Hepatic Hydrothorax – Rare Complication in Pediatrics
Tuan DM1, Nhung BT1, Tran NTN1*, Hoan NTM1, Hoa LT1, Nga NT1, Hoa NPA2, Ninh TP3, Dung LT4
1 Respiratory Department of Vietnam National Hospital of Pediatrics, Vietnam.
2 Hepatobiliary Department of Vietnam National Hospital of Pediatrics, Vietnam.
3 Image Department of Vietnam National Hospital of Pediatrics, Vietnam.
4 Resident Doctor of Vietnam National Hospital of Pediatrics, Vietnam.
*Corresponding Author
Nguyen Thi Ngoc Tran,
Respiratory Department of Vietnam National Hospital of Pediatrics,
Vietnam.
E-mail: dr.ngoctran259@yahoo.com.vn
Article Type : Case Report
Received: August 18, 2015; Accepted: November 24, 2015; Published: November 25, 2015
Citation: Tran NTN et al.,(2015) Hepatic Hydrothorax – Rare Complication in Pediatrics. Int J Pediat Health Care Adv. 2(2), 10-12. doi: dx.doi.org/10.19070/2572-7354-150004
Copyright: Tran NTN© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, whichpermits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Pleural perfusion due to cirrhosis isn’t rare in adult, but in pediatrics, it’s uncommon complication. We present a 9 months old girl with recurrent right pleural effusion. The formation of pleural fluid in this patient was a result of fluid movement from peritoneal to pleural space across diaphragmatic defects. This mechanism was proved.
2.Case Presentation
2.1.Pre-medical history
2.2.Examine
2.3.Investigations
2.4.Initial treatment
3.Discussion
3.1.Treatment
5.Conclusion
6.References
Keywords
Hepatic Hydrothorax; Crirrhosis.
Case Presentation
9 months old girl was detected right pleural effusion in a periodic examination.
Normal delivery, persistent jaundice after birth. When she was 4 months old, she was diagnosed hydrocephalus, and operated to place ventriculoperitoneal shunt. At 6 months of age, she was diagnosed CMV hepatitis/cholestatic jaundice and treated with Gancyclovir.
She had diminished breath sounds in lower lobar of right lung,no crackle rales, no dyspnea, no cough. A cardiovascular examination was normal. An infectious status was unremarkable. Edema wasn’t noted. Liver was 2 cm and spleen was 1 cm under costal margin. She had cholestatic jaundice with yellow stool, no petechiae, no red spider-like blood vessels on the skin.


Table
Right pleural effusion (Figure 1).
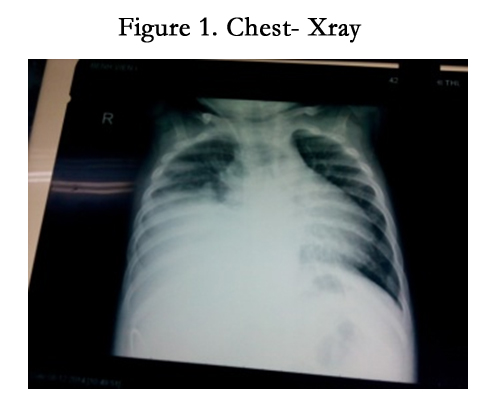

Figure 1. Chest- Xray
Ventriculoperitoneal shunt valve was too close to the right diaphragm (Figure 2).
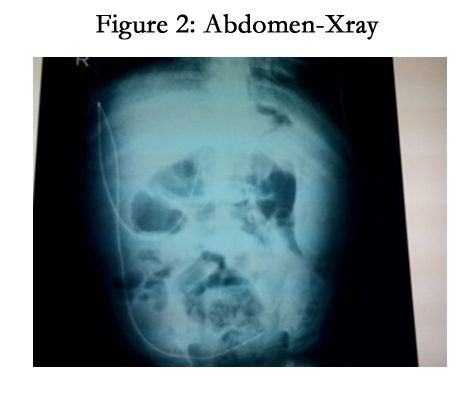

Figure 2: Abdomen-Xray
Mild tricuspid regurgitation, mild pulmonary hypertension. Cranial CT scan: Mild ventricular dilation.
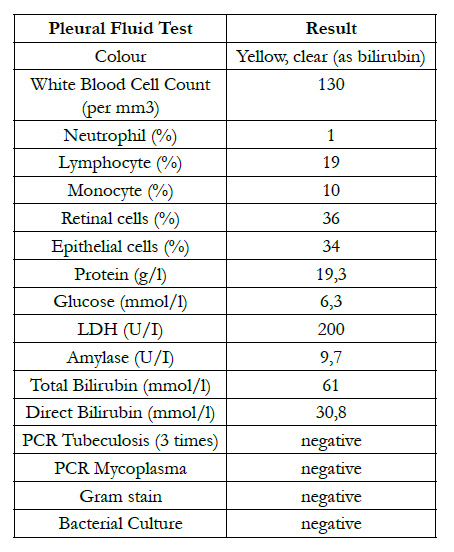
Table
Serum protein: 67 g/l, Albumin: 35g/l. Amylase serum: 35 U/L. GOT: 428 U/L, GPT 256 U/L, total bilirubin: 209, direct: 104 mcmol/l. PT: 68%, Ure: 5,3 mmol/l , Creatinin: 80 mcmol/l, blood PCR CMV(-), CMV IgG(+), CMV IgM (-).
The patient was treated with antibiotic, pleural effusion drainage (3 times because of recurrence) (Figure 3).
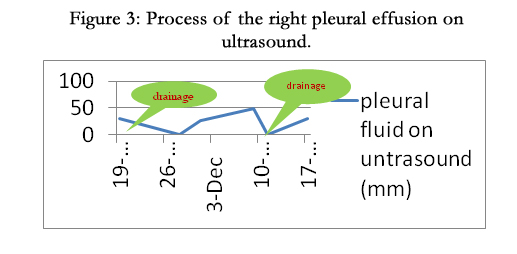
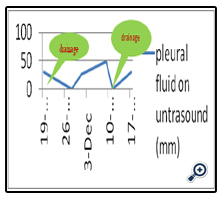
Figure 3: Process of the right pleural effusion on ultrasound.
Then she was operated to replace AP shunt (because we suspected that ectopic position of AP valve might cause pleural effusion) and found nodes on the liver surface.
Grade IV cirrhosis (Figure 4).
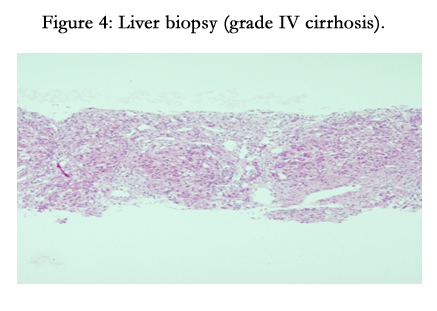
Figure 4: Liver biopsy (grade IV cirrhosis).
Injected 99mTc into patient’s abdomen (Figure 5); 2 hours later, 99mTc was found in right pleural (Figrue 6).
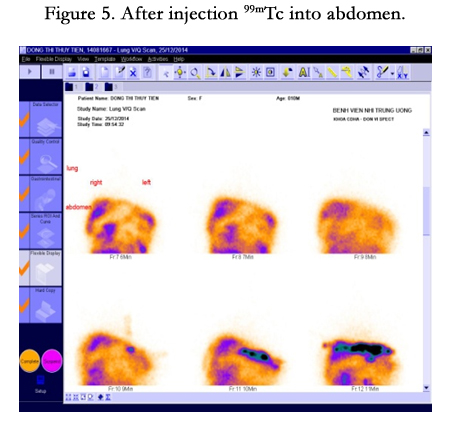
Figure 5. After injection 99mTc into abdomen.
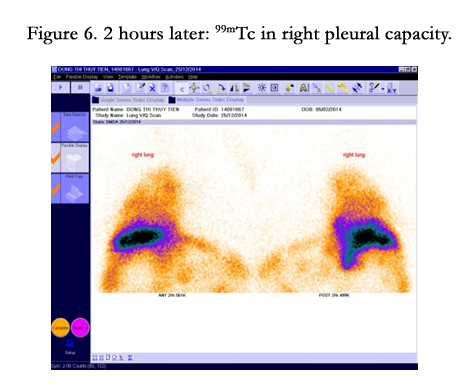
Figure 6. 2 hours later: 99mTc in right pleural capacity.
Hepatic Hydrothorax Treatment with diuretic (furosemide and spironolactone, sandostatin, salt restrict diet) and she got better.
Discussion
Hepatic hydrothorax is defined as a pleural effusion, in patients with cirrhosis without any other underlying primary cardiopulmonary and pulmonary causes [1]. This complication occurs about 4-10% of patients with cirrhosis [2]. In most cases (85%) hepatic hydrothorax develops on the right side, with 13% of cases occurring on the left side and 2% bilateral [2]. Mechanism is the passage of a large amount of ascites from the peritoneal to the pleural cavity through diaphragmatic defects. Typically, the defects are smaller than 1 cm and tend to occur on the right side, and sometimes, just observed by microscopy [3]. Many studies using 99mTchuman Albumin or 99mTc-sulfur colloid and dye studies that show an unidirectional passage of these markers from the abdominal to the pleural cavity in the first 24 hours after administration [4, 5].
Salt restrict diet, diuretics (furosemide and spironolactone). If not response to treatment, alternative treatment was octreotide, TIPS procedure, liver transplant [6].
Conclusion
In pediatrics, hepatic hydrothorax is a rare condition. In addition, in this patient, sign and symptoms of cirrhosis weren’t clear. Diagnosis cirrhosis based on liver biopsy more than clinical finding. Therefore, she wasn’t diagnosed and treated probably at the initial time. However, there were still some problem in this patient we haven’t good understood, such as the cause of cirrhosis and relationship between hydrocephalus and hepatitis/cirrhosis.
References
- Morrow CS, Kantor M, Armen RN (1958) Hepatic hydrothorax. Ann Internal Med 49(1): 193-203.
- Lazaridis KN, Frank JW, Krowka MJ, Kamath PS (1999) Hepatic hydrothorax: pathogenesis, diagnosis, and management. Am J Med 107(3): 262-267.
- Emerson P, Davies JH (1955) Hydrothorax complicating ascites. Lancet. 268(6862): 487-488.
- Rubinstein D, McInnes IE, Dudley FJ (1985) Hepatic hydrothorax in the absence of clinical ascites: diagnosis and management. Gastroenterology 88(1 Pt 1): 188-191.
- Benet A, Vidal F, Toda R, Siurana R, De Virgala CM, et al. (1992) Diagnosis of hepatic hydrothorax in the absence of ascites by intraperitoneal injection of 99m-Tc-Fluor colloid. Postgrad Med J 68(796): 153.
- Kiafar C, Gilani N (2008) Hepatic hydrothorax: Current concepts of pathophysiology and treatment options. Ann Hepatol 7(4): 313-320.





