The Relationship Between Sexual Dysfunction and Depression Levels in Women
Parpaee R*, Hosseini SA
Faculty of Literature/Psychology, Islamic Azad University, Kermanshah Branch, Kermanshah, Iran.
*Corresponding Author
Rozita Parpaee,
Faculty of Literature/Psychology, Islamic Azad University,
Kermanshah Branch, Kermanshah, 6718997551, Iran.
E-mail: r.parpaee@gmail.com
Received: February 01, 2017; Accepted: June 13, 2017; Published: June 14, 2017
Citation: Parpaee R, Hosseini SA (2017) The Relationship Between Sexual Dysfunction and Depression Levels in Women. Int J Reprod Fertil Sex Health. 4(4), 110-112. doi: dx.doi.org/10.19070/2377-1887-1700019
Copyright: Parpaee R© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Proper and healthy sexual function is regarded as a sign of mental and physical health and it is a cause of common sense pleasure, reinforcement of intimacy and reduction of tensions between couples and it will promote the person’s ability to cope with stress and life’s problems and suppress sexual impulses can cause emotional problems and impaired relationships that these issues can create different levels of depression in person. Thus, the purpose of this study was to investigate the relationship between sexual dysfunction and depression levels in those women who has gone to the clinics for consultation in Shiraz city. The research was descriptive and correlational. For this purpose 360 women who has gone to the clinics for consultation in Shiraz city were studied. The sample was selected by cluster sampling. The instruments used in this study were Female Sexual Function Index and the Beck Depression Inventory.In this survey, Pearson correlation coefficient parametric test was used. After data analysis results showed that there is significant relationship between sexual dysfunction and depression levels.
2.Introduction
3.Material and Method
4.Results and Discussions
5.Conclusion
6.References
Keywords
Sexual Dysfunction; Depression; Prevalence; Women.
Introduction
Healthy sexual function is one important aspect of married life and an important part of personal well-being that has an important role in enhancing the health and quality of life. And even can cause reduce depression and stress. Sexual health is a complex phenomenon and multilateral that influenced by biological, psychological, cultural and behavioral. In his regard, the world health organization is considered sexual health as a harmony of mind, emotions and body that leads to complete personality, communication and love. It should be considered that each of chronic disease can in turn lead to changes in the normal sexual response cycle and in many cases lead to sexual dysfunction in people. Although sexuality remains an important component of emotional and physical intimacy that most men and women desire to experience throughout their lives, it is unfortunately a topic many health care professionals have difficulty raising with their patients. Thus, it is not surprising that sexual dysfunction is a problem that is not well studied or discussed [1]. Many women experience issues related to sexual function in the sage of life [2]. The prevalence of sexual dysfunction among all women is estimated to be between 25% and 63% [1]. Female sexual dysfunction can occur at all stages of life and maybe happen continuous or from time to time. Therefore, any disorder that leading to disharmony and dissatisfaction with sex can cause sexual dysfunction [2]. Common disorders related to sexual dysfunction and increasing age include cardiovascular disease, diabetes, lower urinary tract symptoms, and depression [1]. Female sexual dysfunction is the most common problem in worldwide that influence on quality of life [3]. Female sexual dysfunction can arise by a range of factors that is different from person to person. Psychological, emotional, social and cultural factors that can cause sexual dysfunction are depression, functional anxiety and change in self- image and body image. The results of different studies in Iran shows that sexual dysfunction is common in women [4, 5] that based on sexual desire disorder and mental, physiological changes are as identifier sexual reaction cycle and has obvious distress and interpersonal problems [6, 7]. Faber present the effect of depression on sexual function in which, in women with increasing severity of depression, sexual dysfunction becomes greater. Sexual problems occur in adults of all ages and for any reason be raised different consequences will be followed and maybe cause problems such as anger and violence also lead to separation, divorce and depression [8]. So sexual problems according to stress or factors are involved in line with depression. Depression is one of the variables examined in sexual dysfunction especially in sexual desire disorder. Sexual dysfunction is cause and effect for mental problems [9]. Also suppress sexual impulses can cause emotional problems and impaired relationships that these issues can create different levels of depression in person [10]. In a study that conducted in order to assess the prevalence of sexual dysfunction and potential risk factors in 179 Turkish women (age of 18-66) 9/46 percent had sexual dysfunction. Evidence and research findings indicate that sexual disorders are very common and the large number of couples or people who experience these problems require urgent need to receive health services [11, 12].
The survey carried out by Pereira et al., (2013) about sexual dysfunctions has state that depression has a close relationship with female sexual dysfunctions so that in depressed women, hypoactive sexual desire disorder seems to be the most frequent dysfunction. In this study, in the comparison of single vs. married women, results were similar for anxiety, desire, and depression, with no statistically significant differences. In this study, depression was more prevalent in the single group [13].
Ackerman(1995) argues that sexual critical problem is the manifestation of the lack of medical interventions for sexual dysfunction. Thus, according to sexual function and its’ effect on public health this study investigates the relationship between sexual dysfunction and depression levels in those women who has gone to the clinics for consultation in shiraz city as a result of which better therapeutic- training planning in order to decrease harm [14].
Material and Method
The base of this study is descriptive-analytical. Statistical society included counseling clinics in ten areas of the city of Shiraz in 2015-2016. Individuals were selected by cluster sampling. So that each area a clinic was selected and from each clinic were selected about 36 individuals. According to statistical society the sample group is 360 individuals. In order to collect information sexual function questionnaire and the Beck depression inventory were used. The sexual function questionnaire is Female Sexual Function Index that the validity and reliability was approved previously and contains 19 item to distinguish patients with sexual dysfunction in healthy individuals and it had 6 options (I did not have sexual activity, never, rarely, sometimes, often, always) which was scored from 0 to 5. All points calculated were divided into low sexual function (0-3/33), average (4/33-6/66) and much (higher than 7/66). The Beck depression inventory is one of the best well-known test in determining depression [15]. It has 21 multiple- choice questions based on severity of depression which are graded from 0 to 3. According to grading, the score between 0 and 9 is normal and score 10 and more is depressed. So that is divided into Mild depression (10-19), Moderate (20-29), Severe (30-39) and Extreme (40 and more). In this study the assessment standard was correct answer to the questions in the questionnaire. After determining the level of sexual function and depression, the relationship between sexual function and depression was measured. To analyze the data, descriptive statistic and inferential statistic were used.
Results and Discussions
After collecting the questionnaires and extract data, the raw data were analyzed with SPSS software. To carry out the analysis, Pearson correlation coefficient parametric test was used. The findings show that 1/6 percent had low sexual function, 2/47 percent average and 7/46 percent much (Table 1).
The findings suggest that 58/7 percent were depressed women and 3/41 percent were non depressed (Table 2).
There is significant relationship between sexual dysfunction and depression levels (Table 3).
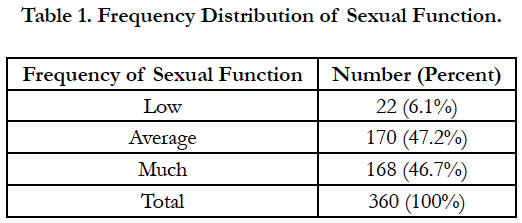

Table 1. Frequency Distribution of Sexual Function.
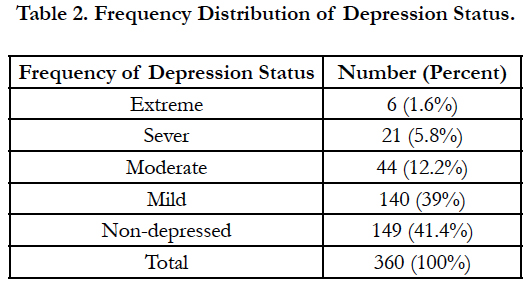
Table 2. Frequency Distribution of Depression Status.
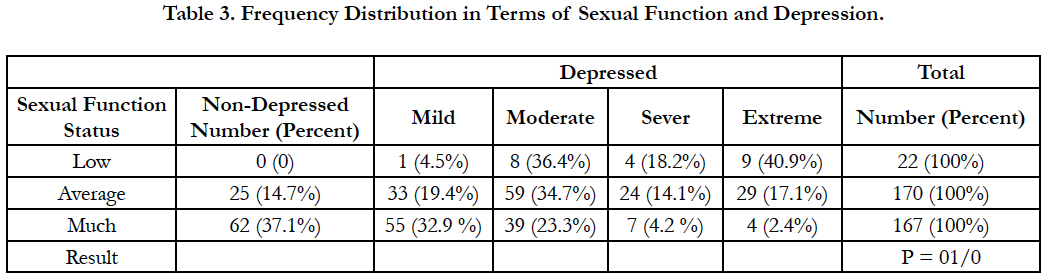
Table 3. Frequency Distribution in Terms of Sexual Function and Depression.
Conclusion
Sexual dysfunction can be a result of physical and mental problems. Tiredness, daily responsibilities, the role of multiple physical, individual psychological problems including depression and anxiety can affect a woman’s sexual function. Analysis of data showed almost less than half of women had high sexual function. Research results of Frotan et al., (2002) is consistent with the findings of this study. According to results this reveals the importance of providing the necessary information for girls at the age of marriage and providing a framework of religious, social and family values about relationships and sexual activity, and proper training about sex is strongly felt to women. Other findings of the present study was that more than half of women (58/7 percent) were depressed that 39 percent had mild depression. In a study Eldarabadi et al., (2002) did in order to assess the prevalence of depression in Zabol medical students the results showed that (3/63) percent of women were depressed. The present study has investigated the relationship between sexual dysfunction and depression levels in those women who has gone to the clinics for consultation in Shiraz city. Analysis of the data indicates that there is a significant relationship of chi-square between sexual dysfunction and depression levels. The results of this study is consistent with the results obtained by Faber (2012), Valeska (2013) [16, 17]. And expresses the relationship between sexual dysfunction and mental status of individuals. In other words, people with mental health problems have more sexual dysfunction. Boyed writes: A person usually in sexual dysfunction is suffering from low selfesteem and shame that is preoccupation and finally causes depression in person (Boyed, 2002). This study was conducted in a sample of women. It is suggested that sexual function be assessed in men that the results of which are used in educational and therapeutic programs. Training young couples understanding of sexuality and desires of each other and how to respond to it can be the main axis in premarital counseling. Discovering and solving sexual problems had significant results to improve the quality of the marital relationship that this is an important step toward the prevention of family conflict and its’ consequences. And due to the destructive effects of depression in personal and social life of people and to reduce depression in different social groups. It is suggested that direct and indirect support of training and consulting programs be promoted. And reports and scientific assessments are needed including longitudinal studies. Finally, sexual health should be considered women’s sexual health care, detection concerns and help them to improve function and sexual satisfaction the main axis of healthy family planning.
References
- Ambler D, Bieber E, Diamond M (2012) Sexual Function in Elderly Women: A Review of Current Literature. Rev Obestet Gynecol. 5 (1): 16-27.
- Afshari P, Nikbina M, Najar Sh, Haghighizadeh MH (2016) Determining some of the factors related to sexual function and satisfaction among wemen in Ahvaz.Eur J Pharma Med Res. 3(7): 445-450.
- Ghavan M (2004) Evaluation of the patient with sexual dysfunction referring to health clinic of Shahed university during the 9 months of year. Second Congress of Family and Sexual Problems Shahed University, Tehran.
- Goshtasbi A, Vahdaninia MS, Rahimiforooshani A (2005)Sexual dysfunction and its relationship with reproductive variables in Kohkiloyeh and Boyerahmad Province. Third Second Congress of Family and Sexual Problems. Shahed University, Tehran.
- Oahadi B (2004) Human sexual behavior. Isfahan: Sadegh Hedayat Press.
- Hallvorsen JG, Metz MF (1992) Sexual dysfunction, part II: Diagnostic, management, and prognostic. J Am BoardFam Pract. 5(2): 177-199.
- Kinzl JF, Mangweth B, Traweger C, Bibl W (1997) Sexual dysfunction in men and women: Significance of a dysfunctional family climate and Sexual abuse. J PsychotherPsychosom Med Psychol. 47(2): 41-45.
- Westheimer RK, Lopater S (2006) Human Sexuality: A Psychosocial Perspective. (2nd Edn), Lippincott Williams & Wilkins,Philadelpia, US.
- Frotan K, Jadidmilani M, Ghavam M (2002) Prevalence sexual dysfunction in divorce applicants refer to legal complex family. 2nd International congress on obstetrics and Gynecology. Shahed University, Tehran, Iran.
- Cayan S, Akbay E, Bozlu M (2004) The prevalence of female sexual dysfunction and potential risk factors that may impair sexual function in Turkish woman. Urol Int. 72(1): 52-7.
- Spence SH (1991) Psychosexual therapy: A cognitive behavioral approach. New York: Chapman & Hall.
- Weisberg KB, Brown TA, Wincze JP, Barlow DH (2001) Causal Attributions and male sexual arousal; the impact of attributions for a bogus erectile difficulty on sexual arousal, cognitions, and affect. J Abnorm Psychol. 110(2): 324-334.
- Pereira VM, Nardi AE, Silva AC (2013) Sexual dysfunction, depression, and anxiety in young women according to relationship status: an online survey. Trends Psychiatry Psychother. 35(1).
- Ackerman MD (1995) Introduction to the special section on contemporary issues in human sexuality: research and practice. J consult clin Psyhcol. 63(6): 859-61.
- Ildarabady E, Firouzkouhi MR, Mazloom S, Navinean A (2004) Prevalence of depression among students of Zabol Medical School. J Shahrekord Univ Med Sci. 6(2): 15-21.
- Sanchez IS, Liorca RG (1992) Psychophysiological and psychopathologic aspects associated with sexual dysfunction. Actas Luso Esp Neuvol Psiquiatr Ciene Afines. 20(6): 27-37.
- Alexander B (1993) Disorders of Sexual desire: diagnosis and treatment of decreased libido. Am Fam Physician. 47(4):832-861.
Indexed in





Total Visitors
Copyright © 2019 SciDoc Publishers. All Rights Reserved.
