Overweight and Obesity Among Primary School Children in Misurata City-Libya: Prevalence and Associated Risk Factors
Hussien AE*
Lecturer, Department of Community and Family Medicine, Faculty of Medicine, Misurata University, Libya.
*Corresponding Author
Hussien A. Elaswdi,
Lecturer, Department of Community and Family Medicine,
Faculty of Medicine, Misurata University, Libya.
Tel: 00218913783835
E-mail: hpharmacy92@yahoo.co.uk
Received: February 14, 2018; Accepted: March 09, 2018; Published: March 12, 2018
Citation: Hussien AE. Overweight and Obesity Among Primary School Children in Misurata City-Libya: Prevalence and Associated Risk Factors. Int J Pediat Health Care Adv. 2018;5(2):74-78. doi: dx.doi.org/10.19070/2572-7354-1800020
Copyright: Hussien AE© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Obesity is currently an escalating epidemic that affects many countries in the world where this condition is responsible for increasing death rates annually. This study was performed to find out the prevalence of overweight and obesity and associated risk factors in primary school children in Misurata city, Libya. Height and weight were measured in a sample of 1000 child aged between 6-11 years. Body mass index (BMI) was calculated for each child. Children were categorized according to age and specific percentile of BMI using 2000 CDC BMI - age growth charts. Information on possible risk factors was collected by questionnaire. The results showed that the prevalence of overweight and obesity 15.8% and 12.4% respectively. Viewing TV more than 2 hrs/day, physical exercise, child order and parent obesity were associated with overweight and obesity. In conclusion, prevalence of overweight and obesity primary school children in Misurata, Libya is high and aggressive preventive strategies should be implemented.
2.Introduction
3.Methods
3.1 Subjects and sample size
3.2 Procedure
3.3 Anthropometric Measurements
3.4 Questionnaire
3.5 Data analysis
4.Discussion
5.Conclusion
6.References
Keywords
Childhood Obesity; Risk Factors; Overweight; Primary School.
Introduction
The prevalence of obesity is increasing worldwide at an alarming rate in both developed and developing countries [1]. The current lack of consistency and agreement among different studies in the classification of overweight and obesity in children and adolescents makes it difficult to give an overview of the global prevalence of overweight and obesity in young age groups. Nevertheless, irrespective of the classification system used, most studies of overweight and obesity during childhood and adolescence have reported that the prevalence of both has increased.
Generally, excessive body weight during childhood influences the development of coronary heart disease, hypertension and stroke, type 2 diabetes mellitus, certain types of cancer, and other diseases in adulthood [2]. Life expectancy in developing countries has increased; however, the possibility of improving it will depend not only on a decrease in infant mortality, but also on a decrease in chronic non-transmissible diseases associated with premature mortality [3]. A decrease in the prevalence of overweight and obesity early in life could contribute towards achieving this goal. As widely demonstrated [1], it is possible to reduce the proportion of deaths due to chronic disease, and furthermore, prevent the occurrence of new cases by applying strategies directed to the modification of Lifestyle risk factors. Because of their public health importance, excessive body weight and obesity in childhood should be closely monitored. This offers the best hope for preventing progression of the disease and its associated morbidities in adulthood. The objective of the study was to evaluate the prevalence of overweight and obesity and associated risk factors in primary school children in Misurata city, Libya.
A Cross sectional study was conducted during the months of January and February, 2006 in Misurata city, Libya, on local primary schools (6-11 years old). Multistage cluster random sampling design was adopted. First clusters sample were obtained by drawing a simple random sample of congresses in Misurata city, two congresses were chosen from the center (Dat alremal and Shohadaa armylha) and three congresses were chosen from the suburbs (Algeran, Tomena and Gaser Ahammed). Then a list of schools in the five congresses was obtained from Misurata people's Committee of Education and 50% of primary schools were randomly selected from the list. The schools were selected with a probability proportional to the size. The total number of selected schools was 25 schools. Next, one class was selected from each grade in each of the 25 schools. Finally a list of students was obtained for each class, students were listed according to alphabetical order, and a number was assigned to every student on the list. This was followed by random selection of 20% of students from each grade. Each student had the same probability of being selected. If the student was absent, the next number on the list was picked. The sample size was calculated using an appropriate formula [4], to get the 384 children. A decision was made to include about 1000 children to decrease the error of sampling.
Permission for the study was obtained from the People’s Committee for Education and the People’s Committee for Health in Misurata. Consent to participate in the study was obtained from the head or principal of each school. Written parental consent was required for children to participate in the study.
Height and weight measurements were obtained according to the guidelines established by Lohman et al., [5]. Weight was measured without shoes and heavy outer clothing. Height was measured with the student shoeless and facing away from the scale. Standing height was measured to the nearest 0.1 cm, and weight was measured to the nearest 0.1 kg. Independent duplicate measurements were obtained for height and weight, and the average of both readings required to be within ± 0.5 cm or 0.5 kg, respectively was used in the data analyses. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Children were categorized according to age and specific percentile of BMI using 2000 CDC BMI - age growth chart [6], which has been adopted by World Health Organization (WHO) as the international anthropometrical reference [7]. Students between the 85th and 95th are categorized as overweight. At the 95th percentile and above, children were classified as obese.
The questionnaire covered information about (age, gender, birth order, birth weight, and breastfeeding practices), socioeconomic status (household and family size, parents level of education, parents occupation, family income, and area of residence) and behavioral factors, including fathers smoking status, physical exercise, sleeping patterns, number of hours spent on watching television. A brief medical history and family history of obesity were also recorded by asking the parents to describe themselves as obese or normal and to self report their weight and height, and then the parent BMI was calculated. This questionnaire was pilot tested in the field on 40 school children before the start of the study to get feedback from respondents. These 40 school children were not included in the study. During pilot testing, questionnaires underwent several modifications. The modified questionnaire was used to collect data. Self administered questionnaires, addressed to parents, were sent with students along with a cover letter explaining the purpose of the study. The parents of each selected child were asked to complete the questionnaire and to send it with their child to school, after they signed an informed consent form for agreement to participate in the study. In order to enhance more effective participation of parents to complete and return the questionnaire, the researcher broadcasted and advertised aspects of the study in the local radio station in Misurata city, which had a great effect on the response rate received.
The data obtained were entered into personal computer and the Statistical Package for the Social Sciences (SPSS) Version 13 was used for analysis and Software Epi-info 6.04 (Center for Disease Control and Prevention. GA, USA) was used for anthropometric analysis to calculate percentile BMI. Descriptive statistics using frequency distribution and analytical statistics using, chi-square, and t test were used. Multiple logistic regression analysis was used to examine factors associated with overweight and obesity in the study population. A p-value below or equal to 0.05 was considered to be statistically significant.
Results
Of the 1000 eligible children, the parents of 817 of them (81.7%) consented to their participation in the study. The sample consisted of 408 males and 409 females; 42.5% were aged 6 through 8 years and 57.5% were aged 9 through 11 years. Table 1 shows the demographic and socio economic characteristics of the study population. The prevalence of underweight, normal weight, overweight and obesity according to age is shown in graph 1. Multiple logistic regression analysis indicated that viewing TV more than 2 h/day, physical exercise, child order, and parent's obesity were significantly associated with child overweight and obesity after adjusting for age and sex, while father education was significantly associated with child obesity (Table 2).
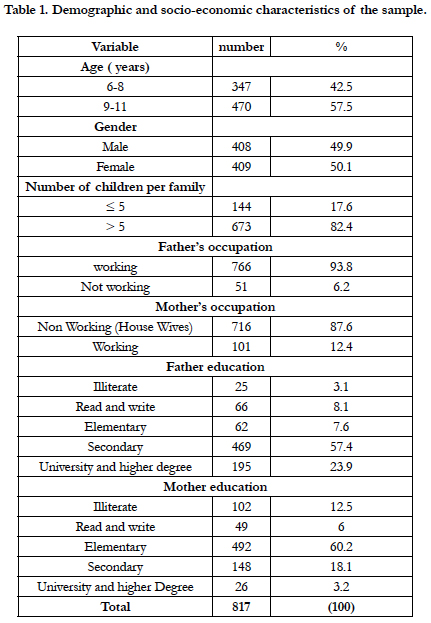

Table 1. Demographic and socio-economic characteristics of the sample.
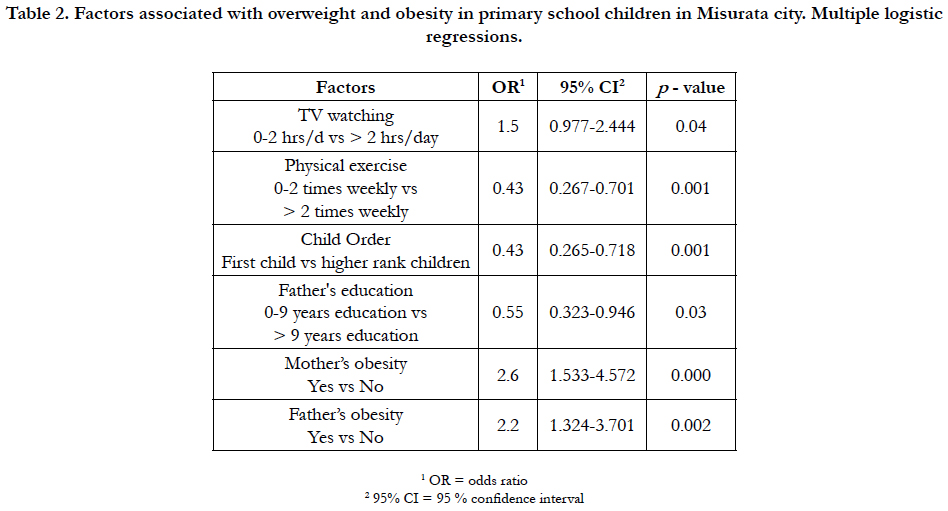
Table 2. Factors associated with overweight and obesity in primary school children in Misurata city. Multiple logistic regressions.
Discussion
Childhood obesity is a serious public health problem with a rapidly increasing prevalence worldwide. The problem is surprisingly difficult to define. It is associated with several risk factors for the development of heart disease and other chronic diseases [8]. Prevalence of obesity and overweight varies greatly with age groups, gender and socioeconomic status. It has been shown that the epidemiological transition seen in the developing countries as a result of, urbanization, migration, adopting new eating habits and recent affluence, are considered as some of the factors involved in the development of obesity and overweight [2].
In the present study, the overall prevalence of overweight and obesity among primary school children from both sexes (males and females) in Misurata city based on the BMI charts percentile for age and gender, of the American National Health and Nutrition Examination Survey (NHANES), were (15.8% and 12.4%), respectively. The prevalence of obesity was almost the same for both sexes (12.5% in boys versus 12.2% in girls, p>0.05). A slightly, higher proportion of girls than boys were overweight (16.1% versus 15.4%), but it was not statistically significant (p>0.05).
When combining both overweight and obesity as a reflection of weight problems, their prevalence in both sexes was almost similar (27.9 % in boys versus 28.3 % in girls). Prevalence of overweight and obesity among boys in this study was 15.4% and 12.5%, respectively and the prevalence of overweight and obesity among girls was 16.1% and 12.2%, respectively.
This prevalence was lower than the prevalence of overweight and obesity among boys in the UK [9] where the prevalence of overweight and obesity among boys under 11 years was (29.6% and 14.9%), respectively and the prevalence of overweight and obesity among girls under 11 years was (25.9% and 12.5%), respectively.
Our study demonstrated that the prevalence of overweight and obesity are significantly increasing with age. The proportion of overweight and obesity increased from 14.7% and 12.1% at age group 6-8 years reaching 16.6% and 12.6%, respectively, at age group 9-11 years. This may give the impression that obesity is a progressive phenomenon that once present, tends to increase with time. This is consistent with a study of primary female school children in Al-Ain city, UAE [2], which found a significant increase in the proportion of overweight and obese children at age 11 years (Figure 1).
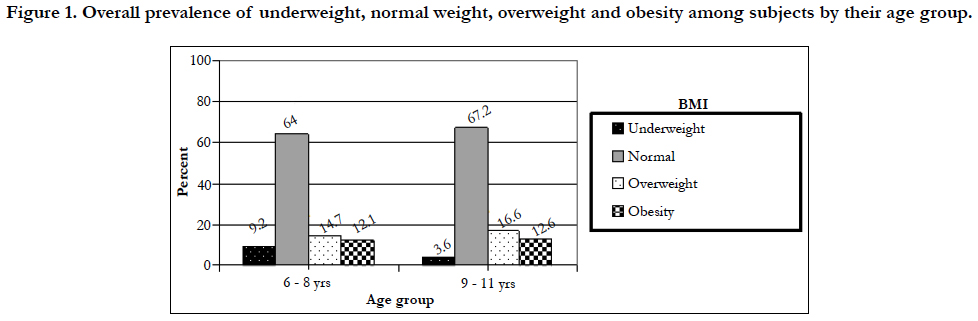

Figure 1. Large sacrococcygeal tumor observed postnatally.
The multiple logistic regression analysis showed that TV watching more than 2 h/day, physical exercise, child order, and parent's obesity were significantly associated with child overweight and obesity after adjusting for age and sex, while father education was significantly associated with child obesity.
Several studies had agreed upon the importance of TV watching in the development of overweight and obesity [2, 10]. Our results showed a positive correlation between times spent watching television and child overweight and obesity. This may be due to the habit of eating while watching TV and less active life style. The odds ratio (OR) of being overweight and of being obese was 1.5 times greater for subjects who used to watch television, for more than 2 hrs per day as compared with those watching TV less than or equal 2 hrs per day.
The study findings are in agreement with Crespo [10], who found that, the prevalence of obesity increased as hours of television watching increased. They reported that, the prevalence of obesity is greater among children who watched 4 or more hours of television a day and lowest among children who reported watching 1 hour or less of television per day. Our results also agree with the findings of Abdelhamid et al., [2], who found a higher risk for overweight among children who watched TV for more than 2 h/d.
Several cross-sectional and population studies had shown a negative relationship between level of physical activity and indices of obesity [10-12]. Our results showed that inactive children were more likely to be overweight and obese compared to active children. Physical activity showed protective effect (OR=0.5). It is noted that in many schools, physical activity was cancelled from the curriculum.
Our research findings showed that child order was a significant factor overall, with first-born child is more likely to be overweight and obese than higher rank children. This result may be due to social and cultural aspects which devote greater attention on the first child. Also the concepts of healthy child, or being first time mothers, tend to be clumsy with the first child in terms of feeding system.
The present study showed that child obesity was significantly associated with parent obesity. It found that the risk of child becoming obese increased almost 2.2 fold if the father was obese and 2.6 fold if the mother was obese. Our findings are in agreement with the findings of Lake et al., [13], who found that parent's obesity is one of the most important risk factors for childhood obesity. They also reported a stronger pattern of overweight tracking from childhood to adulthood among subjects with obese parents.
Our findings are also in agreement with the findings of Abdelhamid et al., [2], reported an association between obesity and family history of obesity (OR=2.6).
Our study showed an inverse relationship between education level of fathers and child obesity (OR=0.5). Prevalence of obesity was associated with low education level of fathers (0-9 year's education). It seems that better educated people are more aware of this problem and more enthusiastic about protecting their children from the dangers of overweight and obesity. This assumption was agreement with the findings of Garn et al., [14]. On the other hand our study findings is in disagreement with the findings of Raja'a et al., [15], who found a positive association of obesity with the educational level of fathers.
Conclusion
Childhood obesity in Misurata is an important public health problem and the prevalence of overweight and obesity is considered high in primary school children.
The sample is a representative of primary school children in Misurata city, and it is not a representative sample of the whole country , so further studies in different regions in Libya are to be performed to identify prevalence of overweight and obesity at the national level, and prevention efforts will be designed accordingly.
Acknowledgement
Special thanks to the officials of both local health and education authorities in the province of Misurata in Libya, including Misurata Central Pharmacy, for their help in conducting the field study.
Grateful Acknowledgement is also due for the school health unit in Misurata, nurses, school principles, and parents of school children who participated and contributed to this study.
References
- World Health Organization Media Centre. Obesity and Overweight Geneva, Switzerland; 2013.
- Kerkadi A, Abo-Elnaga N, Ibrahim W. Prevalence of overweight and associated risk factors among primary female school children in Al-Ain city United Arab Emirates. Emir J Agric Sci. 2005:43-56.
- Badrinath P, Al-Shboul QA, Zoubeidi T, Gargoum AS, Ghubash R, El-Rufaie OE. Measuring the health of the nation: united Arab Emirates Health and Lifestyle Survey 2000. Faculty of Medicine & Health Sciences and College of Economics Al Ain. 2002.
- Cochrane WG. Sampling Techniques. 2nd ed. Johwilly and Sons: USA; 1963. 11p.
- Lohman TG. The use of skinfold to estimate body fatness on children and youth. J Sport Health Sci. 1987 Dec 1;58(9):98-103.
- Flegal KM, Wei R, Ogden C. Weight-for-stature compared with body mass index–for-age growth charts for the United States from the Centers for Disease Control and Prevention. Am J Clin Nutr. 2002 Apr;75(4):761-6. PubMed PMID: 11916765.
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry. Report of a WHO Expert Committee. Geneva, Switzerland; 368-369.
- Obesity-Preventing WH. managing the global epidemic. Report of a WHO Consultation on Obesity. Geneva: 1997 Jun:7-17.
- Jotangia D, Moody A, Stamatakis E, Wardle H. Obesity among children under 11. London: National Statistics. 2005 Apr:1-23.
- Crespo CJ, Smit E, Troiano RP, Bartlett SJ, Macera CA, Andersen RE. Television watching, energy intake, and obesity in US children: results from the third National Health and Nutrition Examination Survey, 1988-1994. Arch Pediatr Adolesc Med. 2001 Mar;155(3):360-5. PubMed PMID: 11231802.
- Garaulet M, Martínez A, Victoria F, Pérez–Llamas F, Ortega RM, Zamora S. Differences in dietary intake and activity level between normal-weight and overweight or obese adolescents. J Pediatr Gastroenterol Nutr. 2000 Mar;30(3):253-8. PubMed PMID: 10749407.
- Moore LL, Nguyen US, Rothman KJ, Cupples LA, Ellison RC. Preschool physical activity level and change in body fatness in young children: the Framingham Children's Study. Am J Epidemiol. 1995 Nov 1;142(9):982-8. PubMed PMID: 7572980.
- Lake JK, Power C, Cole TJ. Child to adult body mass index in the 1958 British birth cohort: associations with parental obesity. Arch Dis Child. 1997 Nov;77(5):376-81. PubMed PMID: 9487953.
- Goran MI. Energy metabolism and obesity. Med Clin North Am. 2000 Mar;84(2):347-62. PubMed PMID: 10793646.
- Raja’a YA, Mohanna MA. Overweight and obesity among schoolchildren in Sana’a City, Yemen. Ann Nutr Metab. 2005 Sep-Oct;49(5):342-5. Epub 2005 Aug 22. PubMed PMID: 16118485.





