Epilepsy in Kashmir, J&K Childhood Seizures & Epilepsy, Types, Causes, Diagnosis, Intervention, Prevalence and Action
Ganaie,S.A1*, Aadil Bashir2
1 Research Assistant & Rehabilitation Psychologist, Department of Social Work,University of Kashmir, Hazratbal, Jammu and Kashmir,India.
2 Associate Professor, Department of Social Work,University of Kashmir, Hazratbal, Jammu and Kashmir, India.
*Corresponding Author
Showkat Ganaie,
Research Assistant & Rehabilitation Psychologist,
Department of Social Work,University of Kashmir,
Hazratbal, Jammu and Kashmir,India.
E-mail: rcirehabilitationpsychologist@gmail.com
Accepted: April 24, 2014; Published: April 26, 2014
Citation: Ganaie SA, Bashir A. (2014). Epilepsy in Kashmir, J&K: Childhood Seizures & Epilepsy, Types, Causes, Diagnosis, Intervention, Prevalence and Action, Int J Translation Community Dis, 02(02), 13-20. doi: dx.doi.org/10.19070/2333-8385-140003.
Copyright: Ganaie, S.A© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited
Abstract
An epileptic seizure is a transient occurrence of signs and or symptoms due to abnormal excessive or synchronous neuronal activity in the brain. Epilepsy is a disorder of the brain characterized by an enduring predisposition to generate epileptic seizures and by the neurobiological, cognitive, psychological, and social consequences of this condition. The definition of epilepsy requires the occurrence of at least one epileptic seizure (ILAE & IBE 2005). Epilepsy is a physical condition that occurs when there is a sudden, brief change in how the brain works. When brain cells are not working properly, a person's consciousness, movement, or actions may be altered for a short time. These physical changes are called epileptic seizures. Epilepsy is therefore sometimes called a seizure disorder. Epilepsy affects people in all nations and of all races (Epilepsy Foundation of America). The peak stages for the occurrence of epileptic disorders are Childhood and late adulthood as seen in developed countries but it has not been documented properly. The main causes are head injuries, cerebrovascular disease, CNS infections, and birth trauma. Availability of epilepsy-care depends largely on economic factors. Imaging and neurophysiological facilities are available in most countries, but often only in urban centres. Costly drugs, a large treatment gap, limited epilepsy surgery, and negative public attitude to epilepsy are other notable features of management in developing countries. An understanding of the psychosocial, cultural, economic, organizational and political factors influencing epilepsy causation, management, and outcome should be of high priority for future investigations. The lifetime prevalence of epilepsy varied among countries from 1.5 to 14.0 per 1000. This wide variation could partly result from the use of different methods and different types of questionnaire. Screening questionnaires were mainly derived from WHO questionnaires. The prevalence of epileptic disorders in India is 5.9 in males and 5.5 in females in the reference year of 1999. The Incidence of epileptic disorders in India is 60 out of 100,000 in the reference year of 199.
2.Introducation
3.Types of EPILEPSY & Seizures
3.1.Generalized seizures
3.2.Partial Seizure
4.Causes of Epilepsy
4.1.Head injury
4.2.CNS infections
4.3.Genetic factors
4.4.Other Causes
5.Diagnosis Criteria
5.1.A brain scan
5.2.EEG
5.3.Blood tests
6.Intervention Techniques
6.1.Medication
6.2.Surgery
6.3.Vagal nerve stimulation
6.4.The ketogenic diet
6.5.Complementary therapies
7.Epilepsy no longer present
8.Incidence
9.National prevalence of epileptic seizures & Disorders
10.Prevalence of Seizures & Epileptic Disorders in Jammu & Kashmir, India
11.Action against seizures and epileptic disorders in India
12.Epilepsy control program through a district model
13.Structure of health care–delivery system
14.Conclusion
15. Acknowledgements
16.References
Keywords
Seizure; Epileptic Disorder; Childhood Epilepsy; Types; Causes; Diagnosis; Intervention; Prevalence & Action.
Introduction
An epileptic seizure is a transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain (ILAE– 2005). A seizure is the physical findings or changes in behavior that occur after an episode of abnormal electrical activity in the brain. The term "seizure" is often used interchangeably with "convulsion." Convulsions are when a person's body shakes rapidly and uncontrollably. During convulsions, the person's muscles contract and relax repeatedly. There are many different types of seizures. Some have mild symptoms and nobody shaking. The nature of seizures varies because the lobes of the brain control different behaviors, movements and experiences.
Epilepsy is a disorder of the brain characterized by an enduring predisposition to generate epileptic seizures, and by the neurobiological, cognitive, psychological, and social consequences of this condition (ILAE– 2005). Epilepsy comes from a Greek word meaning "to hold or seize," and people who have epilepsy have seizures. People might also hear a seizure called a convulsion, fit, or spell. Seizures happen when there is unusual electrical activity in the brain. WHO estimates that 8 people per1000 worldwide have this disease. Over half of the 50 million people with epilepsy worldwide are estimated to live in Asia. Although much research is done in Asia, information about the recognition of the burden created by the disease is scarce.
Epilepsy is a condition of the brain, not a mental illness. It has been estimated that 2.4 million new cases occur each year globally. Around the world an estimated 50 million people have epilepsy at any given time. Epilepsy is diagnosed when the seizures are unprovoked and recurrent – in other words they happen more than once. It is commonly thought that epilepsy always involves convulsions. In fact there are around 40 different types of epilepsy & epileptic syndromes. Incidence of epilepsy in developing countries is almost double that of developed countries. Up to 70% of people gain full seizure control with treatment but in developing countries, over 80% of people with epilepsy may not receive the treatment they need. A small percentage of people may be eligible for surgery. Approximately 70% of people who have epilepsy surgery become seizure free. Up to 15% of people referred to an epilepsy specialist centre do not actually have epilepsy and have been previously misdiagnosed. Many people outgrow or have a long term remission from seizures.
Conceptually, epilepsy exists where there is a high risk for recurring unprovoked seizures. A commonly used operational definition employed for epidemiological purposes has considered epilepsy to be present after two unprovoked seizures occurring at least 24 hours apart (Hauser et al., 1991). After two unprovoked non-febrile seizures, the chance of having another is 73% (Hauser et al., 1998) at four years (95% CI is 59%-87%), versus 40-52% after a single unprovoked seizure (Berg & Shinnar, 1991).
The “two unprovoked seizure” definition of epilepsy has served well, but it is inadequate in some clinical circumstances. A patient might present with a single unprovoked seizure after a remote brain insult, such as a stroke, CNS infection or trauma. A patient with such brain insults has a risk of a second unprovoked seizure that is comparable to the risk for further seizures after two unprovoked seizures (Hesdorffer et al., 2009). The term “unprovoked” implies absence of a temporary or reversible factor lowering the threshold and producing a seizure at that point in time. Unprovoked is however an imprecise term because we can never be sure that there was no provocative factor. The term "provoked seizure" can be considered as being synonymous with a "reactive seizure" or an "acute symptomatic seizure" (Beghi et al. 2010). The concepts of “unprovoked” and “provoked” therefore, do not clearly distinguish epileptic from reactive seizures, they merely inform the likelihood of one diagnosis or the other.
Types of EPILEPSY & Seizures
Seizures are divided into two main types-Generalized and Partial.There are also some uncommon types of seizures. However,some clients have different types of seizures at different times.
These occur if the abnormal electrical activity affects all or most of the brain. The symptoms tend to be general and involve much of client’s body.
A tonic-clonic seizure is the most common type of generalized seizure. With this type of seizure the client’s whole body stiffens, loses consciousness and then shakes body (convulses) due to uncontrollable muscle contractions. Absence seizure is another type of generalized seizure. With this type of seizure the client will have a brief loss of consciousness or awareness. There is no convulsion, client can’t not fall over, and it usually lasts only seconds. Absence seizures mainly occur in children. A myoclonic seizure is caused by a sudden contraction of the muscles, which causes a jerk. These can affect the whole body but often occur in just one or both arms. A tonic seizure causes a brief loss of consciousness, and client’s body may become stiff and fall to the ground. An atonic seizure causes client to become limp and to collapse, often
with only a brief loss of consciousness.
Sometimes called a grand mal seizure, a tonic-clonic seizure is a more violent type of seizure that often involves the whole body. Often preceded by an aura, this type of seizure typically causes the person to become unconscious or faint and may last up to five minutes. People may lose control of their bowels or bladder, stop breathing and begin biting their tongues or cheeks. Contractions of the muscles are common so the person may appear very stiff (Diana Rodriguez 2009).
Partial seizures are also called focal seizures. In these types of seizures the burst of electrical activity starts in, and stays in, one part of the brain. Therefore, client tends to have localized (focal) symptoms. Different parts of the brain control different functions and so symptoms depend on which part of the brain is affected:
Also called a focal seizure, partial seizures can have a variety of symptoms depending on where in the brain they occur and how severe the seizure is. Like a tonic-clonic seizure, muscles may alternately contract and relax. A partial seizure typically affects only one side of the body, but will often cause unusual movements and motion of the head. Repetitive behaviors such as swallowing, chewing, smacking the lips, moving the mouth or picking at something may also occur. Other characteristics include sweating, nausea, stomach ache, rapid heartbeat and hallucinations (Diana Rodriguez 2009). In Simple partial seizures client may have muscular jerks or strange sensations in one arm or leg. Client may develop an odd taste, or pins and needles in one part of body. Client will not lose consciousness or awareness. Complex partial seizures commonly arise from a temporal lobe (a part of the brain) but may start in any part of the brain. Therefore, this type is sometimes called temporal lobe epilepsy. Depending on the part of the brain affected, client may behave strangely for a few seconds or minutes. For example, client may fiddle with an object, or mumble, or wander aimlessly. In addition, client may have odd emotions, fears, feelings, visions, or sensations. Sometimes a partial seizure develops into a generalized seizure. This is called a secondary generalized seizure
Petit mal seizures generally last just a couple of seconds according to the U.S. National Library of Medicine. They're often defined by the person becoming "absent" for a few seconds. The person's speech or movement may be suddenly interrupted and then continues as before. The person may stare or seem blank or unaware, begin chewing or smacking his lips. She/he may also become strangely still. As soon as the seizure has passed, the person is back to normal with no confusion or memory of what just happened. A petit mal seizure does not cause convulsions or loss of consciousness (Diana Rodriguez 2009).
Causes of Epilepsy
There are very few studies on the causes of epilepsy in Asian populations, and there are particularly few case–control studies or cohort studies. From the available literature, causes seem to be dominated by head injury, birth trauma, and intracranial infections, such as neurocysticercosis or meningoencephalitis. Where socioeconomic development is better, head trauma and stroke are the leading causes of epilepsy. In China in the 1980s, brain injury, intracranial infection, and cerebro-vascular disease, in that order, were the leading putative causes of epilepsy. Cases reported from China during 1994–2003 allowed the estimation of an average incidence of 8.7% for epilepsy with cerebrovascular disease and of 8% with posttraumatic epilepsy. In patients in Hong Kong, the commonest causes were cerebrovascular disease (26.2%), a history of CNS infection (26.0%), head trauma (11.4%), perinatal insult (9.7%), congenital brain malformation (7.4%), hippocampal sclerosis (5.9%), and intracranial neoplasm (5.6%). By contrast, in 300 incident cases of epilepsy in Nepal 47% were caused by neurocysticercosis, 9% by tumor, 4% by vascular disease, and 2% by head injury. In this section, we elaborate on these causes of epilepsy in Asia.
In Asia, post-traumatic epilepsy is one of the most common complications of head injury. One study claimed that post-traumatic epilepsy accounted for 5% of total epilepsy and 20% of symptomatic epilepsy.60 A history of major brain trauma (20.9%) was also the leading cause of epilepsy in surgically treated patients in China.
In developing countries of the world, such as sub-Saharan Africa or Latin America, CNS infections seem to explain the high prevalence of epilepsy. The Commission on Tropical Disease of the International League against Epilepsy listed several diseases as causes of epilepsy, including malaria, tuberculosis, schistosomiasis, AIDS and cysticercosis. In Asia, there is a lack of rigorous analytical studies to assess the effect of these infections in epilepsy. An association between neurocysticercosis and epilepsy was found in numerous studies in Africa and Latin America. Neurocysticercosis was the cause of epilepsy in about 50% of cases.
An association between neurocysticercosis and epilepsy was found in numerous studies in Africa and Latin America. Neurocysticercosis was the cause of epilepsy in about 50% of patients in some studies and seizures occur in 50–80% of patients with parenchymal cysticercosis. In Asia, many studies report the presence of cysticercosis (taeniasis). However, there are few studies on the relation between neurocysticercosis and epilepsy in Asia, and their results vary widely. Neurocysticercosis is probably an important cause of seizures and epilepsy in regions with a high prevalence of Taenia solium infection in human beings.
In Asia, this includes India, Nepal, Bali, Papua and Sulawesi in Indonesia, and parts of Vietnam and China. Cysticercosis is only rarely detected in the most economically advanced countries of Asia, such as South Korea but the prevalence might also be low in poor regions. In a meta-analysis, seizures were the most common symptom (56.2%) of cysticercosis in China. Another study noted that between 8.7% and 50.0% of cysticercosis-infected patients had recent seizures. Single CT enhancing lesions and neurocysticercosis together accounted for 67% of the provoking factors of acute symptomatic seizures. Conversely, in some studies, the cysticercosis positivity was not higher in patients with epilepsy in regions with either a low prevalence (e.g., Laos) or a high prevalence (e.g., Indonesia).
Paragonimiasis is endemic in several Asian countries: China, South Korea, the Philippines, Japan, and Vietnam. During migration, the causal lung fluke may reach the brain and may cause seizures, epilepsy, and other neurological syndromes. However, no study has quantified the importance of Paragonimus infection in epilepsy.
Malaria is still widely endemic in Asia, with more than 3 million cases per year. India, Burma, Indonesia, Pakistan, Cambodia, Papua New Guinea, and Bangladesh each have more than 50 000 cases per year. Malaria causes various symptoms, such as fever and convulsions. 7.7% of patients with childhood malaria (with or without the presence of cerebral malaria) in a retrospective survey in Thailand had convulsions. In cerebral malaria, convulsions present in 60% of cases. However, we did not find any analytical study reporting the relation between malaria and epilepsy in Asia. Nevertheless, the link between epilepsy and malaria was recently supported by a case–control study in Gabon and a cohort study in Mali in Africa.
Japanese encephalitis is one of the most common encephalitic disorders worldwide. Most of China, Southeast Asia, and the Indian subcontinent are affected. 65% of patients with Japanese
Encephalitis has acute symptomatic seizures and 13% have chronic epilepsy. In a study in India, 30 of 65 patients with Japanese encephalitis had seizures in the first weeks of illness; 19 of them had two or more seizures.
Two studies in India found no relation between being a twin and epilepsy, and twins of people with epilepsy did not have a high risk of epilepsy. Case–control studies in China have found no relation between epilepsy and susceptibility genes, such as GABABR1, KHDRBS3 (T-STAR), and CACNA1G (calcium channel, voltage dependent, T-type, alpha 1G subunit). However,numerous studies have confirmed familial history of epilepsy and parental consanguinity as risk factors. In Kerala, south India, a family history of epilepsy was three times more common in patients with epilepsy than in controls (or 3.2, 95% CI 2.1–4.7) and two times higher in another study in north India (2.1, 1.1–4.3). Family history was also a risk factor for epilepsy in studies in Laos and China. This level of risk is similar to that in studies from Africa. In Asia, consanguineous marriage is common in certain cultures, in particular among Indian and Muslim populations. Consanguinity of parents was significantly more common among patients than among controls (13.1% vs 6.6%).The odds ratio for parental consanguinity was higher in patients with generalized epilepsy than for controls (2.6; 95% CI 1.5–4.4). Another study of 316 patients with epilepsy of Indian origin in Malaysia showed that 29.5% of them had a parental consanguineous marriage, and that there was a significant association with parental consanguinity in idiopathic and cryptogenic epilepsies. Consanguinity could be a target for a campaign to prevent epilepsy.
Seizures of all types are caused by disorganized and sudden electrical activity in the brain. Some causes like Abnormal levels of sodium or glucose in the blood, Brain infections including meningitis, Brain injury that occurs to the baby during labor or childbirth, Brain problems that occur before birth (congenital brain defects), Brain tumor (rare), Choking, Drug abuse, Electric shock, Fever (particularly in young children), Head injury, Heart diseases, Heat illness (see heat intolerance), High fever, Illicit drugs, such as angel dust (PCP), cocaine, amphetamines, Kidney or liver failure, Low blood sugar, Phenylketonuria (PKU), which can cause seizures in infants, Poisoning, Stroke, Toxemia of pregnancy, Uremia related to kidney failure, Very high blood pressure (malignant hypertension), Venomous bites and stings (see snake bite), Withdrawal from alcohol after drinking a lot on most days, Withdrawal from certain drugs, including some painkillers and sleeping pills and Withdrawal from benzodiazepines (such as Valium) can lead to epileptic disorder.
Sometimes no cause can be identified. This is called idiopathic seizures. They usually are seen in children and young adults but can occur at any age. There may be a family history of epilepsy or seizures.
Diagnosis Criteria
For diagnosis of Seizures and Epilepsy it is always better to consult a medical doctor. Sometimes it is very difficult for a doctor to confirm that the client had a seizure. The most important part of confirming the diagnosis is the description of what has happened. Other conditions can look like seizures also - for example, faints, panic attacks, collapses due to heart problems, breath-holding attacks in children. Therefore, it is important that a doctor should have a clear description of what happened during the event. It may be that a person who witnessed client’s seizure may be able to give a more accurate description of what happened during seizure.
There is no one test to confirm a diagnosis of epilepsy. However,tests such as brain scans, electroencephalogram (EEG - brainwave recordings) and blood tests may help to make a diagnosis.
Usually a magnetic resonance imaging (MRI) or computed tomography (CT) scan - shows the structure of different parts of the brain. This may be performed in some people.
This test records the electrical activity of the brain. Special stickers are placed on various parts of the scalp. They are connected to the EEG machine. This amplifies the tiny electrical messages given off by the brain and records their pattern on paper or computer. The test is painless. Some types of seizure produce typical EEG patterns. However, a normal recording does not rule out epilepsy, and not all EEG abnormalities are related to epilepsy.
Blood tests and other tests may be advised to check on client’s general well-being. They may also look for other possible causes of the event.
However, tests may help to decide if the event was a seizure, or caused by something else. It is unusual for a diagnosis of epilepsy to be made after one seizure, as the definition of epilepsy is recurrent seizures. For this reason a doctor may suggest to wait and see if it happens again before making a firm diagnosis of epilepsy.
Intervention Techniques
Epilepsy cannot be cured with medication. However, with the right type and strength of medication, the majority of client’s with epilepsy do not have seizures. The medicines work by stabilizing the electrical activity of the brain. Client need to take medication every day to prevent seizures. Deciding on which medicine to prescribe depends on such things as: type of epilepsy, age, and other medicines that client may take for other conditions, possible sideeffects. One medicine can prevent seizures in most cases. A low dose is usually started at first. The dose may be increased if this fails to prevent seizures. In some cases two medicines are needed to prevent seizures. The decision when to start medication may be difficult. A first seizure may not mean that client have epilepsy, as a second seizure may never happen, or may occur years later. The decision to start medication should be made by weighing up all the pros and cons of starting, or not starting, the medicine. It is unusual to start treatment after a first seizure. A common option is to wait and see after a first seizure. If client have a second seizure within a few months, more are likely. Medication is commonly started after a second seizure that occurs within 12 months of the first. However, there are no definite rules and the decision to start medication should be made after a full discussion with client’s doctor. The type of treatment client will be given often depends on the type of seizures client had and also if client are taking any other medication.
Surgery to remove a small part of the brain which is the underlying cause of the epilepsy. This is only a suitable option if seizures start in one small area of brain (this means it is only possible for a minority of persons with epilepsy). It may be considered when medication fails to prevent seizures. However, there are risks from operations. Only a small number of persons with epilepsy are suitable for surgery and, even for those who are, there are no guarantees of success. Surgical techniques continue to improve and surgery may become an option for more and more people in the future.
Vagal nerve stimulation is a treatment for epilepsy, where a small generator is implanted under the skin below the left collar bone. The vagus nerve is stimulated to reduce the frequency and intensity of seizures. This can be suitable for some persons with seizures that are difficult to control with medication.
The ketogenic diet is a diet very high in fat, low in protein and almost carbohydrate-free which can be effective in the treatment of difficult-to-control seizures in children.
The ketogenic diet is a diet very high in fat, low in protein and almost carbohydrate-free which can be effective in the treatment of difficult-to-control seizures in children.
Complementary therapies such as aromatherapy may help with relaxation and relieve stress, but have no proven effect on preventing seizures.
The below mentioned diagram shows how integrated approach can help to control seizures and epileptics disorders.
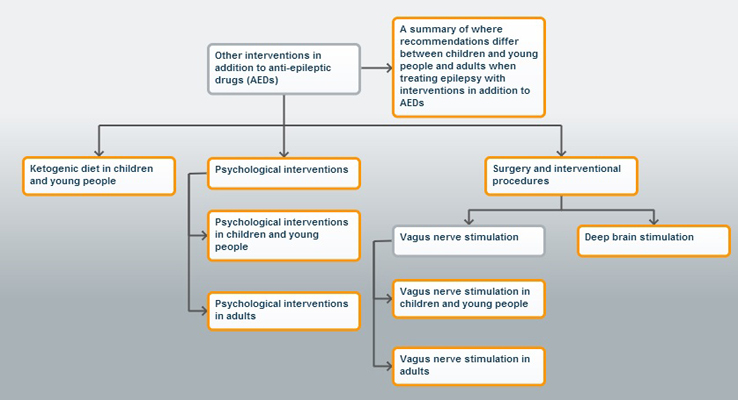
Figure
Epilepsy no longer present
Children can outgrow their epilepsy, as with benign epilepsy with centro-temporal spikes (BECTS). Some persons might have had a treatment, such as brain surgery, rendering them permanently seizure-free. Medical literature uses the term "remission" to imply an abeyance of a disease and "cure" to imply its disappearance, i.e., a chance of recurrence no greater than for the general population. Structural brain lesions, such as malformations of cortical development (Rowland et al., 2012), may elevate risk for seizures long-term. Seizures may recur at variable intervals after remission due to removal of an epileptogenic lesion, such as a cavernous malformation (Kim et al., 2011). Recurrence risk depends upon the type of epilepsy, age, syndrome, etiology, treatment and many other factors. Juvenile myoclonic epilepsy is known to be subject to lifelong elevated risk for seizures (Geithner et al., 2012). Structural brain lesions, such as malformations of cortical development (Rowland et al., 2012), may elevate risk for seizures longterm. The risk of seizure recurrence after unprovoked seizures diminishes with time, although it may never reach risk levels for normal individuals who have not had a prior seizure. Most relapses are early. After a single unprovoked seizure, 80% (Hart et al., 1990; Neligan et al., 2012) to 90% (Lindsten et al., 2001) of those who had a second did so within two years. In one study (Hauser et al., 1998), after a second unprovoked seizure, subsequent seizures occurred within 4 years, but none in the ensuing 3 years, suggesting that the risk may not be zero but are low. Few data are available on seizure recurrence risk after being seizure-free and off medication for extended periods of time. Delayed relapses do occur, but they are rare after 5 years (Lossius et al., 2008). By 10 years off anti-seizure medicines, the annual risk for seizures probably is very low (Chadwick et al., 1996).
Incidence
The incidence of epileptic disorders in India is higher, and reached 60.0 per 100 000 persons. Overall, the results were not different from those in developed countries where the age-adjusted incidence of epilepsy is 24–53 per 100 000 persons. Some authors report an incidence rate in developing countries that is as high as 190 per 100 000 person.
National prevalence of epileptic seizures & Disorders
The prevalence of epileptic disorders in India is 3.91 (1998), 5.0 (2002) 5.6 (2003) and 3.81 (2006). The usual "prevalence" rate (number of persons with epilepsy during a specified time) is 500- 1000 cases per 100,000 persons in the population. Going by these statistics, there will be about 2,600 – 6,500 new cases of epilepsy every year in Delhi and New Delhi alone (estimated population of 1.3 crores) and 200,000 to 500,000 new cases in the whole of India (estimated population about 100 crores). Similarly at the present time there may be approximately 65,000-130,000 persons with epilepsy in Delhi/New Delhi and about 50-100 lakhs in whole of India respectively.
A door-to-door survey was carried out to screen a community of 14,010 people (Parsis living in colonies in Bombay, India) for possible neurologic diseases. High school graduates, social workers, and medical students administered a screening questionnaire that in a pilot survey had a sensitivity of 100% for identifying persons with epilepsy. Neurologists used defined diagnostic criteria to evaluate individual’s positive on the screening survey. Sixty-six persons (43 males, 23 females) suffered from epilepsy (4.7 cases/1,000). Of those, 50 (34 males, 16 females) had active epilepsy (3.6 cases/1,000). The age-specific prevalence ratios remained fairly constant for each age group except for a small peak in the group aged 20-39 years for all epilepsy cases combined. Age-adjusted prevalence ratios were higher for males. The most common seizure type was partial (36 cases). The most frequently associated conditions were cerebral palsy and mental retardation. The majority of individuals were receiving medication as of prevalence day (47 cases) (Bharucha NE, Bharucha EP, Bharucha AE, et al. 1988, March-April).
Prevalence of Seizures & Epileptic Disorders in Jammu & Kashmir, India
The rural population of 63,645 living in the mountainous Kuthar Valley of South Kashmir, Northwest India was surveyed to determine the prevalence of major neurologic disorders, including epilepsy (called Lath/Mirgi/Laran in the local language). House to House survey was done by anganwardi workers to indentify people with possible epilepsy. The screening questionnaire was translated into local vernacular. Persons who had some indication of a history of seizures or other neurologic disease were subsequently examined by a neurologic team. One hundred fifty-seven cases of active epilepsy were detected, giving a crude prevalence rate of 2.47/1,000 general population. In those aged less than 14 years, prevalence was 3.18/1,000. Ninety-five (60.5%) of all cases were male; 91% of active epilepsy cases had onset of seizures before age 30 years. Mean age of onset in males was 5.3 years, and in females it was 7.1 years. Mean duration of seizures was 6 years; 78.9% cases had generalized seizures, 74.5% cases were receiving no specific treatment, 99.4% cases were born of home delivery, and 8.9% cases had a positive family history of seizures. Mental retardation was the most common associated abnormality in 22.9% of cases (Koul R, Razdan S, Motta A. 1988 March-April).
Recently a house to house survey has been conducted in district Kupwara for the identification of Children with Seizures & epileptic Disorders between the age group of 3 to 14 years (Ganaie S & Bashir A, 2014 Feb-March). The multi-stage cluster sampling procedure has been followed to gather research data. In 1st stage 50% of tehsils has been selected, 2nd stage 50% of blocks has been selected, 3rd stage 20% of villages (51) have been selected out of already selected 50% of blocks. The villages have been selected from both rural and urban areas of district Kupwara. Finally the randomized sample of 31children got screened for seizures and epileptic disorders. Diagnostic criteria proposed by the International League against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE) (2005) have been followed to differentiate between seizure and epileptic disorders. The total number of children screened was 1581. The informants were 1410 mothers (89.2%), 74 fathers (4.68%) and 97 significant others like grandparents & caregivers (6.13%). The total number of children who had seizure once in life till the date of screening were 107 (6.76%) and the total number of children who had seizures more than two times were 146 (9.23%). The study will be published soon with detailed descriptions.
The following practical points need to be remembered
1. One in 20 persons will have an epileptic seizure at some point in their lives.
2. One in 100-200 persons in general population has epilepsy at any given time.
3. About 50–70% clients will develop epilepsy (have their first seizure) before the age of 18 years.
Action against seizures and epileptic disorders in India
The stalwarts in the neurological arena in India realized in late 1960's, that a separate section concentrating on various aspects of epilepsy is needed. The aims and objective of such a society had to go beyond the charter of the Neurological Society of India (NSI). Dr. Anil D Desai was designated Secretary of Epilepsy section within NSI and in the period 1968 – 1969. Anil D Desai was designated Secretary of Epilepsy section within NSI and in the period 1968 - 1969, he along with Dr. Eddie P.Bharucha and Dr.Noshir H Wadia went about in a missionary zeal to form a new society. The new society was named Indian Epilepsy Association (IEA). A new constitution for IEA was formulated incorporating the essential objectives, and rules under the Societies Registration Act XXI of 1860.
Epilepsy Foundation of India (EFI) is a non-profitable charitable organization working for the cause of persons suffering from epilepsy. Epilepsy Foundation dedicated solely to the welfare of the millions of people with epilepsy in the India and their families. The organization works to ensure that persons with seizures are able to participate in all life experiences to improve how persons with epilepsy are perceived, accepted and valued in society and to promote research for a cure. The Epilepsy Foundation of India (EFI) was established in 2009. Free Epilepsy Clinic has been started in 1992 with the aim of helping the poor and needy patients, suffering from epilepsy and not able to consult a doctor for a regular therapy. The aim was to ensure the patient see the doctor irrespective if their financial conditions regularly and get the free medication if they cannot afford it. From 2000 onwards Free Epilepsy Clinic has moved to Surya Neuro Center every Tuesday at 1 p.m.
An Indian programme, established by the National Institute of Mental Health and Neurosciences in Bangalore, provides an interesting approach that attempts to circumvent many of the anticipated problems of treatment programmes in developing countries. A national workshop on public health aspects of epilepsy estimated that around 10 million people with epilepsy were living in India (a prevalence rate of 1 in 100 people).
Epilepsy control program through a district model
Epilepsy Control Programme in India through a District Model developed by NIMHANS was supported by WHO through the Ministry of Health, Government of India, during 1999 to 2001.
The program envisaged three objectives:
(a) to sensitize state health administrators to public health aspects of epilepsy;
(b) to train district medical officers for delivery of epilepsy care and also function as “trainer” for PHC doctors; and
(c) to enlist “nodal neurologists” from different states to support and ensure the sustainability of the program.
Other Institutions are also working for the persons with epileptic seizures and disorders like National Institute for the Mentally Handicapped (NIMH), All India Institute for Medical Sciences (AIIMS), PGI Chandigarh etc.
In Jammu & Kashmir, the Institutions working for the persons with Seizures and Epileptic Disorders are like SKIMS, JVC, GMC Srinagar, Children’s Hospital, SMHS, IMHANS, Psychiatric Hospital Jammu, GMC Jammu, Children’s Hospital Jammu, All District Hospitals and PHCs.
Structure of health care–delivery system
India has a population of 1.02 billion spread over 593 districts in 29 states and six union territories, with an urban population of 28% and a rural population of 72% (19). Primary and secondary health care in the government sector is delivered through a vast network of 136,815 sub centers (SCs; one SC for 5,000 population manned by health workers), 22,962 primary health centers (PHCs; one PHC for 30,000–50,000 population), 2,708 taluk hospitals/ community health centers (CHCs; one CHC for 100,000 population) under the administrative control of 593 district hospitals (DHs; one DH for 1.5–2 million population) (20). Tertiary care is provided by hospitals of medical colleges, apex institutions, and specialized centers. Government health services are free/ highly subsidized for the poor and needy. A rapidly emerging private health sector, in the absence of health insurance, is affordable to only a small section of the population. Traditional systems of medicine also are widely used in the country.
Conclusion
Anyone can be affected by seizures at any age, but epilepsy is most frequently diagnosed in infancy, childhood, adolescence and old age. Epilepsy is the world's most common serious brain disorder (WHO). Epilepsy is more than three times as common as multiple sclerosis, Parkinson’s disease and cerebral palsy. Epilepsy is not necessarily a lifelong disorder. Epilepsy can have profound social, physical and psychological consequences. People with epilepsy can face social stigma and exclusion. A fundamental part of reducing this stigma is to raise public and professional awareness. Epilepsy is associated with an increased risk of death which may be related to an underlying brain disease, such as a brain tumor or infection, seizures in dangerous circumstances leading to drowning burns or head injury, prolonged or ongoing seizures, sudden & unexplained causes, a possible respiratory or cardio-respiratory arrest during a seizure and suicide. It is suggested that there is a need for a decentralized model of epilepsy care at the district level, with the district medical officer being the core person to the program, a neurologist functioning as a nodal person, and the primary health center medical officer as the delivery agent. Policy-level initiatives are required at this juncture to expand and sustain this program by health administrators and professionals. It is hoped that the “unreached” will be reached through such a strategy.
Acknowledgements
We thank to Research Assistant Ms. Tamanaah, Mr. Zahoor Ganie, Mr. Khursheed Ganie and Mr. Parveez Ganie
References
- Aziz H, Ali SM, Frances P (1994) Epilepsy in Pakistan: a community based epidemiologic study. Epilepsia; 35: 950–58.
- Berg AT, Shinnar S (1991) The risk of seizure recurrence following a first unprovoked seizure: a quantitative review. Neurology 1991; 41: 965–72.
- Bharucha NE, Bharucha EP, Bharucha AE (1988) Prevalence of epilepsy in the Parsi community of Bombay. Epilepsia; 29: 111–15.
- Bharucha NE, Bharucha EP, Dastur HD (1987) Pilot survey of the prevalence of neurologic disorders in the Parsi community of Bombay. Am J Prev Med; 3:293–9.
- Fisher RS, van Emde Boas W, Blume W, (2005) Epileptic seizures and Epilepsy: definitions proposed by the International League against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia; 46:470–72.
- Fong GCY, Mak W, Cheng TS (2003) A prevalence study of epilepsy in Hong Kong. Hong Kong Med J 2003; 9: 252–57.Bharucha NE. Epidemiology of epilepsy in India. Epilepsia; 44: 9–11.
- Gourie-Devi M, Satishchandra P, Gururaj G (2003) Epilepsy control program in India: a district model. Epilepsia; 44: 58–62.
- Gourie-Devi M, Rao VN, Prakshi R (1987) Neuro-epidemiological study in semiurban and rural areas in south India: Pattern of neurological disorders including motor neuron disease. In: Gourie-Devi M, ed. Motor neuron disease:Global clinical patterns and international Research. New Delhi: Oxford and IBH Publishing Company,:11–21.
- Gourie-Devi M, Gururaj G, Satishchandra P (1996) Neuro-epidemiological pilot survey of an urban population in a developing country: a study in Bangalore, South India. Neuro-epidemiology; 15: 313–20.
- Gourie-Devi M, Gururaj G, Satishchandra P (1995) Neuro-epidemiological survey in urban and rural areas: a prevalence study. New Delhi: Indian Council of Medical Research.
- Gourie-Devi M, Satishchandra P, Gururaj G (1999) Report of national workshop on public health aspects of epilepsy for senior health personnel of state health departments in India. Annals of Indian Academy of Neurology, 2: 43–48.
- Hauser WA, Annegers JF, Kurland LT (1991) Prevalence of epilepsy in Rochester, Minnesota: 1940-1980. Epilepsia 32:429-445.
- Hauser WA, Rich SS, Lee JR, Annegers JF (1998) Risk of recurrent seizures after two unprovoked seizures. N Engl J Med 338:429-434.
- Hesdorffer DC, Benn EK, Cascino GD, Hauser WA (2009) Is a first acute symptomatic seizure epilepsy? Mortality and risk for recurrent seizure. Epilepsia 50:1102-1108.
- Jain S, Padma MV, Puri A ( 2005) Twin birth and epilepsy: an expanded India study. Neurol J Southeast Asia 1999; 4: 19–23. 92 Sharma K. Genetic epidemiology of epilepsy: a twin study. Neurol India; 53: 93–98.
- Kariyawasam SH, Bandara N, Koralagama A (2004) Challenging epilepsy with antiepileptic pharmacotherapy in a tertiary teaching hospital in Sri Lanka. Neurol India; 52: 233–37.
- Krishnan A, Sahariah SU, Kumar Kapoor S (2004) Cost of epilepsy in patients attending a secondary-level hospital in India. Epilepsia; 45: 289–91.
- Kuruvilla A, Pandian JD, Radhakrishnan VV (2001) Neurocysticercosis: a clinical and radiological appraisal from Kerala State, South India. Singapore Med J; 42: 297–303.
- Koul R, Razdan S, Motta A (1988) Prevalence and pattern of epilepsy (Lath/ Mirgi/Laran) in rural Kashmir, India. Epilepsia; 29: 116–22.
- Lim SH (2004) Seizures and epilepsy in the elderly: epidemiology and etiology of seizures and epilepsy in the elderly in Asia. Neurol Asia; 9: 31–32.
- Lu J, Chen Y, Pan H (2003) The gene encoding GABBR1 is not associated with childhood absence epilepsy in the Chinese Han population. Neurosci Lett; 343: 151–54.
- Mani KS, Rangan G, Srinivas HV (1998) The Yelandur study: a community- based approach to epilepsy in rural South India— epidemiological aspects. Seizure; 7: 281–88.
- Mannan MA (2004) Epilepsy in Bangladesh.Neurol Asia; 9: 18.
- Mani KS (1997) Epidemiology of epilepsy in Karnataka, India. Neurosci Today; 1: 167–74.
- Murthy JMK, Vijay S, Ravi Raju C (2004) Acute symptomatic seizures associated with neurocysticercosis: A community-based prevalence study and comprehensive rural epilepsy study in South India. Neurol Asia; 9: 86.
- Muttaqin Z (2006) Surgery for temporal lobe epilepsy in Semarang, Indonesia:the first 56 patients with follow up longer than 12 months. Neurol Asia; 11: 31–36.
- Murthy JM, Yangala R (1999) Acute symptomatic seizures—incidence and etiological spectrum: a hospital-based study from south India. Seizure; 8:162–65.
- Nair RR, Thomas SV (2004) Genetic liability to epilepsy in Kerala State, India. Epilepsy Res; 62: 157–64.
- Panda S, Radhakrishnan K, Sarma PS (2004) Mortality in surgically versus medically treated patients with medically refractory temporal lobe epilepsy. Neurol Asia; 9: 129.
- Radhakrishnan K, Pandian JD, Santhoshkuma T (2000) Prevalence, knowledge, attitude and practice of epilepsy in Kerala, South India. Epilepsia; 41: 1027–35.
- Ray BK, Bhattacharya S, Kundu TN (2002) Epidemiology of epilepsy- Indian perspective. J Indian Med Assoc; 100: 322–26.
- Rajshekhar V, Raghava MV, Prabhakaran V (2006) Active epilepsy as an index of burden of neurocysticercosis in Vellore district, India. Neurology;67: 2135–39.
- Radhakrishnan K, Nayak SD, Kumar SP (1999) Profile of antiepileptic pharmacotherapy in a tertiary referral center in South India: a pharmacoepidemiologic and pharmacoeconomic study. Epilepsia, 40: 179–85.
- Rajshekhar V, Joshi DD, NQ Doanh (2003) Taenia solium taeniosis/ cysticercosis in Asia: epidemiology, impact and issues. Acta Trop; 87: 53–60.
- Rajshekhar V (2004) Epidemiology of Taenia solium taeniasis/cysticercosis in India and Nepal. Southeast Asian J Trop Med Public Health; 35: 247–51.
- Ramasundrum V, Tan CT (2004) Consanguinity and risk of epilepsy. Neurol Asia; 9: 10–11.
- Razdan S, Kaul RL, Motta A (1994) Prevalence and pattern of major neurological disorders in rural Kashmir. Neuro-epidemiology; 13:113–9.
- Ren L, Jin L, Zhang B (2005) Lack of GABABR1 gene variation (G1465A) in a Chinese population with temporal lobe epilepsy. Seizure; 14: 611–13.
- Sawhney IM, Singh A, Kaur P (1999) A case control study and one year follow-up of registered epilepsy cases in a resettlement colony of North India, a developing tropical country. J Neurol Sci; 165: 31–35.
- Schematic representation of district model for epilepsy control program. District Model for Epilepsy Control 61 Epilepsia, Vol. 44, Suppl. 1, 2003
- Seino M (2001) Comprehensive epilepsy care: Contributions from paramedical professionals. Neurol J Southeast Asia; 6: 1–5.
- Singhal BS (1998) Neurology in developing countries: a population perspective. Arch Neurol; 55: 1019–21.
- Sridharan R, Murthy BM (1999) Prevalence and pattern of epilepsy in India. Epilepsia; 40: 631–36.
- Silpakit O, Silpakit C (2003) A Thai version of a health-related quality of life instrument for epilepsy. Neurol J Southeast Asia; 8: 103–07.
- Thomas SV, Koshy S, Nair CR (2005) Frequent seizures and polytherapy can impair quality of life in persons with epilepsy. Neurol India; 53: 46–50.
- Thomas SV, Sarma PS, Alexander M (2001) Economic burden of epilepsy in India: Epilepsia; 42: 1052–60
- Verma A, Misra S (2006) Risk of seizure recurrence after antiepileptic drug withdrawal, an Indian study. Neurol Asia; 11: 19–23.
- Veliath AJ, Ratnakar C, Thakur LC (1985) Cysticercosis in South India. J Trop Med Hyg; 88: 25–29.
- World Health Organization: epilepsy: epidemiology, aetiology and prognosis. WHO Factsheet, 2001: number 165.
- WHO, International Bureau for Epilepsy, International League against Epilepsy. Atlas—epilepsy-care in the world 2005. Geneva: WHO, 2005.
- http://epilepsyfoundationindia.com/?page_id=105 used on 2014/04/06:3:00.p.m.
- www.epilepsy.org.au/resources/formedia/facts-statistics-about-epilepsy used on 2014/04/06:3:15 p.m.
- www.epilepsyindia.org/aboutus_iea.html used on 2014/04/06: 3:30. pm.
- www.who.int/mental_health/neurology/epilepsy/en/ used on 2014/04/06: 3:45.p.m.





