Clinical Study of Primary Ocular Tuberculosis
Tanushree V1*, Venkate Gowda HT2
1 Senior Resident, Department of Ophthalmology, Mysore Medical College and Research Institute, Mysore.
2 Professor and HOD, Department of Ophthalmology, Mysore Medical College and Research Institute, Mysore.
*Corresponding Author
Dr.Tanushree V,
Senior Resident, Department of Ophthalmology, Mysore Medical College and Research Institute,
#1128, 1st cross, Paduvana road, T.K.layout, Kuvempunagar, Mysuru: 570023,
Karnataka, India.
Tel: +919481438530
E-mail: tanushree19686@gmail.com
Received: June 11, 2016; Accepted: July 07, 2016; Published: July 08, 2016
Citation: Tanushree V, Venkate Gowda HT (2016) Clinical Study of Primary Ocular Tuberculosis. Int J Opthalmol Eye Res, S8:001, 1-4. doi: dx.doi.org/10.19070/2332-290X-SI08001
Copyright: Tanushree V© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: “Primary Ocular Tuberculosis” describes an infection by the M. tuberculosis species that can affect any part of the eye (intraocular/extraocular) without any systemic manifestations.
Materials and Methods: Prospective Study was conducted in a tertiary care hospital on patients diagnosed to have primary
ocular tuberculosis attending the outpatient and inpatient department of ophthalmology.
Results: In our study we reported 7 cases of primary ocular tuberculosis. Tuberculosis of eyelid (1 case), Tuberculosis of
conjunctiva (2 cases), Tuberculosis of lacrimal sac (2 cases), Tuberculsois of uvea presenting as acute non granulomatous
anterior uveitis with iris granuloma (1 case) and infectious tubercular scleromalacia perforans (1 case).
Conclusion: Since ocular tuberculosis is treatable and eyes can be saved using anti-tuberculous treatment if detected early, considerable stress should be laid on its early diagnosis and prompt treatment so as to prevent ocular morbidity and blindness.
2.Introduction
3.Materials and Methods
3.1.Source of Data Collection
3.2.Method of data collection
3.3.Method of Study
3.3.Statistical Methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Primary Ocular Tuberculosis; Secondary Ocular Tuberculosis; Tuberculosis of Lacrimal SAC; Tuberculosis of Iris.
Introduction
Tuberculosis (TB) is an infection caused by Mycobacterium tuberculosis, which can cause disease in multiple organs throughout the body, including the eye. The term “Primary Ocular Tuberculosis” describes an infection by the M. tuberculosis species that can affect any part of the eye (intraocular/extraocular) without any systemic manifestations. “Secondary ocular TB” is defined as ocular involvement as a result of seeding by hematogenous spread from a distant site or direct invasion by contiguous spread from adjacent structures, like the sinus or cranial cavity.
TB is an airborne communicable disease that most commonly involves the lungs. Nearly one third of the world’s population is latently infected with TB, and more than 9 million new cases are diagnosed each year, 95% in developing countries.
Ocular TB may not be associated with clinical evidence of pulmonary TB; up to 60% of patients with evidence of extrapulmonary TB may not have diagnosed pulmonary TB Ocular TB may be an initial presentation of extrapulmonary dissemination of infection. Posterior uveitis is the most common presentation of intraocular TB.
The gold standard for diagnosing intraocular TB is demonstration of Mycobacterium tuberculosis from the intraocular fluid or tissues by microbiological or histopathological examination. The currently available laboratory methods provide an indirect evidence of tubercular etiology of uveitis. The diagnosis of intraocular TB still remains largely presumptive as the ocular tissue is rarely sampled. The use of specific clinical signs as markers predicting TB as the cause of uveitis in a TB endemic area has been recently reported. Definitive diagnosis of extraocular TB in a patient with uveitis also aids in diagnosing intraocular TB.
Intraocular TB has a wide clinical spectrum that may include uveitis, retinal vasculitis, serpiginous like choroiditis, choroidal tubercles or granuloma, subretinal abscess, or panuveitis. The rare manifestations include endophthalmitis, panophthalmitis and neuroretinitis. Extraocular manifestations commonly in the lid and adnexa has also been described.
Immunocompromised individuals may have atypical presentations like hypopyon uveitis, or endophthalmitis.
The aim of this study is to note the clinical manifestations in patients with primary ocular tuberculosis without any other systemic manifestations involved.
Materials and Methods
Study was conducted in a tertiary care hospital on patients diagnosed to have primary ocular tuberculosis attending the outpatient and inpatient department of ophthalmology.
The number of cases which will meet the inclusion criteria during study period.
Prospective.
2012- 2015
All patients with primary Ocular Tuberculosis.
All patients with pulmonary and extrapulmonary tuberculosis other than ocular tuberculosis.
Assessment of clinical presentation of all patients with diagnosed ocular Tuberculosis by clinical and histopathological study without any pulmonary/extrapulmonary other than ocular tuberculosis. All patients with confirmed ocular tuberculosis received standard antitubercular treatment along with routine ocular treatment.
The study was analysed by Descriptive statistics and Independent t tests.
Results
In our study we reported 7 cases of primary ocular tuberculosis. Tuberculosis of eyelid (1 case), Tuberculosis of conjunctiva (2 cases), Tuberculosis of lacrimal sac (2 cases), Tuberculsois of uvea presenting as acute non granulomatous anterior uveitis with iris granuloma (1 case) and infectious tubercular scleromalacia perforans(1 case).
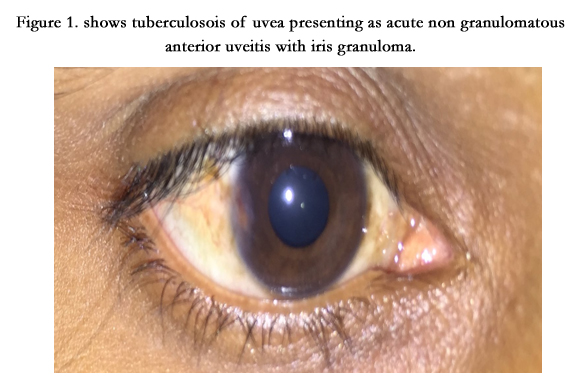

Figure 1. shows tuberculosois of uvea presenting as acute non granulomatous anterior uveitis with iris granuloma.
In this case a 26 year old patients presented with pain and redness in right eye since 15 days. On ocular examination acute non granulomatous anterior uveitis with vacularized iris granuloma was present in the temporal part of Iris. Biopsy was taken from the iris granulomatous lesion and sent for histopathological examination.
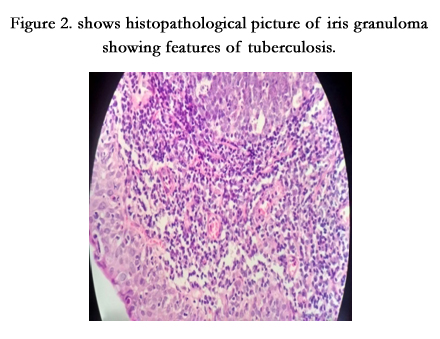
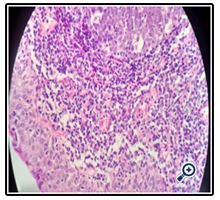
Figure 2. shows histopathological picture of iris granuloma showing features of tuberculosis.
HPE report showed sections of Iris tissue containing loose connective tissue with underlying loose fibrous tissue, lymphocytes, multinucleated giant cells, histiocytes and epitheloid cells forming granuloma. Special stains for Acid fast bacilli was positive. Features were consistent with tubercular granuloma. The patient was advised antitubercular treatment for 9 months with topical steroid eye drops.


Figure 3. shows tuberculosis of conjunctiva who has developed symblepharon with recurrent dacryocystitis with osteomyelitis of lacrimal bone. The patient underwent dacryocystectomy with antitubercular treatment for 9 months.
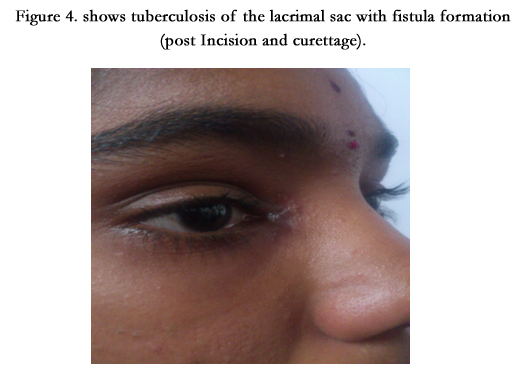

Figure 4. shows tuberculosis of the lacrimal sac with fistula formation (post Incision and curettage).
In this case 18 year old female patient presented with chief complaints of swelling and pain in the right lacrimal sac region since two months. History of watering in right eye since 1 year. She was posted for incision and drainage. On opening abcess there was no evidence of pus but granulation tissue found which was curated and sent for HPE, which revealed tuberculosis of the lacrimal sac. Patient was stared on ATT. In this reported case there is no infection of the neighbouring tissue or could tuberculous lesion be uncovered elsewhere in the body after thorough diagnostic in vestigation.
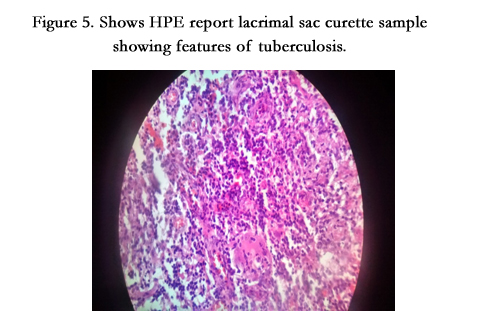
Figure 5. Shows HPE report lacrimal sac curette sample showing features of tuberculosis.
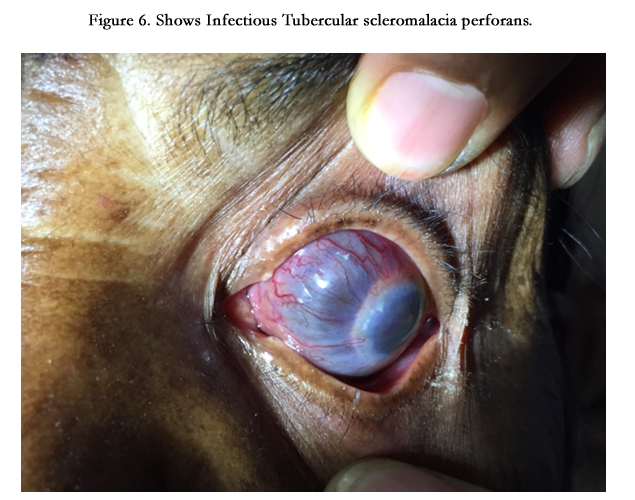

Figure 6. Shows Infectious Tubercular scleromalacia perforans.
In this case 77 yr old female patient presented with forward protrusion, bluish discolouration and loss of vision in the left eye since 2 years.
- Ocular examination (LE)showed:
- Eccentric proptosis.
- Diffuse extensive scleral thinning more marked nasally than temporally with exposure of the underlying uvea with vascular engorgement over the thinned out scleral surface.
- Cornea was hazy with necrotic scleral plaques near the limbus without vascular congestion, anterior chamber was flat and other details were not made out.
- Restriction of extraocular movements was present.
- Vision: No perception of light
- The patient underwent enucleation followed by artificial eye implantation after 3 months for cosmetic purpose. Enucleatedeye ball was sent for Histopathological examination.
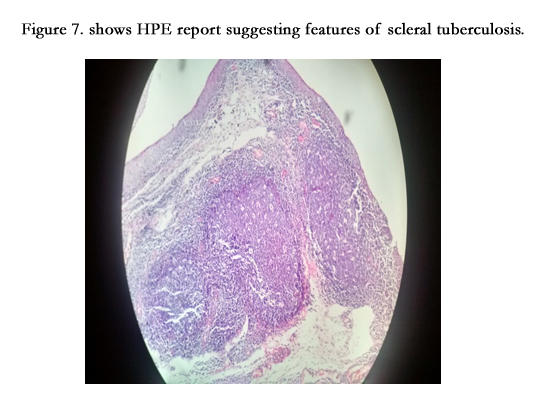
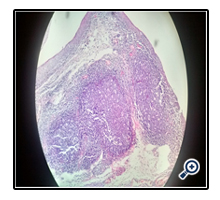
Figure 7. shows HPE report suggesting features of scleral tuberculosis.
HPE report showed sections of episclera and sclera containing loose connective tissue with underlying loose fibrous tissue, lymphocytes, multinucleated giant cells, histiocytes and epitheloid cells forming granuloma. Special stains for Acid fast bacilli is positive. Features consisent with scleral tuberculosis.
Discussion
Tuberculosis is a ubiquitous disease and a major public health problem in developing countries like India. The frequencies of ocular TB in patients with uveitis and systemic TB are respectively 0-0.16% and 0.27-1.4% [1, 2]. The incidence of ophthalmic manifestations in patients known to have systemic tuberculosis is only 1-2% [3]. Tuberculosis remains the world’s leading infectious cause of death and can also cause a variety of diseases throughout the body and the eye. Worldwide there are approximately 8 million new cases and 3 million deaths from tuberculosis each year. Approximately one third of the world’s population has been infected. The demographics of infection vary widely, with developing countries bearing the heaviest burden of disease.
In the United States in 1953, the annual risk of being infected with tuberculosis was 53 per 100000 members of the population [4]. This decreased to 9.4 per 100000 by 1984, and the World Health Organization set a goal of eliminating tuberculosis worldwide. There was a resurgence in the United States to a peak of 10.5 per 100 000 by 1992 ; the reported incidence then declined to 5.1 per 100 000 in 2003 [5]. Ocular tuberculosis has always been considered rare, yet its incidence has varied widely across time, patient populations, and geography. In 1967, Donahue reported an incidence of ocular tuberculosis of 1.46% in 10524 patients from a tuberculosis sanitarium [6].
A prospective study from Spain, reported in 1997, examined 100 randomly chosen patients with proven systemic tuberculosis and found ocular involvement in 18 patients (18%) [7]. In Malawi, Africa, a 2.8% incidence of choroidal granuloma in 109 patients with fever and tuberculosis was reported in a prospective study in 2002 [8]. In India, in a study conducted from January 1992 to December 1994, 0.6% of uveitis cases were believed to be caused by tuberculosis.
In Japan, a prospective case series from April 1998 to August 2000 reported that 20.6% of 126 patients with uveitis had a positive purified protein derivative (PPD) skin test result, and 7.9% were thought to have intraocular tuberculosis. In Saudi Arabia, during the period from 1995 to 2000, tuberculosis was the cause in 10.5% of uveitis cases seen in a referral center [9]. In Boston, 0.6% of patients with uveitis from 1982 to 1992 were believed to have tuberculosis as an underlying cause [10].
Human immunodeficiency virus (HIV) has contributed to the increase in the incidence of tuberculosis worldwide; HIV increases the risk of development of active tuberculosis in patients infected with Mycobacterium tuberculosis. However, rates of ocular tuberculosis in patients with tuberculosis with or without HIV are variable. In a study reported in 1993 of autopsy eyes from 235 patients with AIDS, intraocular tuberculosis was found in only 2 eyes. The effect of HIV on the immune system can influence both the diagnosis, by reducing the response to PPD testing, and the success of treatment.
EE Egbagbe AE, AE Omoti (2008) reported tuberculosis is a cause of ocular morbidity, visual impairment and blindness. Prevention, early diagnosis and early treatment of TB may prevent avoidable visual loss [11].
Aliyu Hamsa Balarabe and Jotirmay Biswas (2015) reported the importance of a detailed ocular, systemic and laboratory evaluation to exclude TB in patients presenting with serpigenous choroiditis particularly if there is delay in clinical response despite appropriate treatment [12].
P Lalitha, SR Rathinam, M Srinivasan (2004) reported that early clinical recognition and prompt laboratory diagnosis together with aggressive topical antibiotic therapy may shorten morbidity and improve the clinical outcome of non tuberculous mycobacterial ocular infection [13].
Conclusion
Ocular tuberculosis may occur in the absence of any systemic disease and the patients may present with a wide variety of clinical signs. Also, the disease can mimic several clinical entities. Tuberculosis may affect all ocular tissues; choroiditis being the most common ocular manifestation. The retinal involvement occurs secondary to the underlying choroidal infection.The extraocular manifestations of the lid and adnexa has been rarely described in the recent review of literature. Treatment for ocular tuberculosis is the same as that for pulmonary tuberculosis. Due to the emergence of drug resistance, multidrug therapy is advocated. In the present time of the HIV pandemic, there has been a resurgence of tuberculosis and it is the most common opportunistic infection in HIV positive patients. HIV related TB shows a higher prevalence of extrapulmonary and disseminated TB. In our cases no HIV positive cases has been reported. Since the disease is treatable and eyes can be saved using anti-tuberculous treatment if detected early, considerable stress should be laid on its early diagnosis and prompt treatment so as to prevent ocular morbidity and blindness.
References
- Copeland RA Jr (1993) The classics: Tuberculosis, Syphilis and sarcoidosis. Ophthalmol Clin North Am 6: 69-80.
- Helm CJ Holland GN (1993) Ocular tuberculosis. Surv Ophthalmol 38(3): 229-256.
- Demirci H, Shields CL, Shields JA,Eagle RC (2004) Ocular tuberculosis masquerading as ocular tumours. Surv ophthalmol 49(1): 78-89.
- Espinal MA, Laszlo A, Simonsen L (2001) Global trends in resistance to antituberculosis drugs: World Health Organization-International Union Against Tuberculosis and Lung Disease Working Group on Anti-Tuberculosis Drug Resistance Surveillance. N Engl J Med 344(17): 1294- 1303.
- Donahue HC (1967) Ophthalmologic experience in a tuberculosis sanatorium. Am J Ophthalmol 64(4): 742- 748.
- Beare NA, Kublin JG, Lewis DK (2002) Ocular disease in patients with tuberculosis and HIV presenting with fever in Africa. Br J Ophthalmol 86(10):1076- 1079.
- Biswas J, Narain S, Das D, Ganesh SK (1996) Pattern of uveitis in a referral uveitis clinic in India. Int Ophthalmol 20(4): 223- 228.
- Morimura Y, Okada A, AKawahara S (2002) Tuberculin skin testing in uveitis patients and treatment of presumed intraocular tuberculosis in Japan.Ophthalmology 109(5): 851- 857.
- Islam SM, Tabbara KF (2002) Causes of uveitis at The Eye Center in Saudi Arabia: a retrospective review. Ophthalmic Epidemiol 9(4): 239- 249.
- Rodriguez A, Calonge M, Pedroza-Seres M (1996) Referral patterns of uveitis in a tertiary eye care center. Arch Ophthalmol 114(5): 593- 599.
- Egbagbe EE, Omoti AE (2008) Ocular disorders in adult patients with tuberculosis in a tertiary care hospital in Nigeria. Middle East Afr J Ophthalmol 15(2): 73-76.
- Balarabe AH, Biswas J (2015) Presumed tuberculous choroiditis:Unusual presentation and review of the literature. Saudi J Health Sci 4(2): 79-81.
- Lalitha P, Rathinam SR, Srinivasan M (2004) Ocular infections due to non tuberculous mycobacteria. Indian J Med Microbiol 22(4): 231-237.





