Dichorio-Triamniotic Triplet Pregnancy after Day 3 Single Embryo Transfer
Gala A1*, Vintejoux E2*, Scalici E1, Ferrieres A1, Bringer-Deutsch S2, Vincens C2, Loup V1, Brunet C2, Boulot P2, Anahory T2, Hamamah S1**
1 CHRU Arnaud de Villeneuve, ART Department, INSERM U 1203, Montpellier, France.
2 CHRU Arnaud de Villeneuve, ART Department, Gynecology-Obstetric Department, Montpellier, France.
* Equal work
*Corresponding Author
Hamamah S,
Service de Biologie de la Reproduction,
CHRU Montpellier, INSERM U 1203,
Montpellier, France.
Tel: 003367336404
E-mail: s-hamamah@chu-montpellier.fr
Received: November 27, 2015; Accepted: December 22, 2015; Published: January 04, 2016
Citation: Hamamah S, et al., (2016) Dichorio-Triamniotic Triplet Pregnancy after Day 3 Single Embryo Transfer. Int J Reprod Fertil Sex Health, S1:002, 09-11. doi: dx.doi.org/10.19070/2377-1887-SI01002
Copyright: Hamamah S© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A 31 year-old woman had a single embryo transfer on day 3 after assisted hatching (AH) and intracytoplasmic sperm injection (ICSI) treatment. Ultrasound examination performed 6 weeks after oocyte retrieval revealed a triplet pregnancy combining monochorionic diamniotic twins and a singleton. If zygote splitting resulting in monochorionic triamniotic triplets following IVF has already been described, this case is about an incredibly rare phenomenon after single embryo transfer. Naturally, a concurrent spontaneous conception cannot be excluded. To our knowledge, this is the first time a dichorionic triplet pregnancy after single embryo transfer is reported.
2.Introduction
3.Case Presentation
4.Discussion
5.References
Keywords
Triplet Pregnancy; Dichorio-Triamniotic; Single Embryo Transfer; Assisted Hatching; Concurrent Natural Conception.
Introduction
Multiple births are associated with higher risk of obstetrical and perinatal complications, such as pre-eclampsia, preterm delivery and low birth weight. A great concern has been made about multiple pregnancies these last years in ART (assisted reproductive technology). In France, the mean number of transferred embryos has dramatically decreased over the last 10 years. The French biomedicine agency reports a drop from 1,88 to 1,79 between 2008 and 2011. Furthermore, more and more single embryo transfers are performed (+ 6% over the past 4 years) [1].
However, single embryo transfer cannot prevent from monozygotic (MZ) twins. Patients undergoing IVF/ICSI are at higher risk to have MZ twins compared with general population (among 5% versus less than 1%).
In natural conception, the type of twinning depends on the moment it originates. Diamniotic dichorionic MZ twins result from an early splitting on the first days of development, creating two distinct blastocysts with each an inner cell mass (ICM) and a cavity. Diamniotic monochorionic MZ twins, more frequent, originate later and result from two inner cell masses included in a unique blastocoel [2].
In ART, various procedures have been associated with this splitting risk, such as AH or late embryo stage transfer. The type of chorionicity is correlated with the technique used: day 3 AH provides more dichorionic MZ twins, whereas extended culture and advanced embryonic stage transfer is linked to more monochorionic MZ twins [3].
Moreover, when natural conception is possible, the risk of DZ twins cannot be excluded even after single embryo transfer.
About twenty cases of monochorionic triamniotic triplets after IVF have been reported in the literature and a few cases of DZ twins after single embryo transfer have already been published.
This paper relates the first case report about non monochorionic triplet pregnancy after single embryo transfer.
Case Presentation
A nulliparous young woman presented at our ART center with five years of infertility history. She was 31 years old and her partner 28. Day 3 hormonal biomarkers of ovarian reserve, ovulation, tubal patency evaluation (hysterosalpingography) and husband’s sperm analysis showed no abnormalities. They had three unsuccessful intrauterine insemination (IUI) cycles in a previous IVF center.
The couple was then referred to our ART center. The unexplained infertility led to a laparoscopy. An endometriosis stage II according to revised American Fertility Society classification [4] was diagnosed and completely treated by surgery. Six months later, as no spontaneous pregnancy occurred, the couple was planned for IVF.
A standard long Gn-RH agonist protocol was chosen for the first attempt. Unfortunately, the stimulation did not begin because of persistent ovarian cyst and poor endometrial quality. Four months later, a controlled ovarian stimulation (COS) with a Gn-RH antagonist protocol was started. The patient received 150 UI of recombinant FSH (Gonal F®, Merck Serono) during five days followed by 125 UI during four days. On the 6th day, antagonist was introduced (Orgalutran 0.25 mg/0.5 ml, MSD). On day 9 of COS, 5 follicles had reached 17 mm diameter and 3 were 15mm, E2 level was 1124 ng/mL and endometrium thickness was 10 mm; the ovulation was then triggered with recombinant hCG (Ovitrelle®, Merck Serono). Transvaginal ultrasound guided egg retrieval was performed 36 h later. We yielded 11 oocytes and 8 metaphase II oocytes were injected by ICSI and cultured individually (G-1TM PLUS, Vitrolife). ICSI was performed rather than conventional IVF because of a moderate asthenozoospermia at the day of the oocytes retrieval. We obtained 4 embryos. On day 3, a top quality embryo, with 8 regular cells and no fragmentation, was transferred after laser pulse AH for thick zona pellucida. Embryo transfer was ultrasound guided and performed with a soft catheter (Inventcath eco®, CCD). Luteal phase support begun on the pick up day and consisted in 15 days of vaginal micronized progesterone (600 mg/day). One blastocyst was cryopreserved on day 6 after prolonged culture. The two remaining embryos were discarded as they didn’t reach the blastocyst stage.
Two weeks after oocyte retrieval, the bhCG serum level was 251 UI. A second blood test at 48 hours confirmed the ongoing pregnancy with 626 UI. Ultrasound examination performed 6 weeks later showed a triplet pregnancy combining monochorionic diamniotic twins plus a singleton. Each fetus had a cardiac activity and normal biometry and morphology.
Because of the unexpected triplet pregnancy after single embryo transfer, the couple was asked if they had unprotected intercourse between egg retrieval and embryo transfer, which they confirmed. To improve perinatal issues, the couple was counseled to undergo a selective fetal reduction. Reduction of the twins has been preferred because of the superior risk of a monochorionic diamniotic pregnancy in comparison with a single pregnancy. The reduction was done at 10 weeks of pregnancy by selective intracardiac administration of KCL. The procedure was not complicated and to date, the pregnancy is still ongoing.
Discussion
ART is associated with higher multiple pregnancy risk, despite the reduction of the number of embryo transferred. According to Vitthala’s meta-analysis, there is at least a 2-fold rise in the incidence of monozygotic twinning after ART compared with natural conception [5].
Several techniques have been thought to enhance the risk of zygote splitting, such as AH. AH is used to thin zona pellucida and thus favor embryo eclosion and implantation. A very recent retrospective study significantly links AH to twin and triplet pregnancy [6]. These results confirm data previously published in the Cochrane database in 2012 [7]. The patients we discuss here did benefit from AH by laser pulse prior to transfer. We also have to note that we used the ICSI technique for fertilization. However, the effect of ICSI treatment on MZ twinning is very controversial [8].
In the case we present here, a triplet pregnancy occurred after a single embryo transfer to a young woman with unexplained infertility.
One hypothesis could be a two-steps zygote splitting: an early division leading to two distinct gestational sacs, followed by a second division in one of them creating monochorionic diamniotic twins plus a singleton. Nevertheless, in the present case, zygosity has not been assessed.
Guilherme et al. [9] studied zygosity and chorionicity in spontaneaous and IVF triplet pregnancies. On 31 sets of triplet obtained after ART, dichorioamniotic triplets were always DZ and trichorioamniotic triplets were almost always trizygotic (TZ).
Based on these data, the hypothesis of a concurrent spontaneous pregnancy seems to be more plausible.
We found four case reports (Table 1) in the literature mentioning DZ twinning after single embryo transfer [10-13]. Four patients had a late stage embryo transfer (morula or blastocyst) and only one an early cleavage-stage embryo transfer as in our case. Each time, natural conception was possible and couples attested having had unprotected intercourse during transfer period in four cases. As mentioned by Takehara et al. [11], there is indeed a possibility of spontaneous ovulation of the remaining oocytes after aspiration of follicles.
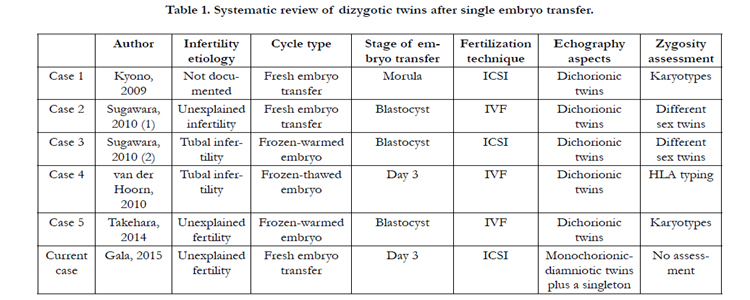

Table 1. Systematic review of dizygotic twins after single embryo transfer.
An interesting study on twin zygosity following single embryo transfer suggest that as many as 1 in 5 twins born after single embryo transfer (SET) may be the result of a concurrent natural conception [14]. Additionally, this phenomenon may be underestimated because same sex twins are too often wrongly considered as MZ twins. Genetic remains the only valid tool to assess zygosity.
Finally, the assumption of a transfer of two embryos instead of one has been considered. However, this probability was not retained because in our in vitro embryo culture system (individual micro drop), each embryo including supernumerary had his own follow up until day 6 (discarded or cryopreserved).
Again, to the best of our knowledge, our present case is the first about a dichorio-triamniotic triplet pregnancy after single embryo transfer.
We must caution that two quite similar phenomenons have been published in 2001 and 2003: two quadruplet pregnancies occurred after the transfer of two embryos and resulted in each case in four living babies with different zygosities [15, 16].
Here, we cannot assess the origin of each fetus, but the most likely hypothesis is that twins originate from the embryo transferred and the singleton from a concurrent natural conception.
Even if this is the first time we diagnose a triplet pregnancy after SET, we suggest that efforts to reduce multiple pregnancies in ART should include advices on avoiding intercourse during transfer period when natural conception is possible. Couple counseling might be improved about multiple pregnancy risk, because most of the patients are not aware of mother and fetal complications and expect above all the much-wanted pregnancy.
References
- Rapport médical et scientifique de l’assistance médicale à la procréation en France, 2012 www.agence-biomedecine.fr
- Corner GW (1955) The observed embryology of human single-ovum twins and other multiple births. Am J Obstet Gynecol 70(5): 933-951.
- Knopman JM, Krey LC, Oh C, Lee J, McCaffrey C, et al. (2014) What makes them split? Identifying risk factors that lead to monozygotic twins after in vitro fertilization. Fertil Steril 102(1): 82-89.
- Andrews WC, Buttram Jr VC, Behrman SJ, Carmichael E, Cohen M, et al. (1985) Revised American Fertility Society classication of endometriosis. Fertil Steril 43(3): 351-352.
- Vitthala S, Gelbaya TA, Brison DR, Fitzgerald CT, Nardo LG (2009) The risk of monozygotic twins after assisted reproductive technology: a systematic review and meta-analysis. Hum Reprod Update 15(1): 45-55.
- Jwa J, Jwa SC, Kuwahara A, Yoshida A, Saito H (2015) Risk of major congenital anomalies after assisted hatching: analysis of three-year data from the national assisted reproduction registry in Japan. Fertil Steril 104(1): 71-78.
- Carney SK, Das S, Blake D, Farquhar C, Seif MM, et al. (2012) Assisted hatching on assisted conception (in vitro fertilisation (IVF) and intracytoplasmic sperm injection (ICSI). Cochrane Database Syst Rev 12: CD001894.
- Wu D, Huang SY, Wu HM, Chen CK, Soong YK, et al. (2014) Monozygotic twinning after in vitro fertilization/intracytoplasmic sperm injection treatment is not related to advanced maternal age, intracytoplasmic sperm injection, assisted hatching, or blastocyst transfer. Taiwan J Obstet Gynecol 53(3): 324-329.
- Guilherme R, Drunat S, Delezoide AL, Oury JF, Luton D (2009) Zygosity and chorionicity in triplet pregnancies: new data. Hum Reprod 24(1): 100-105.
- Kyono K, Nakajo Y, Nishinaka C, Araki Y, Doshida M, et al. (2009) A birth of twins-one boy and one girl-from a single embryo transfer and a possible natural pregnancy. J Assist Reprod Genet 26(9-10): 553-554.
- Sugawara N, Fukuchi H, Maeda M, Komaba R, Araki Y (2010) Sex-discordant twins despite single embryo transfer: a report of two cases. Reprod Med Biol 9: 169-172.
- van der Hoorn ML, Helmerhorst F, Claas F, Scherjon S (2011) Dizygotic twin pregnancy after transfer of one embryo. Fertil Steril 95(2): 805.e1-3.
- Takehara I, Takahashi T, Hara S, Matsuo K, Igarashi H, Kurachi H (2014) Dizygotic twin pregnancy after single embryo transfer: a case report and review of the literature. J Assist Reprod Genet 31(4): 443-446.
- Osianlis T, Rombauts L, Gabbe M, Motteram C, Vollenhoven V (2014) Incidence and zygosity of twin births following transfers using a single fresh or frozen embryo. Hum Reprod 29(7): 1438-1443.
- Milki AA, Hinckley MD, Grumet FC, Chitkara U (2001) Concurrent IVF and spontaneous conception resulting in a quadruplet pregnancy. Hum Reprod 16(11): 2324-2326.
- Cahill DJ, Jenkins JM, Soothill PW, Whitelaw A, Wardle PG (2003) Quadruplet pregnancy following transfer of two embryos: case report. Hum Reprod 18(2): 441-443.





