Evolution of Immunosuppressive Agents in Renal Transplantation: An Updated Review
Kumar A, Shrestha BM*
Sheffield Kidney Institute, Sheffield Teaching Hospitals NHS Trust, Herries Road, Sheffield, S5 7AU, UK.
*Corresponding Author
Badri Shrestha,
Sheffield Kidney Institute, Herries Road,
Sheffield, S5 7AU, UK.
Tel: +44 7949354709
Fax: +44 1142714604
Email: shresthabm@doctors.net.uk
Received: February 09, 2016; Accepted: March 11, 2016; Published: March 22, 2016
Citation: Kumar A, Shrestha BM (2016) Evolution of Immunosuppressive Agents in Renal Transplantation: An Updated Review. Int J Stem Cell Res Transplant 04(3), 158-157.DOI : dx.doi.org/10.19070/2328-3548-1600027
Copyright: Shrestha BM© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Suppression of allograft rejection is the central issue in renal transplantation (RT). Thus, development of immunosuppressive agents is the key for successful allograft function. Immunosuppression agents in RT have evolved over the last six decades beginning with total lymphoid irradiation to the currently available immunosuppressive strategies, which have significantly reduced the incidence of acute rejection episodes and improved short-term graft and patient outcomes. However their use is associated with long-term graft dysfunction, hypertension, hyperlipidaemia, diabetes mellitus, infections and malignancies. Chronic antibody-mediated rejection and chronic allograft dysfunction still remain the major problems, often leading to graft loss and shortened long-term graft survival.
Immunosuppressive agents are used for induction, maintenance and reversal of established rejection. The use of multidrug regimen tailored to the immunological risk of patient and adverse-effect profile of the drug provides the optimum outcomes. This review focuses on the evolution of immunosuppression agentsused in RT over last six decades and highlightsthe newer agents under investigation.
2.Introduction
2.1.Literature Search Strategy
2.2.Immunology in Renal Transplantation
2.3.Allorecognition and T cell activation
2.4.B Lymphocytes
2.4.Donor-specific antibodies
3.Immunosuppressive Agents in Renal Transplantation
3.1.Total lymphoid irradiation
3.2.Corticosteroids
3.3.Azathioprine
3.4.Cyclosporine
3.5.Tacrolimus
3.6.Prolonged-release tacrolimus
3.7.Mycophenolate mofetil (MMF)
3.8.mTOR Inhibitors: Sirolimus and Everolimus
3.9.Antibodies
3.10.Rabbit antithymocyte globulin (rATG)
4.Muromonab (OKT3)
5.Interleukin-2 receptor (CD25) monoclonal antibody
6.Alemtuzumab
7.Rituximab
8.Belatacept
9.Bortezomib
7.Eculizumab
8.C1 inhibitor in AMR
9.Agents Investigated in the Past
9.1.FTY-720
9.2.Sotrastaurin
9.3.Tofacitinib
9.4.Generic Formulations
10.Conclusion
11.References
Keywords
Immunosuppressive Agents; Renal Transplantation; Immunology; Rejection; Side-effects; Outcomes.
Introduction
Renal transplantation (RT) is the best modality of renal replacement therapy for most patients with stage-5 chronic kidney disease, as this improves the quality of life, patient survival and is cost-effective[1].Since the first successful RT performed between the identical twins in the Peter Brent Brigham Hospital, Boston on 23rd December 1954 by Murray et al, RT has become a routine[2]. According to the World Health Organisation, in 2013, a total of 78950 kidney transplants were performed in 104 countries worldwide[3]. When a kidney is transplanted from a human leucocyte antigen (HLA) non-identical donor, the recipient mounts an alloimmune response, that leads to T lymphocyte activation, antibody production, complement activation, allograft rejection and transplant failure [4]. Immunosuppressive agents are used to prevent acute cellular and antibody-mediated rejections (AMR), both early and late, which lead to chronic allograft injury (CAI) in long-term. Significant advances have been made in the immunosuppressive strategies over the past three decades to reduce the incidence of allograft rejection and side-effects of the drugs, and to improve long-term graft and patient survivals.Introduction of cyclosporine revolutionised the practice of RT by reducing acute rejection rate and improved the short-term graft survival, which was further improved by tacrolimus, mycophenolate mofetil (MMF) and induction immunosuppressive agents. Despite these advances, there is lack of clear evidence of improvement of longterm graft survival because CAI continues to cause late renal allografts losses[5].
Immunosuppressive agents used in RT are classified into three groups: induction, maintenance and rescue agents (Table 1). Induction agents comprise of polyclonal antibodies (rabbit antithymocyte globulin (rATG)) and interleukin -2 receptor antagonist (IL-2RA) (basiliximab and daclizumab). The anti-CD3 monoclonal antibody (OKT3) is no longer used because of severe adverse side-effects. Newer induction agents include alemtuzumab and rituximab. The maintenance agents comprise of calcineurin inhibitors (CNIs) (cyclosporine and tacrolimus), antiproliferative agents (azathioprine and MMF), mammalian target of rapamycin inhibitors (mTOR-I) (sirolimus and everolimus) and corticosteroids. Three newer maintenance agents include belatacept, a costimulation blocker; sotrastaurin, a protein kinase C inhibitor; and tofacitinib, a JAK 3 inhibitor. Transplant rejection can be acute cellular and acute AMR. Mild cellular rejection can be treated with corticosteroids, whereas moderate and severe acute cellular rejection is typically treated with ATG. AMR is treated with plasmapheresis, intravenous immunoglobulin (IVIg) and rituximab. Refractory AMR is treated with proteasome inhibitor bortezomib and C5 inhibitor, eculizumab.This review will focus on the stepwise evolution of immunosuppressive agents in RT over the last six decades, their safety and efficacy, outcomes of pivotal trials and newer drugs under investigation.It is essential to understand the principles of immunology involved in RT for theinterpretation of the mechanism of action of these drugs, hence a section on immunology is included.
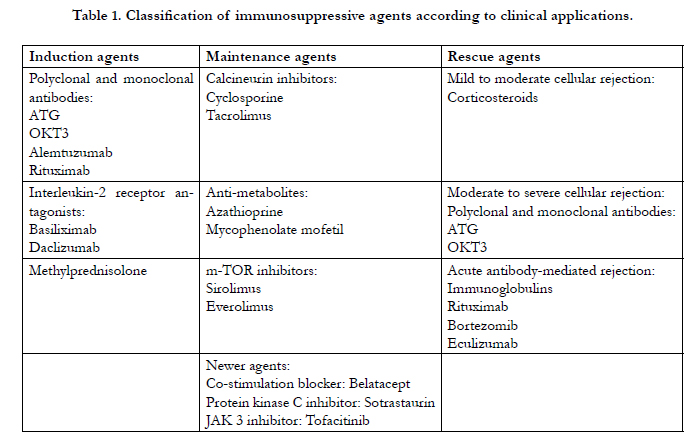

Table 1. Classification of immunosuppressive agents according to clinical applications.
The literature search was carried out in PubMed and relevant websites by using the search terms “kidney transplantation”, “immunosuppressive agents”,“immunology” and “outcomes”. Relevant references were compiled by using EndNote software(Version X 7.4; Thomson Reuters, Philadelphia, PA, USA).
Sir Peter Medawar, the father of transplantation, introduced the concept of transplantation immunology from his pioneering experimental works done between 1943 and 1944. He demonstrated that the second skin graft in the same animal was rejected more readily than the first skin graft, which was due to active immunisation from the first graft [6,7]. The role of lymphocytes in the rejection process was demonstrated much later after the development of hybridoma technology[8].The importance of a humoral component in hyperacute rejection was emphasised by Kissmeyer-Nielsen in 1966 who described the destructive effects of preformed antibodies on the allograft[9].
Both innate (dendritic cells, macrophages, neutrophils, mast cells and natural killer cells) and adaptive (T and B cells) immune systems are implicated in the allograft rejection process. The innate immune system is activated by damage-associated molecular patterns (heat-shock proteins, adenosine triphosphate, uric acid, ribonucleic acid (RNA), deoxyribonucleic acid (DNA)), proteins derived from extracellular matrix (hyaluronan fragments and heparin sulphate), and cytokines and chemokines released due to ischaemia-perfusion injury and microbial products. The activated innate immune system triggers the adaptive immune system leading to cellular rejection. In addition, recognition and presentation of the alloantigens leads to activation of the adaptive immune system[10].
Allorecognition can occur by direct or indirect pathways[11, 12]. After establishment of the vascular connection between donor and recipient, the activated dendritic cells migrate out of the graft to the T-cell rich regions of the recipient lymph nodes where they encounter naive recipient T cells[13]. The donor dendritic cells and recipient T cells engage each other using cell surface receptors, the major histocompatibility complex (MHC) molecules on the dendritic cell and the T cell receptor (TCR), the junction is called an “immunological synapse”, thereby generating antigenspecific intracellular signal (signal 1)[14, 15]. Simultaneously, additional molecules coalesce in the synapse to generate second signal called co-stimulation signal (signal 2), which is essential for complete T cell activation. Lack of signal 2 leads to either anergy or apoptosis [11, 14].
The receptor-ligand interaction between T-cells and the antigen presenting cells (APCs), which are involved in generation of costimulatory signals are CD28-B7 and CD154-CD40. CD28 and CD154 are expressed on T cells and their ligands B7 and CD40 are expressed on APCs. CD28 consists of two ligands, B7-1 (CD80) and B7-2 (CD86). T cells also express cytotoxic T-lymphocyte associated antigen-4 (CTLA-4), which is homologous to CD28, but has a higher affinity than CD28 to bind B7. Binding of CTLA-4 to B7 (both CD80 CD86) leads to generation of inhibitory signal to terminate T cell response [16, 17].
Following assembly of immunological synapses, the combination of signal 1 and 2 activates three downstream signal transduction pathways within the cytoplasm of the T cell: the calcium-calcineurin pathway, the RAS-mitogen activated protein kinase pathway, and the IKK-nuclear factor κB (NF- κB) pathway [18-20]. The signals reach the nucleus and activates gene transcription factors including the nuclear factor of activated T cells (NFAT), activated protein-1, and NF- қB, respectively. As a result of gene transcription, several new molecules and cytokines including CD25, CD154, interleukin-2 (IL-2) and interferon-γ (IFN- γ) are secreted and their receptors expressed [21].
IL-2 binds to its own receptor on the surface of T cell in autocrine fashion (signal 3), which, activates the mammalian target of rapamycin (mTOR) pathway, phosphoinositide-3-kinase (PI3K) pathway and Janus kinase/signal transducers and activators of transcription protein pathway (JAK/STAT), which allow the activated T cells to progress through the cell division cycle and clonal expansion of donor HLA/ peptide -specific effector (CD8+ cytotoxic T cells) T cells [22, 23]. These cells produce CD8+ T-cell mediated cytotoxicity, help macrophage-induced delayed type hypersensitivity response (CD4+Th1) and help B cells for antibody production (CD4+Th2) [24, 25]. A subset of activated T cells (CD4+ or CD8+) survive in an inactive state for a long period, called the memory T cells, but will quickly expand and mount an aggressive immune when re-exposed to the same alloantigen [26].
In addition to production of donor-specific anti-HLA antibodies, B cells play an important role in processing transplant alloantigen and presentation to the alloreactive T cells, thereby amplifying T cell-mediated allograft damage. B cells recognise transplant antigens in their native forms without requirement of processing and presentation to MHC molecules [27]. B cells also internalise antigens, process them and present to the T cells through the indirect pathway of allorecognition. They receive signals from T cells via CD40 by binding to the T cell CD40L, which upregulate expression of B7 molecules on B cells and facilitate antigen presentation and T cell co-stimulation[28]. Cross-linking of unprocessed antigen to the antigen-specific surface antibodies stimulates B cell activation, proliferation, and differentiation in to a plasma cell. Some of the activated B cells become memory B cells. The anti- HLA antibodies produced by plasma cells bind alloantigen and cause graft injury either by activating the complement cascade known as complement-dependent cytotoxicity (CDC) or via Fc receptor (CD16)in the natural killer cells, the antibody-dependent cellular cytotoxicity (ADCC)[29].
The potential role of regulatory B cells in induction of tolerance is under investigation. More recently, a subset of B cells, so called transitional B cells (TrB) with surface markers of CD27negCD24hiCD38hi, have been recognised, which exhibit suppressive function conducive to induction of tolerance. The IL-10 secreting TrB cells can suppress T helper cells and effector T cell responses. The concomitant production of TNF-α by B cells overcomes this inhibitory function. Thus the effects of intervention on the subsets of these two types of TrB cells to induce tolerance in RT, requires further investigation [30, 31].
Plasma cells can produce antibodies against both HLA and non- HLA antigens. Non-HLA antibodies directed against donor endothelial antigens such as MHC class I polypeptide-related sequence A or B (MICA and MICB), smooth muscle antigen (vimentin), collagen-V and cell surface receptor such a type I angiotensin II receptor are reliably detected by currently available techniques [32]. Several studies have suggested that DSA to HLA antigens and endothelial antigens may be a driver for both acute and chronic AMR[33].
Immunosuppressive Agents in Renal Transplantation
Total lymphoid irradiation (TLI) has been the first method of immunosuppression in human RT based on the principle of the destruction of blood cells in bone marrow and lymphoid tissue responsible for rejection[34].In a prospective randomised trial, which compared pre-operative TLI withpost-operative cyclosporine therapy, Waeret al. observed significantly high incidence of acute rejection rate in the TLI group, although the infectious complications were identical [35].Zhu et al. successfully desensitised and rescued highly sensitised and RT recipients with AMR using a combination of TLI, low-dose IVIG and ATG and plasmapheresis[36].The side-effects of TLI, such as nausea, vomiting, diarrhoea, hair loss, bone marrow suppression and infections made this form of treatment less favourable. It is more effective if given prior to transplantation. Local graft irradiation was in routine practice for some time for prevention and treatment of refractory acute rejection, but with the availability of better alternatives, TLI has fallen out of favour [37, 38].
Zukoski and Lee of Texas documented the benefit of corticosteroid therapy, first in a canine model, followed by in man [39]. From 1966 to 1978 conventional therapy consisted of azathioprine and high-dose prednisolone, which wasassociated with complications such as bone marrow aplasia, gastrointestinal perforation, weight gain, hyperlipidemia, diabetes, hypertension, and bone disease. Steroids act by blocking IL-2 gene expression on the T-cellsand APCs. Non-specific immunosuppressive effects like lymphopenia and chemokine inhibition leading to migration of monocytes in the area of inflammation, may also contribute to its action[40].
Several trials compared the efficacy and safety of low-dose versus high-dose steroids and concluded that low-dose steroids were as effective as high dose steroids in preventing rejections and steroid-related complications, but a large dose of azathioprine (at least 2mg/kg/day) was recommended [41, 42].High dose steroid therapy is the first line approach to the treatment of acute rejection. High dose oral steroid versus high- and lower intravenous doses of steroid have been examined in randomised trials. Low dose intravenous steroids (3mg/kg IV bolus) is found to be as effective as high dose steroid (15-30 mg/kg IV bolus) and this was not associated with increased incidence of steroid-resistant rejection [43, 44].
The detrimental effect of steroids on the metabolic profile begins in the early post-transplantation period. The outcome of complete avoidance of steroids was examined in randomised trial using IL-2RA induction.CNIs and maintenance with cyclosporine and MMF, where steroid withdrawal after 1 week was not associated with rise in acute rejection rate or graft failure[45-47].
The pharmacokinetic interaction of steroid with MMF and tacrolimus leads to alteration in the bioavailability of these drugs. Induction of uridine diphosphate glucuronosyltransferase activity by the steroids, increases the clearance of mycophenolic acid, thereby reducing the exposure to MMF. Tapering of steroid in the post-transplant period leads to increased trough, peak and 12 hours area under the concentration curve of MMF[48]. Steroids induce both cytochrome P450 3A (CYP3A) enzymes and P-glycoprotein (P-gp) in the liver and intestine. Tacrolimus is a substrate for these enzymes, thus leadsto increased bioavailability of tacrolimus when steroid is tapered or stopped (as high as 25%) after RT, which may cause nephrotoxicity[49].
The modern era of pharmacological immunosuppression was initiated by Schwartz and Dameshek in 1959 by documenting that the antiproliferative drug 6-mercaptopurine (6-MP) dampened antibody production and prolonged rabbit skin allograft survival[50]. The imidazole derivative of 6-MP, azathioprine, was used by Sir Roy Calne in 1960 demonstrating the prolonged survival of canine renal transplants from 7.5 to 23.7 days[51]. Azathioprine is metabolised in liver by thiopurine methyl transferase (TPMT) to 6-MP, the active metabolite, but other pathways also exist and explain individual variation in its metabolism. It interferes with purine metabolism and RNA synthesis, thus inhibiting gene replication and T cell activation. Individuals with deficiency of TPMT are more sensitive to its myelosuppressive effects[52].
The three pivotal trials, the U.S Renal Transplant Study, the Tri- Continental Study and the European Mycophenolate Mofetil Study compared MMF versus azathioprine or placebo in patients on baseline cyclosporine-prednisolone regimen. All trials demonstrated significant reduction in the incidence of acute rejection in MMF group at 6 months (19.8% vs.38%; 19.7% vs.35.5%; and 17.5 vs. 46.4%, respectively)[53-55], although graft and patient survivals were not different at 1 year. The cost differential between MMF and azathioprine was 10fold to 15 fold. An analysis of 49666primary renal allograft recipients reported to the US renal database system suggested that continued therapy with MMF was associated with protective effect against declining renal function at 1 year compared with azathioprine[56].
Conversion to azathioprine in patients on cyclosporine was examined in several trials, which showed increased risk of rejection (up to 25%), but there was no difference in the graft and patient survivals at 15 years of follow-up[57-59]. In patients receiving CNI together with azathioprine who developed CAI, switching to MMF and reduction of CNI dosage, was associated with either stabilisation or an improvement in renal function[60]. In an European randomised study involving 500 patients, addition of azathioprine to tacrolimus based regimen did not show any difference in the graft survival, patient survival, and acute or chronic rejection[61]. Gradually azathioprine has been replaced with MMF in modern immunosuppressive protocols, butused during pregnancy due to reduced association with foetal malformations[62].
Cyclosporine was isolated in 1969 from a soil fungus Tolypocladium inflatum (Gams) and its immunosuppressive action in transplantation elucidated by Jean F. Borel[63, 64].Cyclosporine combines with cyclophilin, and the complex thus formed,binds to calcium-dependent and calmodulin-dependent phosphatase, the calcineurin, therebyblocks the dephosphorylation of cytosolic form of the nuclear factor of activated T-cells (NFATc) and prevents it from translocating into the nucleus (NFATn) and to the DNA promotor region, thereby inhibits IL-2 synthesis. Blockade of IL2 gene transcription leads to failure of T cell clonal expansion and differentiation of precursor to mature cytotoxic T cells[64]. Clinical trials of cyclosporine in renal transplantation began in Cambridge in 1978 and cyclosporine was introduced into immunosuppression regimen protocols world-wide in 1982[65, 66].
The original, oil-based formulation of cyclosporine(Sandimmune®; Novartis Basel, Switzerland) was introduced in 1983, which showed significant interpatient and intrapatient variability doe to slow absorption. This made dosing difficult and increased the risk of chronic rejection. In 1995, a microemulsion formulation of cyclosporine, Neoral (Sandimmune Neoral®, Novartis Basel, Switzerland) was introduced, which has better absorption leading to improved bioavailability with less variability in denovo and stable transplant patients. Neoral reduced the acute rejection rate significantly although there was no difference in the long-term graft and patient survival[67-69]. In recent years several generic preparation of microemulsion formulations are available; however the results are variable due to variable absorption profile leading to change of dosage in about 20% patients and also increase in the incidence of acute rejection. An analysis of data from Collaborative Transplant Study showed significantly worse 1 year graft survival in patient who had received generic formulation of cyclosporine. It is mandatory to monitor patients more closely when generic formulation is used[58, 70, 71].
The value of monitoring cyclosporine level 2 hours (C2) after administration has been examined in several studies, which have shown variable results, although majority of them have shown that dosing of cyclosporine based on C2 levels (>1500 μg/L in first 2 weeks after RT) reduced acute rejection significantly. However, trough level (C0) remains the standard despite inherent poor correlation with the outcomes[72-74].
The introduction of cyclosporine significantly improved graft survival at 1 year compared to azathioprine and steroid group (89.5% vs. 50%)[75]. Several studies conducted in Europe, Canada, Minneapolis, Milan, Pittsburgh, Sydney and data from Collaborative Transplant Study have confirmed the improved graft survival with the use of cyclosporine[75-77][78][57, 79, 80].In order to reduce the side-effects such as infections, nephrotoxicity and B-cell lymphoma; low dose cyclosporine was combined with azathioprine and low dose steroid, termed as ‘triple therapy’. A randomised trial comparing double therapy (cyclosporine and azathioprine) with triple therapy (low dose cyclosporine, azathioprine and prednisolone) in cadaveric RT showed no difference in the incidence of acute rejection, infection, graft survival (54.4% vs. 59.6%) and patient survivals (79.8% vs.82.3%) at 5 years[81]. Similar results were reported in other studies using triple therapy[59].
A randomised controlled trial from Milan comparing triple therapy versus and high dose cyclosporine and steroids showed similar graft and patient survival between the two groups, but there were more rejection episodes in the triple therapy group with evidence of greater renal impairment and infection in the highdose cyclosporine group[82].Triple therapy replacing azathioprine with MMF has resulted in significant reduction in the incidence of acute rejection episodes (44% versus 31%; P<0.01), although there was no difference in the graft or patient survival rate[83]. ATG, OKT3 or more recently,IL-2RA monoclonal antibodies (basiliximab and daclizumab) are routinely added to triple therapy in patients with delayed graft function and sensitisation. This quadruple therapy or sequential therapy allows one to either delay the introduction of CNI or to use in reduced dose, respectively, while the kidney recovers from acute tubular necrosis[84, 85].
Acute nephrotoxicity is largely reversible but chronic nephrotoxicity is mostly irreversible with non-specific histological damage to glomeruli, blood vessels and interstitium[86]. In the Symphony study, in the first year post-transplantation, cyclosporine was associated with higher blood levels of uric acid, systolic and diastolic pressure in comparison to tacrolimus and sirolimus[87]. Overthe last two decades, tacrolimus has gradually replaced cyclosporine because of superior resultsyielded by it.
Like cyclosporine, tacrolimus is a CNI, which was introduced in 1987. Tacrolimus was isolated from a soil fungus, Streptomyces tsukubaensis and was found to be 100 times more potent than cyclosporine. Structurally both are different, but have similar mode of action. Tacrolimus binds to FK binding protein, calcium, calmodulin and calcineurin, which inhibits the phosphatase activity of calcineurin and thereby blocks translocation of cytosolic NFATinto the nucleus, leading to inhibition of IL-2 gene transcription and T-cell activation[88, 89].
The phase III U.S. multicentre trial compared the efficacy and safety of tacrolimus with that of Sandimmune cyclosporine. At 1 year, there was significantly low incidence of acute rejection in tacrolimus group (30.7% vs. 46.4%; P=0.001), low incidence of moderate-to-severe rejection (10.8% vs. 26.5%), at 5 years patients with serum creatinine value greater than 150μg/L was lower in tacrolimus group (40.4% vs. 62%; P=0.0017), but tremor and paraesthesia were more common in tacrolimus group. There was no difference in the 1 year patient (95.6% vs. 96.6%) and graft survival (91.2% vs. 87.9%) between the two groups. The incidence of post-transplant diabetes mellitus (PTDM) was 19.9% in the tacrolimus group and 4.0% in the cyclosporine group (P<0.001), and was reversible in some patients [90].
A randomised prospective trial comparing tacrolimus/ azathioprine, cyclosporine Neoral /MMF, and tacrolimus/MMF showedno difference in the acute rejection episodes, but there was a significant difference in the number of patient requiring ATG (4.2% in tacrolimus/MMF arm compared with 10.7% in the cyclosporine/ MMF arm and 11.8% in the tacrolimus/azathioprine arm; P=0.05). There was no difference in the patient and graft survival at 1, 2 or 3 years[91]. Combination of sirolimus or MMF with tacrolimus based regimens did not show any difference in the incidence of acute rejection, patient or graft survival[92]. Comparison of dual therapy (tacrolimus/prednisolone) with triple therapy (tacrolimus/MMF/prednisolone) showed significantly low incidence of acute rejection in the triple therapy group (44% vs, 27%; P=0.014). There was no difference in the patient and graft survival, incidence of delayed graft function, CMV and PTDM between the two groups[93].
A meta-analysis of 30 trials (4102 patients) comparing tacrolimus with cyclosporine showed significant reduction of graft loss in tacrolimus treated recipients (RR=0.56), less acute rejection (RR=0.69), less steroid-resistant rejection (RR=0.49), but more diabetes mellitus requiring insulin (RR = 1.86), tremor, headache, diarrhoea, dyspepsia, and vomiting. Cyclosporine treated recipients had significantly more constipation and cosmetic side effects. No differences were seen in infection or malignancy [94]. Several trials have confirmed better renal function associated with tacrolimus compared to cyclosporine [95],[96],[97].
Tacrolimus has been proven effective as rescue therapy in cyclosporine- treated patients with steroid-resistant acute rejection episodes[98, 99]. In Pittsburgh, 5-year follow-up of 169 patients, who were converted from cyclosporine to tacrolimus for refractory rejection, showed 74% success rate and a mean serum creatinine of 202μmol/L. Steroid withdrawal was achieved in 22% of cases after conversion to tacrolimus[100].
In a large European study on tacrolimus conversion for cyclosporine- induced toxicities, successful outcomes were achieved in resolving gingival hyperplasia, hypertrichosis, hyperlipidaemia and hypertension[101].With the use of tacrolimus, nephrotoxicity leading to CAI and metabolic side-effects, particularly PTDMhave generated major concerns. Several CNI minimising or sparing protocols have been examined to assess the efficacy of low dose CNIs in combination with other agents, which have shown to reduce premature graft loss.In the ELITE (Efficacy Limiting Toxicity Elimination) Symphony study, a regimen of daclizumab, mycophenolate mofetil, and corticosteroids in combination with low-dose tacrolimus was superior to regimens involving daclizumab induction plus either low-dose cyclosporine, low-dose sirolimus, or standard-dose cyclosporine without induction, in improving renal function, allograft survival, and acute rejection rates[102, 103].
Non-adherence is a common and major cause of RT failure and amounts to seven-fold risk of graft failure in non-adherent group compared to adherent group (OR=7.1; P<0.001)[104]. To address the nonadherence issue, a once-a-day (QD) formulation of tacrolimus (Advagraf®) has been approved in several countries since 2007. Several prospective studies have assessed the efficacy, safety, acute rejection, graft dysfunction and graft loss of QD preparation with twice-a-day (BID) formulation (Prograf®) both in de novo initiation or conversion settings. A review including all published phase III/IV studies in de novoinitiation concluded that QD is as effective as BID in preventing acute rejection, graft dysfunction and graft loss[105]. The early conversion from tacrolimus BID to QD has the theoretical advantages of reducing the odds of underexposure with tacrolimus in early post-transplantation, however there is paucity of data regarding efficacy and safety of the early conversion. The recommendation from the French expert panel is to perform early conversion (1:1mg) after bowel movement has resumed and a stable state of the tacrolimus trough level has been achieved. If the trough level with BID level is below the target range, conversion should be postponed[106]. Following de novo initiation, tacrolimus systemic exposure is reduced by approximately 30% with the QD formulation. The reduction is lower if first dose is given pre-operatively. Therefore, it is recommended to initiate tacrolimus QD pre-operatively. Following conversion, 10-15% decrease in trough level is observed, which does not translate into an equivalent decrease in area under the curve (AUC). There is no difference in the glycaemic control, renal function, patient and graft survival between the two groups, but there is trend for improved adherence with QD formulation[107].
MMF has been used extensively in all organ transplant recipients due to its good safety profile, efficacy,and easeof its administration without need of mandatory monitoring. The active metabolite is mycophenolic acid, which inhibits the enzyme inosine monophosphate dehydrogenase and thereby purine nucleotide synthesis,blocks both T and B lymphocyte proliferation[108].
The three pivotal trials, the U.S Renal Transplant Study, the Tri- Continental Study and European Mycophenolate Mofetil Study compared MMF versus azathioprine or placebo in patients on baseline cyclosporine-prednisolone regimen (see section on azathioprine) suggested a lack of nephrotoxicity, neurotoxicity, or hepatotoxicity. Significant incidence of myelotoxicity and gastrointestinal (GI) side-effects were reported. The GI side-effect was significantly reduced with the use of enteric-coated mycophenolate sodium (Myfortic®, Novartis)[109]. There was also consistent increase in the incidence of cytomegalovirus (CMV) infection in the MMF group. The U.S Pivotal trial showed significant benefit of MMF to the higher immunological risk patients in reducing the risk of rejection, particularly for African-Americans[110].
A meta-analysis of 19 trials involving 3143 patients has shown that MMF used with a CNI confers a clinical benefit over azathioprine by reducing the risk of acute rejection (RR=0.62) and graft loss (RR=0.76), with no difference in other adverse events except diarrhoea [111]. A single centre trial evaluated the combination of MMF and tacrolimus plus steroids versus last two agents and observed a decreased risk of acute rejection episodes from 44% to 27% at 1 year[112]. Tacrolimus in combination with MMF providedbetter renal function, less hypertension and reduced hyperlipidaemia than in combination with sirolimus[92].
Administration of MMF for the treatment of acute rejection episodes has failed to show any benefit. However, a multicentre study has suggested that MMF reduced the incidence of steroidresistant acute rejection episodes[113].The use of MMF has allowed reduction of CNI exposure after 3 months (cyclosporine C0 100 to 150 ng/mL; tacrolimus C0 5 to 7 ng/mL) leading to improved creatinine clearance, uric acid, blood pressure and triglyceride values[114]. Several studies have examined elimination of CNIs to avert chronic nephrotoxicity. Withdrawal of cyclosporine and continuation of MMF plus steroid at 3 months was associated with two fold increase in acute rejection episodes, although better creatinine clearance, reduced blood pressure and favourable lipid profile was observed[115].
For avoidance of CNIs, MMF and steroids has been used in combination with sirolimus[116], basiliximab/sirolimus[117], or belatacept/ basiliximab[118]. An excessive occurrence of acute rejection episodes have been observed in studies where CNI was not used. In a Spanish study, 65% of MMF-treated patients remained on CNI free regimen at 12 months, but only 36% remained CNI free at 5 years[119].
A meta-analysis of nine RCTs (1820 participants) assessed the effect of steroid withdrawal between 3 and 6 months of RT in patients on CNI plus MMF. Use of cyclosporine was associated with an increased incidence of biopsy-proven acute rejection (BPAR) (RR=1.61).Contrarily, tacrolimus allowed steroid withdrawal without increased incidence of BPAR[120]. MMF is also shown to reduce the incidence of chronic allograft nephropathy (CAN) and benefit those patients with evidence of early CAN[121].In summary, MMF has become a component of several immunosuppressive regimens resulting in better outcomes compared to azathioprine and has been successful in reducing CNI-induced nephrotoxicity.
Sirolimus is a macrocyclic lactone, a fermentation product isolated from Streptomyces hygroscopicus[122]. Everolimus was synthesised from sirolimus by substitution at position 40 at its structure by 2-hydroethyl chain, which has improved oral bioavailability. mTOR is serine-threonine kinase that acts as a scaffold for binding of proteins, which and a key component in cell cycle regulatory signalling pathway. Sirolimus and everolimus act by inhibiting the mTOR and inhibit T-cell proliferation. After entering the cells, mTOR-Ibind with FK binding proteins, which further binds with mTOR and blocks its action resulting in inactivation of S6K1 and 4EBP and inhibition of CD28-mediated downregulation of IκBα, a regulatory protein that upregulates IL-2 transcription[123]. This leads to cell cycle arrest in late G1 phase[124]. Sirolimus has no nephrotoxicity but in addition to its immunosuppressive effects it inhibits proliferation of fibroblasts, endothelial cells, hepatocytes and smooth muscle cells [125, 126].
mTOR-Ihave been evaluated in RT as an addition to CNI-based therapy, as de novo immunosuppression from the time of RT, as a later addition to CNI to enhance immunosuppression in response to acute rejection, and as a substitution for CNIs in the presence of nephrotoxicity or CAI in the maintenance phase. When sirolimus was compared with Sandimmune cyclosporine in combination with azathioprine and prednisolone, there was no difference in the incidence of acute rejection (41% versus 31% at 12 months)[127]. Similar results were observed when azathioprine was substituted with MMF (27% versus 18.5%)[116]. A registry analysis suggested higher incidence of acute rejection, higher rate of delayed graft function and reduced allograft survival in RT recipients, when combination of sirolimus and MMF was compared with tacrolimus/MMF or cyclosporine/MMF regimens[128]. Two large randomised trials ORION[129] and SYMPHONY[102] suggest that combination of sirolimus and MMF is inferior to low-dose tacrolimus and MMF-based triple therapy.
In a systematic review by Webster et al. (33 trials: sirolimus (27); everolimus (5) and head-to-head (1)), [130]; when mTOR-I replaced CNI there was no difference in acute rejection, but serum creatinine was lower, and bone marrow more suppressed (leukopenia: RR 2.02; thrombocytopenia: RR 6.97; anaemia: RR 1.67). When mTOR-I replaced antimetabolites, acute rejection (RR 0.84) and CMV infection (RR 0.49) were reduced, but hypercholesterolaemia was increased (RR 1.65). There was no significant difference in mortality, graft loss or malignancy risk for mTOR-I in any comparison. The use of mTOR-I immediately after RT is limited due to adverse effects on would healing and lymphocele. However, replacement of CNI with sirolimus as maintenance therapy before structural changes have occurred in cases of early CAI has shown to improve renal function[131].
The Sirolimus Renal Conversion Trial (CONVERT trial) examined the effects of converting from CNI to sirolimus as maintenance therapyand showed (particularly in the subgroup with a baseline GFR of > 40 mL/min and a urinary protein-to creatinine ratio of ≤ 0.11) superior renal function in patients treated with sirolimus for 12 to 24 months[132]. RCT by Guerra etal. suggest maintenance therapy with tacrolimus/MMF is more favourable than either tacrolimus/sirolimus or cyclosporine/sirolimus[133].
The efficacy of everolimus with reduced CNI in comparison to conventional MMF and standard CNI in de novoRT have been addressed in two large randomised trials; namely, the A2309 trial[134]; and the EVEREST study[135]; and third TRANSFORM study[136] is in recruitment stage. The available data indicate that everolimus targeting 3-8 ng/ml can achieve at least 60% reduction in maintenance concentration of CNI without loss of efficacy in de novo RT recipients at low to moderate immunological risk. The benefit in terms of renal function was achieved when very low CNI exposure was achieved. Early withdrawal of steroids in everolimus with reduced CNI have shown an increased risk of acute rejection[137].
Several randomised trials have investigated the effect of introducing everolimus and withdrawing CNI in RT recipients, where the time of CNI withdrawal varied from seven weeks to seven years. Studies of early switch at seven weeks or halving of CNI dose from two weeks onwards followed by full withdrawal at 2 months was associated with high rate of BPAR at 12 month (27.5% and 31%, respectively)[138-140]. Two large studies have demonstrated improved renal function when the switch was initiated at months 3-4.5, although ZEUS study showed high incidence of mild BPAR after CNI withdrawal compared to CNI continuation(13.6% versus 7.6%) [141, 142]. Two studies of late conversion (APOLLO [mean seven years][143] and ASCERTAIN [mean >5 years][144] showed no loss of efficacy after switch. Data regarding development of de novoDSA in patients receiving everolimus is inadequate. Patients on CNI with declining renal function, malignant neoplasms or non-melanoma skin cancers have benefitted when switched to everolimus[145].
In the early 1950s, lymphocytes were recognised as the predominant effector in rejection and by the mid-1960s, lymphocyte depleting antibodies such as antilymphocyte serum (ALS), antilymphocyte globulin (ALG) and rabbit antithymocyte globulin (rATG) were isolated from animal experiments, which were composed of many undefined specificities, hence collectively known as polyclonal preparations. In 1975, Kohler and Milstein, developed monoclonal antibodies by the hybridoma technology, which has genetically defined monoclonal specificity and overcame the shortcomings of polyclonal preparations, particularly specificity and variability.Anti-CD3 monoclonal antibody (OKT3, Muromonab) was the first monoclonal antibody specific for CD3, which very rapidly cleared T-cells from peripheral circulation and was found to be very effective in prevention and treatment of rejection. Subsequently, with the advances in genetic engineering, several monoclonal antibodies were developed, whose efficacy and safety and clinical applications are described below. There are currently three antibodies which are used for induction therapy: IL-2 receptor antagonist (basiliximab and daclizumab), rATG and alemtuzumab.
Rabbit ATG is commonly used for induction and treatment of steroid-resistant cellular and antibody mediated rejections. In 1960s and 1970s, ALS and ALG were used to reduce the acute rejection, which delayed the onset of acute rejection, but did not alter the ling-term survival[146, 147]. The use of polyclonal antibodies declined after introduction of cyclosporine because of the increased incidence of infections and malignancies. However, ATG has been investigated in combinations with CNIs, MMF and steroids in higher immunological risk patients, recipients of donation after circulatory death and extended criteria donors, delayed graft function, particularly where avoidance of prolonged calcineurin inhibitor is desired [148-152]. With better viral prophylaxis and improved understanding of the infectious aetiology of post-transplant lymphoproliferative disorder (PTLD), ATG is being used in a variety of situations with confidence.It causes Tcell depletion through complement activation. It also modulates cell surface and adhesion molecules.[153]. Side- effects include early acute cytokine release syndrome, delayed serum sickness and higher infections with CMV and other infections.
Pilch et al. compared the efficacy and safety of rATG and IL-2 receptor antagonists (basiliximab and daclizumab) in a prospective randomised controlled trial (RCT) in combination with tacrolimus, MMF and steroid, and showed no difference in the incidence of acute rejection, renal function and graft survival between the two groups. There was increased incidence of BK virus infection in the rATG group [154]. In a meta-analysis by Liu et al. including 6 studies (853 patients), there was no difference between rATG and basiliximab in terms of BPAR, delayed graft function, graft loss and patient death. But basiliximab group had lower incidence of infection and neoplasm. Basiliximab is considered as effective as rATG, therefore, is safer and preferable option for induction therapy in RT [155].
Recent evidence suggests that de novo DSA is associated with AMR and graft failure afterRT. The effects of induction immunosuppression with rATG and basiliximab on DSA wasassessed by Brokhofet al.in 114 consecutive moderately sensitized (positive DSA andnegativeflow crossmatch) recipients who received deceased donor RT with a follow-up of 36months. The incidence of DSA (HR=0.33) and AMR (HR=0.9) weresignificantlylower in the ATG group[156].
In a comprehensive systematic review, Webster et al. examined the safety and efficacy of ATG, OKT3 and steroids in the treatment of acute rejection episodes. In treating the first rejection episodes, antibodies were better than steroids in reversing rejection episodes and preventing graft loss, but there was no difference in preventing subsequent rejection ordeath at 1 year.For the treatment of steroid-resistant rejection, there was no benefit of OKT3 over ATG inreversing rejection, preventing subsequent rejection, preventing graft loss or death [157].
Muromonab (OKT3)
Orthoclone OKT3 is a murine IgG2a antibody that was first introduced in the early 1980s as an induction agent in sensitised patients, for the treatment of steroid-resistant rejections and in patients with delayed graft function to facilitate delay of CNI administration[158, 159].OKT3 binds to epsilon chain of the CD3 protein in association with the T cell receptor complex, and mediates complement-dependent cell lysis and ADCC, thereby clears all T-cells from peripheral circulation. Binding of OKT3 to CD3 leads to TCR-CD3 internalisation, thus T cells without TCR are incapable of receiving primary antigen signal and are immunologically inactive[160]. Lysis of T cells leads to release of cytokines causing severe systemic manifestations including pulmonary oedema and aseptic meningitis[158].
All trials in the past have shown OKT3 as an efficacious agent in the prevention and successful reversal of 80% of severe rejections, particularly those associated with vasculitis (Banff grade 2 or 3 rejection). OKT3 together with tacrolimus, MMF and prednisolone improved the graft survival and renal function in patients with steroid-resistant rejection [161]. Low doses OKT3 and low dose ATG were found to be equally effective in the treatment of steroid-resistant rejection[162]. However, the use of OKT3 in RT has been abandoned due to its severe side-effects and the availability of safer agents.
Interleukin-2 receptor (CD25) monoclonal antibody
Basiliximab and daclizumab are anti-CD25 monoclonal antibodies, which inhibit IL-2 binding to α-chain of the CD25 molecule and deprive T cells of this cytokine thereby preventing T cell activation and proliferation without causing cell lysis[163]. Therefore, they are also known as non-depleting antibodies.Daclizumab is a humanized anti-CD25 IgG1, while basiliximab is a chimeric anti- CD25 IgG1.Daclizumab and basiliximab have been shown to reduce modestly the incidence of acute cellular rejection compared with methylprednisolone induction when used with triple or dual immunosuppressive agents, with no side-effects[164]. There was no difference in the efficacy and safety between basiliximab and daclizumab in terms of BPAR, renal function, graft and patient survival[165].
In a phase III study,Nashan et al.assessed the ability of basiliximab to prevent acute-rejection episodes in renal allograft recipients in comparison to a placebo in patients receiving cyclosporine and steroids. The incidence of BPARat 6 months was significantly lower in the basiliximab group (29.8% vs. 44%), as was the incidence of steroid-resistant rejection episodes (10% vs. 23.1%) [166]. Webster et al. in a meta-analysis including 38 trials and 4893 participants, showed significant reduction of acute rejection at 6 months compared to placebo (RR: 0.66), but with no difference in the incidence of CMV infection, malignancy, graft and patient survival. There is no apparent difference in the outcomes between basiliximab and daclizumab [167].
Brennan et al., in a randomised trial, compared basiliximab with rATG in patients receiving cyclosporine, MMF and prednisolone, and showed lower incidence of acute rejection (25.5% vs. 15.5%) and steroid-resistant rejection (8% vs. 1.4%). Both groups had similar incidences of graft loss (9.2% and 10.2%), delayed graft function (40.4% and 44.5%), and death (4.3% and 4.4%). Patients receiving rATG had a greater incidence of infection (85.8% vs. 75.2%, P=0.03) but a lower incidence of CMV disease (7.8% vs. 17.5%, P=0.02). Patient and graft survival were similar in the two groups[168]. Similar results were observed by Noel et al. when daclizumab was compared with ATG [169]. At present, basiliximab has supplanted ATG as the most frequently used induction agent in RT.
Alemtuzumab
Alemtuzumab (Campath-1H) is a humanised rat monoclonal anti-CD52 antibody directed against the CD52 membrane protein present on most Tcells, B cells and monocytes [170]. It leads to rapid depletion of bulk of T cells, lesser depletion of B cells and monocytes by cell lysis, thereby causes cytokine release syndrome, but less in severity compared to rATG and OKT3 [171]. Because alemtuzumab does not clear plasma cells, there is increased incidence of AMR and development of DSA [172].
The role of alemtuzumab as an induction treatment followed by an early reduction in CNI and MMF exposure and steroid avoidance (3-C Trial in UK), and basiliximab-based induction treatment was examined in a RCT. The patients were randomly assigned to either alemtuzumab-based induction treatment (ie, alemtuzumab followed by low-dose tacrolimus and MMF without steroids) or basiliximab-based induction treatment (basiliximab followed by standard-dose tacrolimus, MMF, and prednisolone). Compared with basiliximab-based treatment, alemtuzumab-based induction therapy was followed by reduced CNI and MMF exposure and steroid avoidance; and reduced the risk of BPAR in patients receiving a RT (7% vs. 17%). There was no difference in the incidence of infections and graft loss [173].
In a meta-analysis including 10 RCTs (1223 patients), alemtuzumab induction had a lower risk of BPAR compared with basiliximab and daclizumab. No significant difference was observed in the risk of BPAR when induced with rATG. There was no difference in early or delayed graft loss, patient death, PTDM, when alemtuzumab was compared with IL-2RA and rATG. It is more acceptable to base the choice of induction agent on safety outcomes and/or costs [174].
In the prospective INTAC study, alemtuzumab was compared with rATG and basiliximab induction in patients who received tacrolimus and MMF as maintenance therapy and early steroid withdrawal was done at day 5. In low risk-group (alemtuzumab vs. basiliximab induction), there was low incidence of BPAR (3% vs. 15% at 3 months; 5% vs. 17% at 12 months; and 10% vs. 22% at 3 years). But among high-risk patients (alemtuzumab and rATG), no significant difference was seen in the incidence of BPAR(18% vs. 15%). The risk of cancer (5% vs. 1%) and serious infection (22% vs. 35%)were significantly high in the low risk group [175].
Rituximab
Rituximab is a chimeric monoclonal antibody specific for CD20, which is expressed on the majority of B cells, leads to depletion of these cells. Rituximab is used as an induction agent for desensitisation in ABO-incompatible donor recipient pairs or transplant across a positive crossmatch following antibody removal and in the treatment of AMR [176, 177]. In a double-blind, placebocontrolled study, van den Hoogen, et al. evaluated the efficacy and safety of rituximab as induction therapy in RT patients receiving either single dose of rituximab or placebo. Maintenance immunosuppression consisted of tacrolimus, MMF and steroids. Immunologically high-risk patients (PRA >6% or retransplant) not receiving rituximab had a significantly higher incidence of rejection (38.2%)compared to other treatment groups (rituximab-treated immunologically high-risk patients, and rituximab or placebotreated immunologically low-risk (PRA </= 6% or first transplant) patients 17.9%, 16.4% and 15.7%, respectively; P = 0.004). Thus rituximab induction was beneficial to the high-risk patients [178].
Fuchinoue et al. have reported their 5 year outcome of ABO-incompatible RT using rituximab induction and showed better outcome in terms of graft survival (100%, 96.8% and 99.2%, respectively), renal function,AMR (4%, 15.95 and 2.5%, respectively), and acute cellular rejection (4%, 9.5%, and 14.3%, respectively) in the rituximab treated ABO-incompatible RT compared to the ABO-incompatible RT who did not receive rituximab and ABOcompatible RT[179].
RT in the presence of DSA and positive CDC crossmatch carry significant risk of AMR and mortality. The desensitisation protocol consisting of rituximab, plasmapheresis and low dose IVIG was assessed by Riella at al. and showed 84% graft survival and 86% patient survival at 5 years. 61% of the graft experienced AMR and 1 graft was lost from hyperacute rejection. The mean serum creatinine was 170μmol/L at 5 years. Thus, desensitisation using rituximab induction provided acceptable results in living donor RT [180].Rituximab is used effectively in the treatment of PTLD in combination with chemotherapy and reduction of immunosuppression, where renal function has been well preserved [181, 182].
Belatacept
Belatacept, a fusion protein composed of the Fc fragment of human IgG1 linked to the extracellular domain of CTLA-4, selectively inhibits T-cell activation through costimulation blockade [183]. Balatacept has been in use since 2006 in two phase III studies, Belatacept Evaluation of Nephroprotection and Efficacy as First-line Immunosuppression Trial (BENEFIT) and BENEFIT– Extended Criteria Donors (BENEFIT-EXT) trial [184, 185].
The phase III BENEFIT study assessed a more intensive (MI) or less intensive (LI) regimens of belatacept, versus cyclosporine in adults receiving a kidney transplant from living or standard criteria deceased donors. At 1 year, the both belatacept groups and cyclosporine groups had similar graft and patient survivals (MI: 95%, LI: 97% and cyclosporine: 93%)better renal function (eGFR 65, 63 and 50 mL/min for MI, LI and cyclosporine, respectively), but belatacept patients experienced a higher incidence (MI: 22%, LI: 17% and cyclosporine: 7%) and grade of acute rejection episodes. Safety was generally similar between groups, but PTLD was more common in the belatacept groups [118].The phase III BENEFIT-EXT study evaluated similar drug regimens in extended criteria deceased donor RTs and showed better renal function (4-7 mls/min higher mean eGFR in the belatacept group), but the acute rejection rate, graft and patient survivals and infections were similar. The incidence of PTLD was high in the belatacept group [186]. The 7 years follow-up result of the BENFIT study has been published recently, showed a 43% reduction in death or graft loss for moth MI and LI belatacept regimens compared with cyclosporine regimen. The mean eGFR increased over the 7 year period with belatacept and decreased with cyclosporine regimen. The cumulative frequency of serious adverse events at month 84 were similar across treatment groups [187]. One limitation of the trial is that cyclosporine, a less contemporary immunosuppressive agent was utilised.
Bortezomib
Bortezomib is a proteasome inhibitor which causes phosphorylation of the Bcl2 family of proteins and the cleavage product induced G2-M cell arrest and apoptosis of the plasma cells and thereby inhibits antibody production. Several case series have shown successful reversal of severe AMR refractory to conventional therapy and preoperative desensitisation of highly sensitised positive crossmatch living donor RT [188-190]. In order to assess the efficacy of bortezomib in RT patients with positive DSA and biopsy-proven AMR, a prospective randomised trial (BORTEJECT) is underway in Vienna, which aims to assess the renal function, proteinuria, patient and graft survivals at 24 months [191].
Eculizumab
Eculizumab is a humanised monoclonal anti-C5 IgG antibody that binds to complement protein C5, preventing cleavage into C5a and C5b, and subsequent formation of C5b-9 or membrane attack complex. There are several case series reporting successful treatment of severe AMR refractory to conventional treatment and thrombotic microangiopathy post-RT [192, 193]. Stegall et al. from Mayo Clinic studied the efficacy of eculizumab in 26 recipients of highly sensitised recipients of living donor RT and compared with historical controls of 51 sensitised patients treated with similar plasma exchange-based protocol without eculizumab. The incidence of BPAR at 3 months was 7.7% in the eculizumab group compared with 41.2% in the control group. With eculizumab, AMR episodes were easily treated with plasma exchange, thus reducing the need for splenectomy. On 1-year protocol biopsy, transplant glomerulopathy was found to be present in 6.7% of eculizumab-treated recipients and in 35.7% of control patients [194]. More research needs to be undertaken in order to determine indications and the length of treatment for patients DSA and at risk of recurrence of haemolytic-uraemic syndrome[195].
C1 inhibitor in AMR
The safety and efficacy of C1 inhibitor (C1-INH, Berinert®), which inhibits the classical and lectin pathways of complement activation, is under evaluation in highly sensitised RT patients who are at risk of developing AMR. The plasma derived C1 inhibitor was given in addition to IVIg, plasmapheresis and rituximab and compared using placebo. In the study group there was significant reduction in the incidence of AMR, reduced C1q and DSA. C1-INH was also tested in AAMR, which showed favourable outcomes. However, the efficacy of this agents needs to be evaluated in prospective randomised trials [196, 197].
Agents Investigated in the Past
FTY-720 is a sphingosine-1-phosphate analogue which interferes with cell traffic between lymphoid organs and blood without impairing T- and B-cell activation, proliferation and effector function. Its efficacy and safety was tested in clinical trials, but further investigation was discontinued due to adverse effects on visual function [198].
Sotrastaurin is a protein kinase C signalling inhibitor, blocks IL-2 production and T-cell activation independent of the CNI pathway. In a phase II randomised study, de novo RTs received sotrastaurin was given to two groups of patients; standard exposure of tacrolimus (SET), reduced exposure of tacrolimus (RET) and control (SET + MMF). After 3 months, tacrolimus was omitted in the sotrastaurin group and MMF given. There was significantly high rate acute rejection, infections, GI side-effects in the sotrastaurin group leading to discontinuation of the study[199].
Tofacitinib is a small molecule agent which inhibits JAK3 and thereby inactivates JAK/STAT dependent IL-2 induced T-cell proliferation [200]. In a phase II study,Tofacitinib was compared with CNI-free regimens, where the incidence of acute rejection and graft function were comparable between the two groups. But the incidence of serious infection, anaemia, neutropenia and PTLD were significantly high in the Tofacitinib group. Further investigation of this agent has been abandoned [201].
There has been growing interest in promoting generic conversion from brand medications in clinical RT for cost-containment measures. However, due to drug variability, issues with bioequivalence, increased risk of rejection, graft loss and increased hospitalisation, concerns have been raised onconversion to generic formulations, particularly due to narrow therapeutic index of some of the drugs [202] . The available data on the efficacy and safety of generic conversion to brand formulations of tacrolimus (Prograf®), MMF (Cellcept®) and cyclosporine Neoral to generic formulations such as tacrolimus (Tacni®) MMF (Myfenax®, Mycept®) and cyclosporine (Iminoral®) is limited and variable. Prospective data on the pharmacokinetics including the area under the curve, Cmax, time to Cmax and trough levels are paramount to compare the two formulations [203]. A systematic review and meta-analysis has evaluated the clinical efficacy and bioequivalence of generic immunosuppressive drugsNeoral (cyclosporine) (32 studies), Prograf ® (tacrolimus) (12studies), and Cellcept® (mycophenolate mofetil) (six studies) in solid organ transplantation, withreference to the outcomes including patient survival, allograft survival, acute rejection, adverse events andbioequivalence. Pooled analysis of RCTs in patients with RT that reported bioequivalence criteria showedthat Neoral (two studies) and Prograf® (three studies) were not bioequivalent with generic preparations. The single Cellcept ® trial also did not meet bioequivalence. Acute rejection was rare but did not differ between groups. High quality data showing bioequivalenceand clinical efficacy of generic immunosuppressive drugs in patients with transplants were lacking, hence need for well-designed studies was recommended [204].
Conclusion
The pinnacle of success achieved in RT has evolved over the past century by passing through various milestones in the field of immunology and immunosuppressive drugs, which has become possible through relentless research, both in experimental animal models and human volunteers. Since the early years of TLI to the current stage of evaluation of costimulation blockade, significant reduction in the incidence of acute rejection has been achieved, but chronic AMR, side-effects of the drugs and their cost have been the target of intervention. Further development in both induction and maintenance immunosuppressive strategies is required to achieve an ideal regimen, which would prolong allograft survival with minimal complications.
References
- Shrestha A, Shrestha A, Basarab-Horwath C, McKane W, Shrestha B, et al.(2010) Quality of life following live donor renal transplantation: a single centre experience. Ann Transplant 15(2): 5-10.
- Merrill JP, Murray JE, Harrison JH, Guild WR (1984) Landmark article Jan 28, 1956: Successful homotransplantation of the human kidney between identical twins. JAMA 251(19): 2566-2571.
- Kidney Transplant Activity in 2013 in 104 Countries. World Health Organisation.
- Halloran PF (2004) Immunosuppressive drugs for kidney transplantation. N Engl J Med 351(26): 2715-2729.
- Stegall MD, Gaston RS, Cosio FG, Matas A (2015) Through a glass darkly:seeking clarity in preventing late kidney transplant failure. J Am Soc Nephrol 26(1): 20-29.
- Medawar PB (1944) The behaviour and fate of skin autografts and skin homografts in rabbits: A report to the War Wounds Committee of the Medical Research Council. J Anat 78(Pt 5): 176-199.
- Medawar PB (1945) A second study of the behaviour and fate of skin homografts in rabbits: A Report to the War Wounds Committee of the Medical Research Council. J Anat 79(Pt 4): 157-176.
- Kohler G, Hengartner H, Shulman M (1978) Immunoglobulin production by lymphocyte hybridomas. Eur J Immunol 8(2): 82-88.
- Kissmeyer-Nielsen F, Olsen S, Petersen VP, Fjeldborg O (1966) Hyperacute rejection of kidney allografts, associated with pre-existing humoral antibodies against donor cells. Lancet 2(7465): 662-665.
- He H, Stone JR, Perkins DL (2003) Analysis of differential immune responses induced by innate and adaptive immunity following transplantation.Immunology 109(2): 185-196.
- Game DS, Lechler RI (2002) Pathways of allorecognition: implications for transplantation tolerance. Transpl Immunol 10(2-3): 101-108.
- Vartdal F, Thorsby E (1999) Transplantation immunology--the role of human leucocyte antigen in allorecognition. Curr Top Pathol 92: 1-18.
- Ponticelli C (2014) Ischaemia-reperfusion injury: a major protagonist in kidney transplantation. Nephrol Dial Transplant 29(6): 1134-1140.
- Halloran PF (1999) T-cell activation pathways: a transplantation perspective. Transplant Proc 31(1-2): 769-771.
- Sim GK, Yague J, Nelson J, Marrack P, Palmer E, et al. (1984) Primary structure of human T-cell receptor alpha-chain. Nature 312(5996): 771-775.
- Snanoudj R, Zuber J, Legendre C (2010) Co-stimulation blockade as a new strategy in kidney transplantation: benefits and limits. Drugs 70(16): 2121-2131.
- Poirier N, Blancho G, Vanhove B (2010) Alternatives to calcineurin inhibition in renal transplantation: belatacept, the first co-stimulation blocker.Immunotherapy 2(5): 625-636.
- Strehlau J, Pavlakis M, Lipman M, Maslinski W, Shapiro M, et al. (1996) The intragraft gene activation of markers reflecting T-cell-activation and -cytotoxicity analyzed by quantitative RT-PCR in renal transplantation. Clin Nephrol 46(1): 30-33.
- Huang GN, Huso DL, Bouyain S, Tu J, McCorkell KA, et al. (2008) NFAT binding and regulation of T cell activation by the cytoplasmic scaffolding Homer proteins. Science 319(5862): 476-481.
- Zhao Z, Wang L, Yang C, Zhao T, Li L, et al. (2013) Soluble FGL2 induced by tumor necrosis factor-alpha and interferon-gamma in CD4+ T cells through MAPK pathway in human renal allograft acute rejection. J Surg Res 184(2): 1114-1122.
- Young-Fadok TM, Simpson MA, Madras PN, Dempsey RA, O'Connor K, et al. (1991) Predictive value of pretransplant IL-2 levels in kidney transplantation. Transplant Proc 23(1 Pt 2): 1295-1296.
- Taniguchi T, Minami Y (1993) The IL-2/IL-2 receptor system: a current overview. Cell 73(1): 5-8.
- Flanagan ME, Blumenkopf TA, Brissette WH, Brown MF, Casavant JM, et al. (2010) Discovery of CP-690,550: a potent and selective Janus kinase (JAK) inhibitor for the treatment of autoimmune diseases and organ transplant rejection. J Med Chem 53(24): 8468-8484.
- Goldman M, Druet P (1995) The TH1/TH2 concept and its relevance to renal disorders and transplantation immunity. Nephrol Dial Transplant 10(8): 1282-1284.
- Nickerson P, Steurer W, Steiger J, Zheng X, Steele AW, et al. (1994) Cytokines and the Th1/Th2 paradigm in transplantation. Curr Opin Immunol 6(5): 757-764.
- Bingaman AW, Farber DL (2004) Memory T cells in transplantation: generation, function, and potential role in rejection. Am J Transplant 4(6): 846-852.
- Cambier JC, Pleiman CM, Clark MR (1994) Signal transduction by the B cell antigen receptor and its coreceptors. Annu Rev Immunol 12: 457-486.
- Lederman S, Yellin MJ, Inghirami G, Lee JJ, Knowles DM, et al. (1992) Molecular interactions mediating T-B lymphocyte collaboration in human lymphoid follicles. Roles of T cell-B-cell-activating molecule (5c8 antigen) and CD40 in contact-dependent help. J Immunol 149(12): 3817-3826.
- Muro M, Llorente S, Marin L, Moya-Quiles MR, Gonzalez-Soriano MJ, et al. (2005) Acute vascular rejection mediated by HLA antibodies in a cadaveric kidney recipient: discrepancies between FlowPRA, ELISA and CDC vs luminex screening. Nephrol Dial Transplant 20(1): 223-226.
- Mehrotra A, Heeger PS (2014) B cells and kidney transplantation: beyond antibodies. J Am Soc Nephrol 25(7): 1373-1374.
- Cherukuri A, Rothstein DM, Clark B, Carter CR, Davison A, et al. (2014) Immunologic human renal allograft injury associates with an altered IL-10/TNF-alpha expression ratio in regulatory B cells. J Am Soc Nephrol 25(7):1575-1585.
- Dragun D, Philippe A, Catar R (2012) Role of non-HLA antibodies in organ transplantation. Curr Opin Organ Transplant 17(4): 440-445.
- Valenzuela NM, Reed EF (2013) Antibodies in transplantation: the effects of HLA and non-HLA antibody binding and mechanisms of injury. Methods Mol Biol 1034: 41-70.
- Hamburger J (1963) 11 Attempts at Renal Homotransplants in Man after Irradiation of the Receiver. Rev Med Chil 91: 446-459.
- Waer M, Vanrenterghem Y, Roels L, Verberckmoes R, Hauglustaine D, et al. (1988) Renal cadaveric transplantation in diabetics using total lymphoid irradiation or cyclosporin A. A controlled randomized study. Leuven Collaborative Transplantation Group. Transpl Int 1(2): 64-68.
- Zhu D, Qi G, Tang Q, Li L, Yang C, et al. (2014) Combination of Total Lymphoid Irradiation, Low-Dose IVIG and ATG as Rescue Therapy for Highly Sensitized and Antibody-Mediated Rejection Renal Transplant Recipients. Clin Transpl 215-221.
- Micke O, Seegenschmiedt MH, Bruns F, Matzkies FK, Schafer U, et al. (2002) Radiotherapy within the scope of allogeneic kidney transplantation: an indication for local irradiation?. Strahlenther Onkol 178(5): 280-285.
- Najarian JS, Ferguson RM, Sutherland DE, Slavin S, Kim T, et al. (1982) Fractionated total lymphoid irradiation as preparative immunosuppression in high risk renal transplantation: clinical and immunological studies. Ann Surg 196(4): 442-452.
- Zukoski CF, Callaway JM, Rhea WG Jr (1965) Prolonged Acceptance of a Canine Renal Allograft Achieved with Prednisolone. Transplantation 3: 380-386.
- Bush WW (1999) Overview of transplantation immunology and the pharmacotherapy of adult solid organ transplant recipients: focus on immunosuppression. AACN Clin Issues. 10(2): 253-269.
- d'Apice AJ, Becker GJ, Kincaid-Smith P, Mathew TH, Ng J, et al. (1984) A prospective randomized trial of low-dose versus high-dose steroids in cadaveric renal transplantation. Transplantation 37(4): 373-377.
- McGeown MG, Douglas JF, Brown WA, Donaldson RA, Kennedy JA, et al. (1979) Low dose steroid from the day following renal transplantation. Proc Eur Dial Transplant Assoc 16: 395-400.
- Kauffman HM Jr, Stromstad SA, Sampson D, Stawicki AT (1979) Randomized steroid therapy of human kidney transplant rejection. Transplant Proc 11(1): 36-38.
- Lui SF, Sweny P, Scoble JE, Varghese Z, Moorhead JF, et al. (1989) Lowdose vs high-dose intravenous methylprednisolone therapy for acute renal allograft rejection in patients receiving cyclosporin therapy. Nephrol Dial Transplant 4(5): 387-389.
- Cole E, Landsberg D, Russell D, Zaltzman J, Kiberd B, et al. (2001) A pilot study of steroid-free immunosuppression in the prevention of acute rejection in renal allograft recipients. Transplantation 72(5): 845-850.
- Kumar MS, Xiao SG, Fyfe B, Sierka D, Heifets M, et al. (2005) Steroid avoidance in renal transplantation using basiliximab induction, cyclosporine- based immunosuppression and protocol biopsies. Clin Transplant 19(1): 61-69.
- Woodle ES, Peddi VR, Tomlanovich S, Mulgaonkar S, Kuo PC, et al. (2010) A prospective, randomized, multicenter study evaluating early corticosteroid withdrawal with Thymoglobulin in living-donor kidney transplantation. Clin Transplant 24(1): 73-83.
- Cattaneo D, Perico N, Gaspari F, Gotti E, Remuzzi G (2002) Glucocorticoids interfere with mycophenolate mofetil bioavailability in kidney transplantation.Kidney Int 62(3): 1060-1067.
- Anglicheau D, Flamant M, Schlageter MH, Martinez F, Cassinat B, et al. (2003) Pharmacokinetic interaction between corticosteroids and tacrolimus after renal transplantation. Nephrol Dial Transplant 18(11): 2409-2414.
- Schwartz R, Dameshek W (1960) The effects of 6-mercaptopurine on homograft reactions. J Clin Invest 39: 952-958.
- Calne RY, Alexandre GP, Murray JE (1962) A study of the effects of drugs in prolonging survival of homologous renal transplants in dogs. Ann N Y Acad Sci 99: 743-761.
- Weiler S, Aellig N, Fauchere I, Jetter A, Corti N (2014) Treatment of gout in a renal transplant patient leading to severe thrombocytopenia. J Clin Pharm Ther 39(5): 571-572.
- Sollinger HW (1995) Mycophenolate mofetil for the prevention of acute rejection in primary cadaveric renal allograft recipients. U.S. Renal Transplant Mycophenolate Mofetil Study Group. Transplantation 60(3): 225-232.
- Browne BJ (1996) The Tricontinental Mycophenolate Mofetil Trial. Transplantation 62(11): 1697.
- European Mycophenolate Mofetil Cooperative Study Group (1999) Mycophenolate mofetil in renal transplantation: 3-year results from the placebo- controlled trial. Transplantation 68(3): 391-396.
- Meier-Kriesche HU, Steffen BJ, Hochberg AM, Gordon RD, Liebman MN, et al. (2003) Mycophenolate mofetil versus azathioprine therapy is associated with a significant protection against long-term renal allograft function deterioration. Transplantation 75(8): 1341-1346.
- Morris PJ, Chapman JR, Allen RD, Ting A, Thompson JF, et al. (1987) Cyclosporin conversion versus conventional immunosuppression: long-term follow-up and histological evaluation. Lancet 1(8533): 586-591.
- Talaulikar GS, Gallagher MP, Carney GM, Jadeer AA, Falk MC, et al. (2004) Switchover to generic cyclosporine in stable renal transplant recipients: a single unit experience. Nephrology (Carlton) 9(6): 418-421.
- Joss N, Rodger RS, McMillan MA, Junor BJ (2007) Randomized study comparing cyclosporine with azathioprine one year after renal transplantation- 15-year outcome data. Transplantation 83(5): 582-587.
- Stoves J, Newstead CG, Baczkowski AJ, Owens G, Paraoan M, et al. (2004) A randomized controlled trial of immunosuppression conversion for the treatment of chronic allograft nephropathy. Nephrol Dial Transplant 19(8): 2113-2120.
- Pascual J, Segoloni G, Gonzalez Molina M, del Castillo D, Capdevila L, et al. (2003) Comparison between a two-drug regimen with tacrolimus and steroids and a triple one with azathioprine in kidney transplantation: results of a European trial with 3-year follow up. Transplant Proc 35(5): 1701- 1703.
- Hou S (2013) Pregnancy in renal transplant recipients. Adv Chronic Kidney Dis. 20(3): 253-259.
- Borel JF (1986) Ciclosporin and its future. Prog Allergy 38: 9-18.
- Kahan BD (1985) Cyclosporine: the agent and its actions. Transplant Proc 17(4 Suppl 1): 5-18.
- Calne RY, Rolles K, White DJ, Thiru S, Evans DB, et al. (1979) Cyclosporin A initially as the only immunosuppressant in 34 recipients of cadaveric organs: 32 kidneys, 2 pancreases, and 2 livers. Lancet 2(8151): 1033-1036.
- Calne RY, Thiru S, McMaster P, Craddock GN, White DJ, et al. (1998) Cyclosporin A in patients receiving renal allografts from cadaver donors. 1978. J Am Soc Nephrol. 9(9): 1751-1756.
- Brennan DC, Barbeito R, Burke J, Brayman K, Greenstein S, et al. (1999) Safety of Neoral conversion in maintenance renal transplant patients: A oneyear, double-blind study. NOVARTIS OLN-353 Study Group. Kidney Int 56(2): 685-691.
- Tisone G, Orlando G, Mercadante E, Vennarecci G, Pisani F, et al. (1998) Neoral versus Sandimmune in kidney transplantation. Transplant Proc 30(5): 1749-1750.
- Frei UA, Neumayer HH, Buchholz B, Niese D, Mueller EA (1998) Randomized, double-blind, one-year study of the safety and tolerability of cyclosporine microemulsion compared with conventional cyclosporine in renal transplant patients. International Sandimmun Neoral Study Group. Transplantation 65(11): 1455-1460.
- Khatami SM, Taheri S, Azmandian J, Sagheb MM, Nazemian F, et al. (2013) One-Year Multicenter Double-Blind Randomized Clinical Trial on the Efficacy and Safety of Generic Cyclosporine (Iminoral) in De Novo Kidney Transplant Recipients. Exp Clin Transplant.
- Niemczyk M, Paczek L (2011) Generic formulation of Cyclosporine A, Equoral(R), in de novo kidney transplant recipients: five-year follow-up. Ann Transplant 16(2): 59-62.
- Knight SR, Morris PJ (2007) The clinical benefits of cyclosporine C2-level monitoring: a systematic review. Transplantation 83(12): 1525-1535.
- Canadian Neoral Renal Transplantation Study Group (2001) Absorption profiling of cyclosporine microemulsion (neoral) during the first 2 weeks after renal transplantation. Transplantation 72(6): 1024-1032.
- Kyllonen LE, Salmela KT (2006) Early cyclosporine C0 and C2 monitoring in de novo kidney transplant patients: a prospective randomized singlecenter pilot study. Transplantation 81(7): 1010-1015.
- Rosenthal JT, Hakala TR, Iwatsuki S, Shaw BW Jr, Starzl TE (1983) Cadaveric renal transplantation under cyclosporine-steroid therapy. Surg Gynecol Obstet 157(4): 309-315.
- A randomized clinical trial of cyclosporine in cadaveric renal transplantation (1983) N Engl J Med 309(14): 809-815.
- Calne RY, Wood AJ (1985) Cyclosporin in cadaveric renal transplantation: 3-year follow-up of a European multicentre trial. Lancet 2(8454): 549.
- Ferguson RM, Rynasiewicz JJ, Sutherland DE, Simmons RL, Najarian JS (1982) Cyclosporin A in renal transplantation: a prospective randomized trial. Surgery 92(2): 175-182.
- Opelz G (1986) Multicenter impact of ciclosporin on cadaver kidney graft survival. Prog Allergy 38: 329-345.
- Ponticelli C, Minetti L, Di Palo FQ, Vegeto A, Belli L, et al. (1988) The Milan clinical trial with cyclosporine in cadaveric renal transplantation. A three-year follow-up. Transplantation 45(5): 908-913.
- Lindholm A, Albrechtsen D, Tufveson G, Karlberg I, Persson NH, et al. (1992) A randomized trial of cyclosporine and prednisolone versus cyclosporine, azathioprine, and prednisolone in primary cadaveric renal transplantation. Transplantation 54(4): 624-631.
- Ponticelli C, Tarantino A, Montagnino G, Aroldi A, Banfi G, et al. (1988) A randomized trial comparing triple-drug and double-drug therapy in renal transplantation. Transplantation 45(5): 913-918.
- Shah S, Collett D, Johnson R, Thuraisingham RC, Raftery MJ, et al. (2006) Long-term graft outcome with mycophenolate mofetil and azathioprine: A paired kidney analysis. Transplantation 82(12): 1634-1639.
- Simmons RL, Canafax DM, Fryd DS, Ascher NL, Payne WD, et al. (1986) New immunosuppressive drug combinations for mismatched related and cadaveric renal transplantation. Transplant Proc 18(2 Suppl 1): 76-81.
- Vincenti F, Kirkman R, Light S, Bumgardner G, Pescovitz M, et al. (1998) Interleukin-2-receptor blockade with daclizumab to prevent acute rejection in renal transplantation. Daclizumab Triple Therapy Study Group. N Engl J Med 338(3): 161-165.
- Naesens M, Kuypers DR, Sarwal M (2009) Calcineurin inhibitor nephrotoxicity. Clin J Am Soc Nephrol 4(2): 481-508.
- Claes K, Meier-Kriesche HU, Schold JD, Vanrenterghem Y, Halloran PF, et al. (2012) Effect of different immunosuppressive regimens on the evolution of distinct metabolic parameters: evidence from the Symphony study. Nephrol Dial Transplant 27(2): 850-857.
- Solez K, Vincenti F, Filo RS (1998) Histopathologic findings from 2-year protocol biopsies from a U.S. multicenter kidney transplant trial comparing tarolimus versus cyclosporine: a report of the FK506 Kidney Transplant Study Group. Transplantation 66(12): 1736-1740.
- Rowshani AT, Scholten EM, Bemelman F, Eikmans M, Idu M, et al. (2006) No difference in degree of interstitial Sirius red-stained area in serial biopsies from area under concentration-over-time curves-guided cyclosporine versus tacrolimus-treated renal transplant recipients at one year. J Am Soc Nephrol 17(1): 305-312.
- Pirsch JD, Miller J, Deierhoi MH, Vincenti F, Filo RS (1997) A comparison of tacrolimus (FK506) and cyclosporine for immunosuppression after cadaveric renal transplantation. FK506 Kidney Transplant Study Group. Transplantation 63(7): 977-983.
- Johnson C, Ahsan N, Gonwa T, Halloran P, Stegall M, et al. (2000) Randomized trial of tacrolimus (Prograf ) in combination with azathioprine or mycophenolate mofetil versus cyclosporine (Neoral) with mycophenolate mofetil after cadaveric kidney transplantation. Transplantation 69(5): 834- 841.
- Gonwa T, Mendez R, Yang HC, Weinstein S, Jensik S, et al. (2003) Randomized trial of tacrolimus in combination with sirolimus or mycophenolate mofetil in kidney transplantation: results at 6 months. Transplantation 75(8): 1213-1220.
- Shapiro R, Jordan ML, Scantlebury VP, Vivas C, Marsh JW, et al. (1999) A prospective, randomized trial of tacrolimus/prednisone versus tacrolimus/ prednisone/mycophenolate mofetil in renal transplant recipients. Transplantation 67(3): 411-415.
- Webster AC, Woodroffe RC, Taylor RS, Chapman JR, Craig JC (2005) Tacrolimus versus ciclosporin as primary immunosuppression for kidney transplant recipients: meta-analysis and meta-regression of randomised trial data. BMJ 331(7520): 810.
- Jurewicz WA (2003) Tacrolimus versus cyclosporin immunosuppression: long-term outcome in renal transplantation. Nephrol Dial Transplant 18(Suppl 1): i7-11.
- Kaplan B, Schold JD, Meier-Kriesche HU (2003) Long-term graft survival with neoral and tacrolimus: a paired kidney analysis. J Am Soc Nephrol 14(11): 2980-2984.
- Vincenti F, Friman S, Scheuermann E, Rostaing L, Jenssen T, et al. (2007) Results of an international, randomized trial comparing glucose metabolism disorders and outcome with cyclosporine versus tacrolimus. Am J Transplant 7(6): 1506-1514.
- Jordan ML, Shapiro R, Vivas CA, Scantlebury VP, Rhandhawa P, et al. (1994) FK506 "rescue" for resistant rejection of renal allografts under primary cyclosporine immunosuppression. Transplantation 57(6): 860-865.
- Jordan ML, Shapiro R, Jensen CW, Scantlebury V, Fung J, et al. (1991) FK 506 conversion of renal allografts failing cyclosporine immunosuppression. Transplant Proc 23(6): 3078-3081.
- Jordan ML, Naraghi R, Shapiro R, Smith D, Vivas CA, et al. (1997) Tacrolimus rescue therapy for renal allograft rejection--five-year experience. Transplantation 63(2): 223-228.
- Margreiter R, Pohanka E, Sparacino V, Sperschneider H, Kunzendorf U, et al. (2005) Open prospective multicenter study of conversion to tacrolimus therapy in renal transplant patients experiencing ciclosporin-related sideeffects. Transpl Int 18(7): 816-823.
- Ekberg H, Tedesco-Silva H, Demirbas A, Vitko S, Nashan B, et al. (2007) Reduced exposure to calcineurin inhibitors in renal transplantation. N Engl J Med 357(25): 2562-2575.
- Ekberg H, Bernasconi C, Tedesco-Silva H, Vitko S, Hugo C, et al. (2009) Calcineurin inhibitor minimization in the Symphony study: observational results 3 years after transplantation. Am J Transplant 9(8): 1876-1885.
- Butler JA, Roderick P, Mullee M, Mason JC, Peveler RC (2004) Frequency and impact of nonadherence to immunosuppressants after renal transplantation: a systematic review. Transplantation 77(5): 769-776.
- McCormack PL (2014) Extended-release tacrolimus: a review of its use in de novo kidney transplantation. Drugs 74(17): 2053-2064.
- Caillard S, Moulin B, Buron F, Mariat C, Audard V, et al. (2015) Advagraf®, a once-daily prolonged release tacrolimus formulation, in kidney transplantation: literature review and guidelines from a panel of experts. Transpl Int
- Guirado L, Cantarell C, Franco A, Huertas EG, Fructuoso AS, et al. (2011) Efficacy and safety of conversion from twice-daily to once-daily tacrolimus in a large cohort of stable kidney transplant recipients. Am J Transplant 11(9): 1965-1971.
- Fulton B, Markham A (1996) Mycophenolate mofetil. A review of its pharmacodynamic and pharmacokinetic properties and clinical efficacy in renal transplantation. Drugs 51(2): 278-298.
- Sollinger HW, Sundberg AK, Leverson G, Voss BJ, Pirsch JD (2010) Mycophenolate mofetil versus enteric-coated mycophenolate sodium: a large, single-center comparison of dose adjustments and outcomes in kidney transplant recipients. Transplantation 89(4): 446-451.
- Schrama YC, Joles JA, van Tol A, Boer P, Koomans HA, et al. (2000) Conversion to mycophenolate mofetil in conjunction with stepwise withdrawal of cyclosporine in stable renal transplant recipients. Transplantation 69(3): 376-383.
- Knight SR, Russell NK, Barcena L, Morris PJ (2009) Mycophenolate mofetil decreases acute rejection and may improve graft survival in renal transplant recipients when compared with azathioprine: a systematic review. Transplantation 87(6): 785-794.
- Ciancio G, Burke GW, Gaynor JJ, Mattiazzi A, Roth D, et al. (2004) A randomized long-term trial of tacrolimus and sirolimus versus tacrolimus and mycophenolate mofetil versus cyclosporine (NEORAL) and sirolimus in renal transplantation. I. Drug interactions and rejection at one year. Transplantation. 77(2): 244-251.
- Sollinger HW, Belzer FO, Deierhoi MH, Diethelm AG, Gonwa TA, et al. (1992) RS-61443 (mycophenolate mofetil). A multicenter study for refractory kidney transplant rejection. Ann Surg 216(4): 513-519.
- Dudley C, Pohanka E, Riad H, Dedochova J, Wijngaard P, et al. (2005) Mycophenolate mofetil substitution for cyclosporine a in renal transplant recipients with chronic progressive allograft dysfunction: the "creeping creatinine" study. Transplantation 79(4): 466-475.
- Schnuelle P, van der Heide JH, Tegzess A, Verburgh CA, Paul LC, et al. (2002) Open randomized trial comparing early withdrawal of either cyclosporine or mycophenolate mofetil in stable renal transplant recipients initially treated with a triple drug regimen. J Am Soc Nephrol 13(2): 536-543.
- Kreis H, Cisterne JM, Land W, Wramner L, Squifflet JP, et al. (2000) Sirolimus in association with mycophenolate mofetil induction for the prevention of acute graft rejection in renal allograft recipients. Transplantation 69(7): 1252-1260.
- Flechner SM, Goldfarb D, Modlin C, Feng J, Krishnamurthi V, et al. (2002) Kidney transplantation without calcineurin inhibitor drugs: a prospective, randomized trial of sirolimus versus cyclosporine. Transplantation 74(8): 1070-1076.
- Vincenti F, Charpentier B, Vanrenterghem Y, Rostaing L, Bresnahan B, et al. (2010) A phase III study of belatacept-based immunosuppression regimens versus cyclosporine in renal transplant recipients (BENEFIT study). Am J Transplant 10(3): 535-546.
- Grinyo JM, Gil-Vernet S, Cruzado JM, Caldes A, Riera L, et al. (2003) Calcineurin inhibitor-free immunosuppression based on antithymocyte globulin and mycophenolate mofetil in cadaveric kidney transplantation: results after 5 years. Transpl Int 16(11): 820-827.
- Pascual J, Galeano C, Royuela A, Zamora J (2010) A systematic review on steroid withdrawal between 3 and 6 months after kidney transplantation. Transplantation 90(4): 343-349.
- Glicklich D, Gupta B, Schurter-Frey G, Greenstein SM, Schechner RS, et al. (1998) Chronic renal allograft rejection: no response to mycophenolate mofetil. Transplantation 66(3): 398-399.
- Morales JM, Wramner L, Kreis H, Durand D, Campistol JM, et al. (2002) Sirolimus does not exhibit nephrotoxicity compared to cyclosporine in renal transplant recipients. Am J Transplant 2(5): 436-442.
- Lai JH, Tan TH (1994) CD28 signaling causes a sustained down-regulation of I kappa B alpha which can be prevented by the immunosuppressant rapamycin. J Biol Chem 269(48): 30077-30080.
- Terada N, Lucas JJ, Szepesi A, Franklin RA, Domenico J, et al. (1993) Rapamycin blocks cell cycle progression of activated T cells prior to events characteristic of the middle to late G1 phase of the cycle. J Cell Physiol 154(1): 7-15.
- Gregory CR, Huie P, Billingham ME, Morris RE (1993) Rapamycin inhibits arterial intimal thickening caused by both alloimmune and mechanical injury. Its effect on cellular, growth factor, and cytokine response in injured vessels. Transplantation 55(6): 1409-1418.
- Cao W, Mohacsi P, Shorthouse R, Pratt R, Morris RE (1995) Effects of rapamycin on growth factor-stimulated vascular smooth muscle cell DNA synthesis. Inhibition of basic fibroblast growth factor and platelet-derived growth factor action and antagonism of rapamycin by FK506. Transplantation 59(3): 390-395.
- Groth CG, Backman L, Morales JM, Calne R, Kreis H, et al. (1999) Sirolimus (rapamycin)-based therapy in human renal transplantation: similar efficacy and different toxicity compared with cyclosporine. Sirolimus European Renal Transplant Study Group. Transplantation 67(7): 1036-1042.
- Srinivas TR, Schold JD, Guerra G, Eagan A, Bucci CM, et al. (2007) Mycophenolate mofetil/sirolimus compared to other common immunosuppressive regimens in kidney transplantation. Am J Transplant 7(3): 586-594.
- Flechner SM, Glyda M, Cockfield S, Grinyo J, Legendre C, et al. (2011) The ORION study: comparison of two sirolimus-based regimens versus tacrolimus and mycophenolate mofetil in renal allograft recipients. Am J Transplant 11(8): 1633-1644.
- Webster AC, Lee VW, Chapman JR, Craig JC (2006) Target of rapamycin inhibitors (TOR-I; sirolimus and everolimus) for primary immunosuppression in kidney transplant recipients. Cochrane Database Syst Rev (2): CD004290.
- Watson CJ, Firth J, Williams PF, Bradley JR, Pritchard N, et al. (2005) A randomized controlled trial of late conversion from CNI-based to sirolimusbased immunosuppression following renal transplantation. Am J Transplant 5(10): 2496-2503.
- Schena FP, Pascoe MD, Alberu J, del Carmen Rial M, Oberbauer R, et al. (2009) Conversion from calcineurin inhibitors to sirolimus maintenance therapy in renal allograft recipients: 24-month efficacy and safety results from the CONVERT trial. Transplantation 87(2): 233-242.
- Guerra G, Ciancio G, Gaynor JJ, Zarak A, Brown R, et al. (2011) Randomized trial of immunosuppressive regimens in renal transplantation. J Am Soc Nephrol 22(9): 1758-1768.
- Tedesco Silva H Jr, Cibrik D, Johnston T, Lackova E, Mange K, et al. (2010) Everolimus plus reduced-exposure CsA versus mycophenolic acid plus standard-exposure CsA in renal-transplant recipients. Am J Transplant 10(6): 1401-1413.
- Salvadori M, Scolari MP, Bertoni E, Citterio F, Rigotti P, et al. (2009) Everolimus with very low-exposure cyclosporine a in de novo kidney transplantation: a multicenter, randomized, controlled trial. Transplantation 88(10): 1194-1202.
- Pascual J, Srinivas TR, Chadban S, Citterio F, Oppenheimer F, et al. (2014) TRANSFORM: a novel study to design to evaluate the effect of everolimus on long-term outcomes after kidney transplantation. Open Access J Clin Trials 6: 45-54.
- Montagnino G, Sandrini S, Iorio B, Schena FP, Carmellini M, et al. (2008) A randomized exploratory trial of steroid avoidance in renal transplant patients treated with everolimus and low-dose cyclosporine. Nephrol Dial Transplant 23(2): 707-714.
- Mjornstedt L, Sorensen SS, von Zur Muhlen B, Jespersen B, Hansen JM, et al. (2015) Renal function three years after early conversion from a calcineurin inhibitor to everolimus: results from a randomized trial in kidney transplantation. Transpl Int 28(1): 42-51.
- Mjornstedt L, Sorensen SS, von Zur Muhlen B, Jespersen B, Hansen JM, et al. (2012) Improved renal function after early conversion from a calcineurin inhibitor to everolimus: a randomized trial in kidney transplantation. Am J Transplant 12(10): 2744-2753.
- Chadban SJ, Eris JM, Kanellis J, Pilmore H, Lee PC, et al. (2014) A randomized, controlled trial of everolimus-based dual immunosuppression versus standard of care in de novo kidney transplant recipients. Transpl Int 27(3): 302-311.
- Budde K, Lehner F, Sommerer C, Reinke P, Arns W, et al. (2015) Fiveyear outcomes in kidney transplant patients converted from cyclosporine to everolimus: the randomized ZEUS study. Am J Transplant 15(1): 119-128.
- Budde K, Becker T, Arns W, Sommerer C, Reinke P, et al. (2011) Everolimus- based, calcineurin-inhibitor-free regimen in recipients of de-novo kidney transplants: an open-label, randomised, controlled trial. Lancet 377(9768): 837-847.
- Budde K, Rath T, Sommerer C, Haller H, Reinke P, et al. (2015) Renal, efficacy and safety outcomes following late conversion of kidney transplant patients from calcineurin inhibitor therapy to everolimus: the randomized APOLLO study. Clin Nephrol 83(1): 11-21.
- Holdaas H, Rostaing L, Seron D, Cole E, Chapman J, et al. (2011) Conversion of long-term kidney transplant recipients from calcineurin inhibitor therapy to everolimus: a randomized, multicenter, 24-month study. Transplantation 92(4): 410-418.
- Chiurchiu C, Carreno CA, Schiavelli R, Petrone H, Balaguer C, et al. (2010) Results of the conversion to everolimus in renal transplant recipients with posttransplantation malignancies. Transplant Proc 42(1): 277-279.
- Cosimi AB, Wortis HH, Delmonico FL, Russell PS (1976) Randomized clinical trial of antithymocyte globulin in cadaver renal allograft recipients: importance of T cell monitoring. Surgery 80(2): 155-163.
- Streem SB, Novick AC, Braun WE, Steinmuller D, Greenstreet R (1983) Low-dose maintenance prednisone and antilymphoblast globulin for the treatment of acute rejection. A steroid-sparing approach to immunosuppressive therapy. Transplantation 35(5): 420-424.
- Cecka JM, Gjertson D, Terasaki PI (1993) Do prophylactic antilymphocyte globulins (ALG and OKT3) improve renal transplant survival in recipient and donor high-risk groups? Transplant Proc 25(1 Pt 1): 548-549.
- Goggins WC, Pascual MA, Powelson JA, Magee C, Tolkoff-Rubin N, et al. (2003) A prospective, randomized, clinical trial of intraoperative versus postoperative Thymoglobulin in adult cadaveric renal transplant recipients. Transplantation 76(5): 798-802.
- Vilalta R, Lara E, Madrid A, Chocron S, Vazquez A, et al. (2009) Delayed graft function is reduced with antithymocyte globulin induction in pediatric kidney transplantation. Transplant Proc 41(6): 2373-2375.
- Shaffer D, Langone A, Nylander WA, Goral S, Kizilisik AT, et al. (2003) A pilot protocol of a calcineurin-inhibitor free regimen for kidney transplant recipients of marginal donor kidneys or with delayed graft function. Clin Transplant 17(Suppl 9): 31-34.
- Sumrani N, Hong JH, DiBenedetto A, Clayton R, Miles AM, et al. (1996) Comparison between three different antilymphocyte induction protocols in renal transplant recipients with delayed graft function. Transplant Proc 28(1): 400-401.
- Thiyagarajan UM, Ponnuswamy A, Bagul A (2013) Thymoglobulin and its use in renal transplantation: a review. Am J Nephrol 37(6): 586-601.
- Pilch NA, Taber DJ, Moussa O, Thomas B, Denmark S, et al. (2014) Prospective randomized controlled trial of rabbit antithymocyte globulin compared with IL-2 receptor antagonist induction therapy in kidney transplantation. Ann Surg 259(5): 888-893.
- Liu Y, Zhou P, Han M, Xue CB, Hu XP, et al. (2010) Basiliximab or antithymocyte globulin for induction therapy in kidney transplantation: a metaanalysis. Transplant Proc 42(5): 1667-1670.
- Brokhof MM, Sollinger HW, Hager DR, Muth BL, Pirsch JD, et al. (2014) Antithymocyte globulin is associated with a lower incidence of de novo donor- specific antibodies in moderately sensitized renal transplant recipients. Transplantation 97(6): 612-617.
- Webster AC, Pankhurst T, Rinaldi F, Chapman JR, Craig JC (2006) Monoclonal and polyclonal antibody therapy for treating acute rejection in kidney transplant recipients: a systematic review of randomized trial data. Transplantation 81(7): 953-965.
- Vigeral P, Chkoff N, Chatenoud L, Campos H, Lacombe M, et al. (1986) Prophylactic use of OKT3 monoclonal antibody in cadaver kidney recipients. Utilization of OKT3 as the sole immunosuppressive agent. Transplantation 41(6): 730-733.
- Cosimi AB, Burton RC, Colvin RB, Goldstein G, Delmonico FL, et al. (1981) Treatment of acute renal allograft rejection with OKT3 monoclonal antibody. Transplantation 32(6): 535-539.
- Chatenoud L, Ferran C, Bach JF (1991) Clinical applications of anti-T-cell monoclonal antibodies. Adv Nephrol Necker Hosp 20: 281-304.
- Mariat C, Alamartine E, Diab N, de Filippis JP, Laurent B, et al. (1998) A randomized prospective study comparing low-dose OKT3 to low-dose ATG for the treatment of acute steroid-resistant rejection episodes in kidney transplant recipients. Transpl Int 11(3): 231-236.
- Patschan D, Kribben A, Pietruck F, Lutz J, Binek M, et al. (2006) OKT3 therapy in addition to tacrolimus is associated with improved long-term function in patients with steroid refractory renal allograft rejection. Nephron Clin Pract 103(3): c94-99.
- Baan CC, van Riemsdijk-Overbeeke IC, Boelaars-van Haperen MJ, IJzermans JM, Weimar W (2002) Inhibition of the IL-15 pathway in anti-CD25 mAb treated renal allograft recipients. Transpl Immunol 10(1): 81-87.
- Ponticelli C, Yussim A, Cambi V, Legendre C, Rizzo G, et al. (2001) A randomized, double-blind trial of basiliximab immunoprophylaxis plus triple therapy in kidney transplant recipients. Transplantation 72(7): 1261-1267.
- Aktas S, Colak T, Baskin E, Sevmis S, Ozdemir H, et al. 2011) Comparison of basiliximab and daclizumab with triple immunosuppression in renal transplantation. Transplant Proc 43(2): 453-457.
- Nashan B, Moore R, Amlot P, Schmidt AG, Abeywickrama K, et al. (1997) Randomised trial of basiliximab versus placebo for control of acute cellular rejection in renal allograft recipients. CHIB 201 International Study Group. Lancet 350(9086): 1193-1198.
- Webster AC, Playford EG, Higgins G, Chapman JR, Craig JC (2004) Interleukin 2 receptor antagonists for renal transplant recipients: a meta-analysis of randomized trials. Transplantation 77(2): 166-176.
- Brennan DC, Daller JA, Lake KD, Cibrik D, Del Castillo D, et al. (2006) Rabbit antithymocyte globulin versus basiliximab in renal transplantation. N Engl J Med 355(19): 1967-1977.
- Noel C, Abramowicz D, Durand D, Mourad G, Lang P, et al. (2009) Daclizumab versus antithymocyte globulin in high-immunological-risk renal transplant recipients. J Am Soc Nephrol 20(6): 1385-1392.
- Hale G (2001) The CD52 antigen and development of the CAMPATH antibodies. Cytotherapy 3(3): 137-143.
- Kirk AD, Hale DA, Mannon RB, Kleiner DE, Hoffmann SC, et al. (2003) Results from a human renal allograft tolerance trial evaluating the humanized CD52-specific monoclonal antibody alemtuzumab (CAMPATH-1H).Transplantation 76(1): 120-129.
- Cai J, Terasaki PI (2010) Induction immunosuppression improves longterm graft and patient outcome in organ transplantation: an analysis of United Network for Organ Sharing registry data. Transplantation 90(12): 1511-1515.
- Group CSC, Haynes R, Harden P, Judge P, Blackwell L, et al. (2014) Alemtuzumab-based induction treatment versus basiliximab-based induction treatment in kidney transplantation (the 3C Study): a randomised trial. Lancet 384(9955): 1684-1690.
- Morgan RD, O'Callaghan JM, Knight SR, Morris PJ (2012) Alemtuzumab induction therapy in kidney transplantation: a systematic review and metaanalysis. Transplantation. 93(12): 1179-1188.
- Hanaway MJ, Woodle ES, Mulgaonkar S, Peddi VR, Kaufman DB, et al.(2011) Alemtuzumab induction in renal transplantation. N Engl J Med 364(20): 1909-1919.
- Tanabe K, Ishida H, Inui M, Okumi M, Shirakawa H, et al. (2013) ABOincompatible kidney transplantation: long-term outcomes. Clin Transpl 307-312.
- Ejaz NS, Shields AR, Alloway RR, Sadaka B, Girnita AL, et al. (2013) Randomized controlled pilot study of B cell-targeted induction therapy in HLA sensitized kidney transplant recipients. Am J Transplant 13(12): 3142-3154.
- van den Hoogen MW, Kamburova EG, Baas MC, Steenbergen EJ, Florquin S, et al. (2015) Rituximab as induction therapy after renal transplantation: a randomized, double-blind, placebo-controlled study of efficacy and safety. Am J Transplant 15(2): 407-416.
- Fuchinoue S, Ishii Y, Sawada T, Murakami T, Iwadoh K, et al. (2011) The 5-year outcome of ABO-incompatible kidney transplantation with rituximab induction. Transplantation 91(8): 853-857.
- Riella LV, Safa K, Yagan J, Lee B, Azzi J, et al. (2014) Long-term outcomes of kidney transplantation across a positive complement-dependent cytotoxicity crossmatch. Transplantation 97(12): 1247-1252.
- Trappe R, Hinrichs C, Appel U, Babel N, Reinke P, et al. (2009) Treatment of PTLD with rituximab and CHOP reduces the risk of renal graft impairment after reduction of immunosuppression. Am J Transplant 9(10): 2331-2337.
- Said-Conti V, Amrolia PJ, Gaze MN, Stoneham S, Sebire N, et al. (2013) Successful treatment of central nervous system PTLD with rituximab and cranial radiotherapy. Pediatr Nephrol 28(10): 2053-2056.
- [183]. Larsen CP, Pearson TC, Adams AB, Tso P, Shirasugi N, et al. (2005) Rational development of LEA29Y (belatacept), a high-affinity variant of CTLA4-Ig with potent immunosuppressive properties. Am J Transplant 5(3): 443-453.
- Vincenti F, Larsen CP, Alberu J, Bresnahan B, Garcia VD, et al. (2012) Three-year outcomes from BENEFIT, a randomized, active-controlled, parallel-group study in adult kidney transplant recipients. Am J Transplant 12(1): 210-217.
- Charpentier B, Medina Pestana JO, Del CRM, Rostaing L, Grinyo J, et al. (2013) Long-term exposure to belatacept in recipients of extended criteria donor kidneys. Am J Transplant 13(11): 2884-2891.
- Durrbach A, Pestana JM, Pearson T, Vincenti F, Garcia VD, et al. (2010) A phase III study of belatacept versus cyclosporine in kidney transplants from extended criteria donors (BENEFIT-EXT study). Am J Transplant 10(3): 547-557.
- Vincenti F, Rostaing L, Grinyo J, Rice K, Steinberg S, et al. (2016) Belatacept and Long-Term Outcomes in Kidney Transplantation. N Engl J Med 374(4): 333-343.
- De Sousa-Amorim E, Revuelta I, Diekmann F, Cofan F, Lozano M, et al. (2015) Bortezomib for refractory acute antibody-mediated rejection in kidney transplant recipients. A single-center case series. Nephrology (Carlton).
- Wong NL, O'Connell P, Chapman JR, Nankivell B, Kable K, et al. (2015) Bortezomib in ABO-incompatible kidney transplant desensitization: a case report. Nephrology (Carlton). 20(Suppl 1): 22-24.
- Everly MJ, Terasaki PI, Trivedi HL (2012) Durability of antibody removal following proteasome inhibitor-based therapy. Transplantation 93(6): 572-577.
- Eskandary F, Bond G, Schwaiger E, Kikic Z, Winzer C, et al. (2014) Bortezomib in late antibody-mediated kidney transplant rejection (BORTEJECT Study): study protocol for a randomized controlled trial. Trials 15: 107.
- Yelken B, Arpali E, Gorcin S, Kocak B, Karatas C, et al. (2015) Eculizumab for Treatment of Refractory Antibody-Mediated Rejection in Kidney Transplant Patients: A Single-Center Experience. Transplant Proc 47(6): 1754-1759.
- Stevenson S, Mallett A, Oliver K, Hyland V, Hawley C, et al. (2014) Atypical HUS associated with severe, unexpected antibody-mediated rejection post kidney transplant. Nephrology (Carlton) 19(Suppl 1): 22-26.
- Stegall MD, Diwan T, Raghavaiah S, Cornell LD, Burns J, et al. (2011) Terminal complement inhibition decreases antibody-mediated rejection in sensitized renal transplant recipients. Am J Transplant 11(11): 2405-2413.
- Legendre C, Sberro-Soussan R, Zuber J, Rabant M, Loupy A, et al. (2013) Eculizumab in renal transplantation. Transplant Rev (Orlando) 27(3): 90-92.
- Vo AA, Zeevi A, Choi J, Cisneros K, Toyoda M, et al. (2015) A phase I/II placebo-controlled trial of C1-inhibitor for prevention of antibody-mediated rejection in HLA sensitized patients. Transplantation 99(2): 299-308.
- Viglietti D, Gosset C, Loupy A, Deville L, Verine J, et al. (2015) C1-Inhibitor in Acute Antibody-Mediated Rejection Non-Responsive to Conventional Therapy in Kidney Transplant Recipients: A Pilot Study. Am J Transplant.
- Budde K, Schmouder RL, Brunkhorst R, Nashan B, Lucker PW, et al. (2002) First human trial of FTY720, a novel immunomodulator, in stable renal transplant patients. J Am Soc Nephrol 13(4): 1073-1083.
- Budde K, Sommerer C, Becker T, Asderakis A, Pietruck F, et al. (2010) Sotrastaurin, a novel small molecule inhibiting protein kinase C: first clinical results in renal-transplant recipients. Am J Transplant 10(3): 571-581.
- Wojciechowski D, Vincenti F (2011) Targeting JAK3 in kidney transplantation: current status and future options. Curr Opin Organ Transplant 16(6):614-619.
- Vincenti F, Tedesco Silva H, Busque S, O'Connell P, Friedewald J, et al. (2012) Randomized phase 2b trial of tofacitinib (CP-690,550) in de novo kidney transplant patients: efficacy, renal function and safety at 1 year. Am J Transplant 12(9): 2446-2456.
- Heavner MS, Tichy EM, Yazdi M, Formica RN Jr, Kulkarni S, et al. (2013) Clinical outcomes associated with conversion from brand-name to generic tacrolimus in hospitalized kidney transplant recipients. Am J Health Syst Pharm 70(17): 1507-1512.
- Farney AC, Doares W, Kaczmorski S, Rogers J, Stratta RJ (2010) Cost-effective immunosuppressive options for solid organ transplantation: a guide to lower cost for the renal transplant recipient in the USA. Immunotherapy 2(6): 879-888.
- Molnar AO, Fergusson D, Tsampalieros AK, Bennett A, Fergusson N, et al. (2015) Generic immunosuppression in solid organ transplantation: systematic review and meta-analysis. BMJ 350: h3163.





