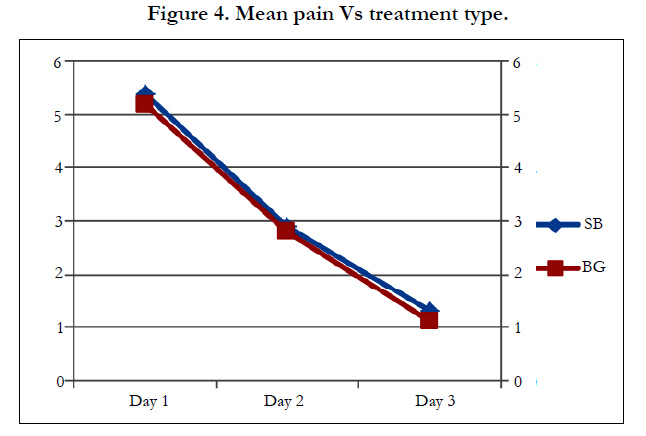
Figure 4. Mean pain Vs treatment type.
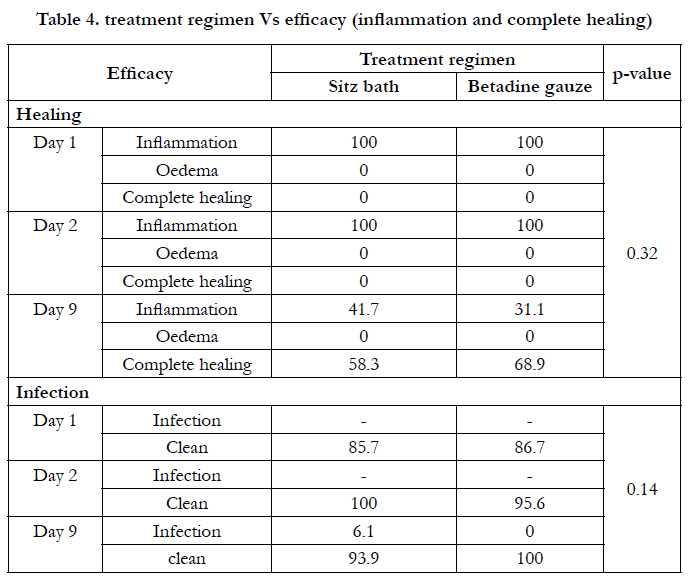
Table 4. treatment regimen Vs efficacy (inflammation and complete healing)
We had HIV prevalence in our series of 13.8% (not taken in to consideration the missing 12 values). This value is far above the 7.4% value in the national survey for pregnant women [7]. Mbu et al found a prevalence of 7 to 17% in 2001 depending on the area of the Nation [8].
Naturally, we would have think that bigger babies be proportionate with the severity of tears [9] but we didn’t find any influence of birth weight with the degree of tear.
This might be explained in the sense that our analysis didn’t consider separately the birth weight and tear with respect to their parity. That is primipara and multipara were not considered separately with their consequent tears.
Episiotomies were more frequent with primiparas (58.3% as compared to 39.1% in a UK series [10] and 77.1% in a Nigerian series [11]. We had a general prevalence of episiotomy of 5.3% in our series. This prevalence varies widely throughout the globe with 8% in the Netherlands, 14% in England, 50% in the USA and up to 94% in Eastern Europe countries [1, 3, 12].
Assessing the efficacy of the different treatment regimens, we found out the mean pain decreased steadily and similarly in both groups.
Healing was also similar independent of the treatment regimen although more patients (65% Vs 58%) achieved complete healing with Betadine by the 9th day of treatment. We used only the warm sitz bath is our series since this was the tradition even though cold sitz bath has been reported to reduce oedema than the warm sitz bath [13]. Assessing the infection state of the wound, a 100% success as compared to 94% was achieved with the betadine group although not statistically significant.
We didn’t find any statistically significant difference (P values 0,32; 0,61 and 0,14 respectively) between the two groups in the healing, reduction of pain and infection.
Conclusion
We finally conclude that the two methods are comparatively efficient if adequately applied. Compliance and efficacy as well as cost permit us to advocate for betadine imbibed gauze protocol for the management of perineal and vaginal injuries.
Acknowledgement
We want to thank the staff of the Central Maternity of the Yaounde Central Hospital for their support in carrying out deliveries and notifying tears and episiotomies. We acknowledge the administration and colleagues of the Gynecology and Obstetrics Unit of the Yaounde Central Hospital for their assistance and encouragement throughout the study period. We thank Dr Feunou Felix for his help in the statistical analytic assistance and finally, we acknowledge our families for support, tolerance and inconvenience we burdened them throughout the period.
Author's Contributions
Dr Filbert Eko designed the study, performed the statistical analysis, wrote the protocol, and wrote the first draft of the manuscript. Dr Vivian Verbe assisted in the write ups and literature search on the topic. Dr Fouelifack managed the analyses of the study. All authors read and approved the final manuscript. Professor Mbu Robinson did the general supervision from conception to finalization of the manuscript.
Consent
All authors declare that ‘written informed consent was obtained from the patients (or their relevant) for publication of this manuscript. A copy of the written consent is available for review by the Editorial.
References
- Benjamin W. Van Voorhees, MD, MPH, Review provided by VeriMed Healthcare Neywork Chicago,IL .
- McCandlish R, Bowler U, Asten H, Berridge G, Winter C, et al. (1998). A randomised controlled trial of care of the perineum during second stage of normal labour. BJOG: an international journal of obstetrics & gynaecology. 105(12):1262-1272.
- Sleep J, Grant A, Garcia J, Elbourne D, Spencer J, et al. (1984). West Berkshire perineal management trial. Bmj, 289(6445), 587-590.
- Wagner M. (1994) Pursuing a birth machine: the search for appropriate technology. Camprerdown: ACE Graphics. 165-174
- Statistical bulletin- NHS Maternity Statistics, England: 2001-2002. London: department of Health, 2003
- Graves E. J, Kozak L. J (1999) National hospital discharge survey: annual summary, 1996. Vital and health statistics. Series 13, Data from the National Health Survey (140), i-iv.
- Republic of Cameroon, Ministry of Public Health. (2004)Antiretroviral therapy in pregnant women and the prevention ofHIV infection in children in Cameroon. Guidelines on the Use.
http://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0CB4QFjA A&url=http%3A%2F%2Fwww.unicef.org%2Ffrench%2Faids%2Ffiles%2 Fhiv_pmtctfactsheetCameroon.pdf&ei=if73VJOAL46wuATm1IHQBQ& usg=AFQjCNFQJ-bWg-jytQcLiEXSW9bXi9TKYg&sig2=974UAftZ53ljvON7Lv5Jg. - Mbu R, Mfopi Keou F, Maka J, Leke R, Eteki N (2001) Impact of HIV on pregnancy outcome in Yaounde. Journal Camerounais de Médicine 1(10):61.
- Sultan AH, Kamm MA, Bartram CI, Hudson CN (1994) Perineal damage at delivery. Contemporary Reviews in Obstetrics & Gynaecology 6:18-24.
- Williams F. L. R, Florey C. D. V, Mires G. J, Ogston S. A (1998) Episiotomy and perineal tears in low-risk UK primigravidae. Journal of Public Health 20(4):422-427.
- Enyindah C. E, Fiebai P. O, Anya S. E, Okpani A. O (2006) Episiotomy and perineal trauma prevalence and obstetric risk factors in Port Harcourt, Nigeria. Nigerian journal of medicine: journal of the National Association of Resident Doctors of Nigeria, 16(3):242-245.
- Wagner M. Pursuing the birth machine: the search for appropriate technology. Camperdown: ACE Graphics, 1994; 165-174
- Tejirian, T., & Abbas, M. A. (2005). Sitz bath: where is the evidence? Scientific basis of a common practice. Diseases of the colon & rectum, 48(12), 2336-2340.





