The Dialogical Process in Three Different Diagnostic Procedures and Therapy Approaches
Löffler-Stastka H*, Bukowski X, Finger-Ossinger M, Grillmeier-Rehder U, Kotlowski I
Postgraduate University Programme Psychotherapy Research, Dept. of Psychoanalysis and Psychotherapy, Medical University Vienna, Austria.
*Corresponding Author
Henriette Löffler-Stastka,
Postgraduate University Programme Psychotherapy Research,
Dept. of Psychoanalysis and Psychotherapy,
Medical University Vienna, Austria.
E-mail: henriette.loeffler-stastka@meduniwien.ac.at
Article Type: Research Article
Received: December 05, 2014; Accepted: February 28, 2015; Published: March 03, 2015
Citation: Löffler-Stastka H et al., (2015) The Dialogical Process in Three Different Diagnostic Procedures and Therapy Approaches. Int J Translation Community Dis. 3(2), 55-58. doi: dx.doi.org/10.19070/2333-8385-1500010
Copyright: Löffler-Stastka H© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Clinical reasoning and diagnostic processes are easy to be applied by the experienced clinician. Clinicians with their implicit knowledge gather experiences, some build up guidelines, search for consensus statements, but the practical point of the procedure is an underrepresented research topic: First, the components of efficient processes have to be elucidated: The affectively involving “now moment” facilitates initial treatment processes. In order to produce such communication processes a dialogical process including empathy, respect, authenticity and reflective functioning has to be establish. Three psychotherapeutic methods describe their way of establishing such a dialogical process in order to meet best practice diagnostic procedures. An empirical evaluation of the therapeutic processes with the AREQ and PQS, based on the q-sort methodology, illustrates the interaction and change process, especially significant “now moments”. As these moments are essential for clinical work patient-doctor-communication processes should focus on such affectively.
2.Introduction
3.The Dialogical Process
4.Discussion
5.References
Keywords
Dialogical Process, Now-Moment, Therapeutic Relationship, Psychoanalysis, Humanistic Psychology.
Introduction
Diagnostic procedures in psychotherapy depend on a dialogical process. It involves the patient’s health profile, his subjective theory of disease, his and the therapist’s belief system and image of human being. Using classification systems such as DSM5 or the ICD-10, a purely formal diagnosis following the ideal norm is set. Even though operationalization (e.g., OPD) inhibits the dynamics of the conversation, it is necessary in order to avert random definitions of diseases [17]. At the outset, the initial interview provides the possibility to classify the occurring symptoms and to adapt the intervention techniques to the needs as well as the possibilities of the patient [18].
In psychoanalysis the attention is focussed more on the subjective feelings of the patient. The scenic comprehension is also important since the patient not only communicates consciously and verbally but also unconsciously and nonverbal. In this way, the patient has enough space for the active design of the initial interview. But the therapist needs still to focus on the transference- and countertransference processes. Regarding this ‘balanced attention’, more empathy can contribute towards emotions and impulses of the patient [12].
Kernberg developed the structural interview as one possibility to work under differential diagnostic circumstances in addition to the above-mentioned points. The focus is on the current and past symptomatology, the concept of self and others and on the quality of the interaction between patient and therapist [23]. In addition there are further structural measuring instruments, such as the STIPO, SWAP, Reflective functioning scale which are important for the description of intrapsychic structural characteristics of patients [5]. The higher the fit between diagnosis and intervention, the more effective the therapy is designed.
By contrast the humanistic psychology is strongly influenced by a positive, upbeat concept of humanity. Rogers, representing the conversational therapy, assumes a high level of personal control and self-determination. On one side the therapist acts more passive and follows the client, on the other side he also actively interferes. In this way the therapist engenders a relationship on equal terms. At the beginning the therapist focuses only on the design of a good and well-established therapeutic relationship. Here the humanistic approach overlaps strongly with the psychodynamic method, more than assumed by both sides. From a psychodynamic point of view, however, the humanistic psychotherapy exerts mainly an accompanying function and risks that after the end of therapy the patient's symptoms remain. For instance, because the patient didn’t recognize his own resources and thus didn’t know how to use them [19].
In terms of a radical constructivism it’s important to clarify the definition of objectives together with the client in a process of dialogue and to focus on the initial interview.
In order to evaluate and quantify the dialogical process through an independent research team the following instruments were applied:
The Affect Experience and Affect Regulation Q-sort [16], an observer-based Q-sort designed to assess affective experience (including affect intensity, lability, and tendency to experience particular emotions) and affect regulation (including a range of conscious and unconscious procedures used to increase pleasant and decrease unpleasant emotions). It yields three factors of affective experience: socialized negative affect (e.g., guilt), positive affect (e.g., interest), and intense negative affect (e.g., anger). The affect regulation dimension includes three factors: reality-focused response (e.g., goal-directed coping), externalizing defenses (e.g., projection), and avoidant defenses. Internal consistency of the factors in previous research is acceptable to high, as is interrater reliability or external validity of the factor scores. In this study, inter-rater reliability showed sufficient consistency (median-K = .70, min = .10, max = .95)
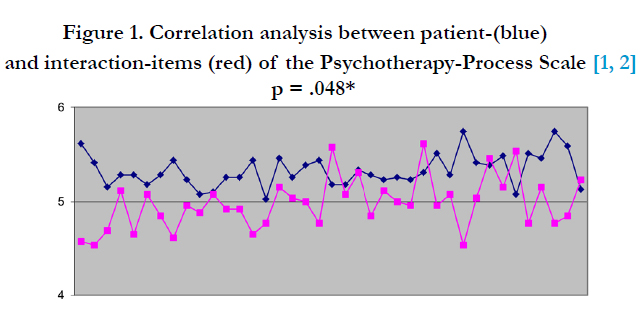
The Psychotherapy-Process Scale [1, 2, 13] assessed psychotherapeutic technique and processes. The PQS is a pan theoretically developed instrument that provides a comprehensive language and rating system for describing psychotherapy processes. It consists of 100 items (i.e., the “Q set”) covering actions, behaviors, and thoughts of both therapist and patient in individual and dyadic terms (e.g., “Therapist suggests that patient accept responsibility for his/her problems”; “Patient expresses angry or aggressive feelings”), as well as interaction items. Interrater reliability was stable at K = 0.87. Correlational analyses were performed using SPSS 20.0; results were considered significant at an error Ievel of 5%.
"The Dialogical Process"
The following case vignettes illustrate the diagnostic procedure; all three patients are prototypically successful treatment engagers, could start and proceeded in prosperous therapeutic treatments, although they all were suffering from severe disturbances:
“Mr. S was treated according to the criteria of the person-centered psychotherapy at a forensic outpatient department. Due to the patient's multiple traumata, the psychodynamic imaginative trauma therapy after Reddemann was applied” [6].
A safe working alliance and a good therapeutic relationship are important factors in the course of therapy. The constitution of the relationship depends on the severity of the patient’s diseaseThe constitution of the therapist depends on the different concepts developed by the individual therapy systems [20]. Furthermore, especially the psychoanalyst tries to maintain an adult working relationship, while humanistic methods work mainly supportive and thus contribute to the activation of resources by selfexploration, the strengthening of contact and the self-support and finding of his own interpretations and meanings by the patient.
Further, mental processes are mediated by emotions that are themselves experienced through thoughts and somatic signals -from a neuroscientific perspective emotions are perceived as changes in body states [21].
Activating these emotionally significant events in the life of the patient may result in reactivation of the emotions in the current therapeutic situation [4]. Emotional interaction regulation requires empathy on the part of the therapist and a mentalization ability by the patient. Referring to Freud, Bion (2002) also describes the non-psychotic part that develops simultaneously with psychotic elements. Both parts exist in every person, whereas the non-psychotic part at the majority is distinctly greater and the psychotic one more isolated. If the structure reverses, various forms of therapy use different treatment options. The psychoanalysis focuses on the early interpretation of the dominant affect in the activated transference relationship. The mentioned humanistic approach focuses the treatment on security, regulation and control, and affective containment [15].
"After many "ups and downs" in the process, Mr. S had a incisive experience with a drunken roommate, who gave him a slap. The result was that Mr. S. cancelled the following therapy session due to illness. In the next session the sentence "It never ends." accompanied him. His sadomasochistic parts could be worked through.
This unexpected event interrupted the therapeutic process, initially created an instability and changed the behavior of the patient. Such affective highly occupied 'now-moments' are for all participants “unfamiliar, unexpected in their act from timing, unsettling or weird” [22]: ,,Mr. S reported a massive crash. He later described his flashbacks as an outlet for a clogged pipe that could now be cleaned. Toward the end of the therapy, Mr. S. reported that he had felt a sense of contentment for the first time and his mood was better.”
This 'now-moment' brought the patient unexpectedly back to the present. The repetition of certain activities created moments which allow intersubjective recognition of a shared subjective reality [7]. If something unexpected occurs in this interaction, the initial intersubjective context will be changed.
A new intersubjective state can only emerge when there is a 'moment of meeting' (see also Figure.1) in which all participants properly perceive the 'now moment', recognize and give an authentic answer to this.
The second case report is about a 40 year old patient, Mrs. T, who is treated by a Gestalt-Therapy approach with the diagnosis of histrionic personality disorder.
"From the therapeutic point of view the improvement of the contact to herself, the anchoring of her experience in an accurate perception and improved body awareness are necessary" [8].
Gestalt-Therapy treats people according to humanistic values with focus on acceptance, empathy, creativity, self-development and solidarity [11]. The human being is seen in his totality of physical and mental processes. As a whole organism he stands in interaction and constantly in contact with the environment.
Also Mrs. T experienced a 'now-moment' at the start of therapy which was reinforced and worked through by the therapist during the meeting:
"After Mrs. T didn’t calm down, the therapist set down besides her and put her hand on her back. Result of the intervention was that the patient could calm down and began a reflexive examination of her needs and conflictual relations."
The third vignette shows the diagnostic procedure of a systemic therapy. Referring to this method Mr. U was in treatment for his somatization disorder. Systemic therapy considers the interaction of the patient with his social micro-and macro system as a central part of its approach [10]. By changing the behavior it has an impact on the social environment and vice versa. A well-structured therapeutic relationship can prevent and promote stability. In order to depict the patient’s symptoms in connection with the relations/ social environment tools such as the genogram, resources interview or the system board are used – also to motivate an awareness for psychic processes in the patient (c.f. Fig. 3 for the intra-psychic processes). It is another way to build a secure space to create reflective thinking in the patient and the therapist.
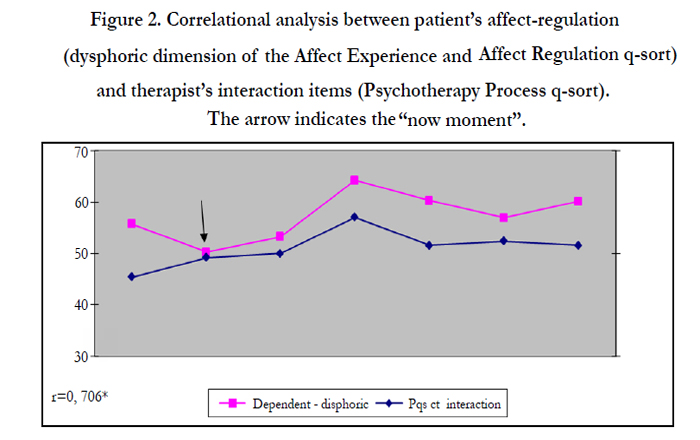
Figure 2. Correlational analysis between patient’s affect-regulation (dysphoric dimension of the Affect Experience and Affect Regulation q-sort) and therapist’s interaction items (Psychotherapy Process q-sort). The arrow indicates the “now moment”.
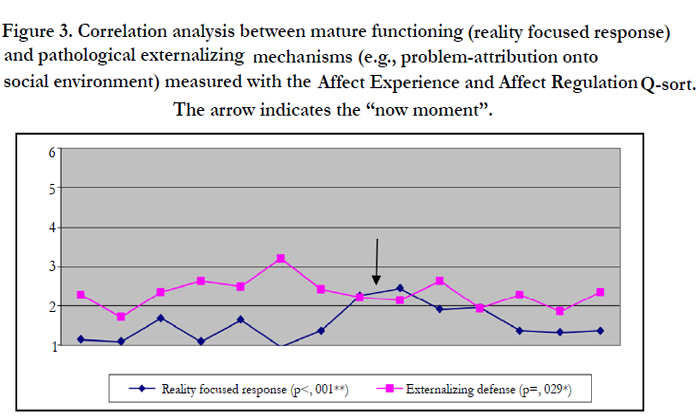
Figure 3. Correlation analysis between mature functioning (reality focused response) and pathological externalizing mechanisms (e.g., problem-attribution onto social environment) measured with the Affect Experience and Affect Regulation Q-sort. The arrow indicates the “now moment”.
Discussion
To be able to intervene successfully as a therapist, the systemic psychotherapy, humanistic therapy and psychoanalysis work similar at the beginning. Further procedure depends more on the nature and severity of the disorder, the chronicity, the reflectivity and the patient's motivation. It is the relationship that allows the therapist to take up the patient’s needs and desires, in order to facilitate a balance between their realization and renunciation [14]. At this juncture there is a disagreement. Both the systemic and the Gestalt-Therapy intervene supportive whereas psychoanalysis acts interpretive. This fact doesn’t have to be necessarily mutually excluded because interpretations are always supportive in the long term. That short-term therapy cannot work with many interpretations is due to the limited time. Consequently other methods must be used which are helpful at least initially such as the body contact in the Gestalt-Therapy case vignette. Most important is the dialogical process in which such “now-moments” can occur and are worked through.
References
- Ablon J. S, Jones E. E (1998) How expert clinicians' prototypes of an ideal treatment correlate with outcome in psychodynamic and cognitive-behavioral therapy. Psychotherapy Research 8(1):71-83.
- Ablon J. S, Jones E. E (2005) On analytic process. Journal of the American Psychoanalytic Association 53(2):541-578.
- Bion W (2002) Zur Unterscheidung von psychotischen und nicht psychotischen Persönlichkeiten. In E. Bott Spillius (Ed.), Melanie Klein heute. Entwicklungen in Theorie und Praxis. 3(1). Stuttgart: Klett- Cotta 75–99
- Bänninger-Huber E (2006) Die Bedeutung der Affekte für die Psychotherapie. In H. Böker (Ed.), Psychoanalyse und Psychiatrie. Geschichte, Krankheitsmodelle und Therapiepraxis. Heidelberg: Springer 301–312
- Doering S, Hörz S (2012) Handbuch der Strukturdiagnostik. Konzepte, Instrumente, Praxis. Stuttgart: Schattauer
- Finger-Ossinger M (2014) Methode-Prozess-Wirksamkeit: Ein Fallbeispiel zur Diagnose „instabile Persönlichkeit”. In Tagungsband der Psychotherapie- Forschungstagung. Wien: Bundesministerium für Gesundheit. pp xx (in press)
- Fonagy P (1998) Moments of change in psychoanalytic theory: Discussion of a new theory of psychic change. Infant Mental Health Journal 19(3):346–353
- Grillmeier-Rehder U (2014) Der Einsatz gezielter Körperwahrnehmung zur Förderung der Selbstunterstützung in der gestalttherapeutischen Einzelpsychotherapie. In Tagungsband der Psychotherapie-Forschungstagung. Wien: Bundesministerium für Gesundheit. pp xx (in press)
- Hartmann-Kottek L (2000) Gestalttherapie. Heidelberg: Springer 177-233
- Hand I (2008) Strategisch-systemische Aspekte der Verhaltenstherapie. Eine praxisbezogene Systematik in ihren historisch-autobiografischen Bezügen. Wien: Springer ISBN: 978-3-211-25219-2 (Print) 978-3-211-69367-4 (Online)
- Ter Horst W, Hartmann-Kottek L (2008): Relationale Gestalttherapie– Beziehung als Essenz. In: Hartmann-Kottek, L (Hrsg) Gestalttherapie. Springer, Heidelberg, S 287–289
- Janssen L, Joraschky P, Tress W (2009) Leitfaden Psychosomatische Medizin und Psychotherapie (2. Auflage). Köln: Deutscher Ärzte-Verlag
- Jones, E. E. (1985). Manual for the Psychotherapy Q Sort. Unpublished manuscript, University of California, Berkeley.
- Kächele H (2006) Psychotherapeut/Psychotherapeutin Person-Persönlichkeit- Funktion. Psychotherapie 11(2):136–140
- Löffler-Stastka H, Blueml V, Boes C (2010) Exploration of personality factors and teir predictive impact an therapy utilization: The externaliziation mode of functioning. Psychotherapy Research 20(3):295–308
- Löffler-Stastka Henriette, Stigler Katharina (2011) Der Affektwahrnehmung und Affektregulation Q-sort-Test (AREQ): Validierung und Kurzform. Psychotherapie Psychosomatik Medizinische Psychologie 61:225-232.
- Reimer C, Rüger U (2006) Psychodynamische Psychothrerapien. Berlin: Springer Medizin ISBN: 978-3-540-25384-6 (Print) 978-3-540-34272-4 (Online)
- Rieken B, Sindelar B, Stephenson T (2011) Psychoanalytische Individualpsychologie in Theorie und Praxis. Psychotherapie, Pädagogik, Gesellschaft. Wien: Springer
- Rudolf G, Rüger U (2012) Psychodynamische Therapieverfahren: Welche nichtpsychodynamischen Ansätze lassen sich integrieren. In Reimer, C & Rüger, U (Hrgs.) Psychodynamische Psychotherapieverfahren. Berlin: Springer Medizin 25-34
- Senf W, Broda M, Wilms B (2012) Therapeutische Beziehung. In W. Senf & M. Broda (Eds.), Praxis der Psychotherapie. Ein integratives Lehrbuch. (5 Auflage). Stuttgart: Georg Thieme Verlag 105- 109
- Stern D, Bruschweiler-Stern N, Harrison A, Lyons-Ruth K, Morgan A, et al. (2001). Die Rolle des impliziten Wissens bei der therapeutischen Veränderung. Einige Auswirkungen entwicklungspsychologischer Beobachtungen für die psychotherapeutische Behandlung Erwachsener. Psychotherapie, Psychosomatik, Medizinische Psychologie 51(3-4):147–152
- Stern D, Sander L, Nahum J, Harrison A, Lyons-Ruth K, et al. (1998) Noninterpretive mechanisms in psychoanalytic therapy: The “something more” than interpretation. International Journal of Psycho-Analysis 79:903–921
- Thomä H, Kächele H (2006) Psychoanalytische Therapie. Grundlagen (3. Auflage.). Heidelberg: Springer Medizin Verlag





