A Rare Location of Eyelid Kaposi Disease
Lahlou A*, Baybay H, Mernissi FZ
Departement of Department, University Hospital Hassan II, Morocco.
*Corresponding Author
Asmae Lahlou,
Department of Department, University Hospital Hassan II, Fez, Morocco.
E-mail: lahlouasmae@gmail.com
Received: September 04, 2016; Accepted: October 14, 2016; Published: October 17, 2016
Citation: Lahlou A, Baybay H, Mernissi FZ (2016) A Rare Location of Eyelid Kaposi Disease. Int J Ophthalmol Eye Res. 4(9), 253-255.
doi:dx.doi.org/10.19070/2332-290X-1600053
Copyright: Lahlou A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The classic Kaposi's disease is an uncommon endothelial malignant tumor, first described by Moricz Kaposi in 1872. It is commonly encountered in patients with acquired immunodeficiency syndrome (AIDS), immunosuppression or organ transplantation. Eylid location is rare , mostly in patients with AIDS. We present a selected case with a purplish erythematous lesion in the upper eyelid in a patient who is HIV negative and immunocompetent, with an unremarkable general medical history. The lesion was surgically excised with no adjunctive treatment, and histological examination confirmed the diagnosis.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
Kaposi’s Sarcoma; Eylid; Immunosuppression.
Introduction
The classic Kaposi's disease (CKD) is a proliferative disease and multifocal double vascular component and fibroblast cell, cutaneous and visceral expression, first described by Moricz Kaposi in 1872. It is frequently encountered in patients with acquired immunodeficiency syndrome (AIDS), immunosuppression, organ transplantation or human herpes simplex virus-8 (HHV-8) infection [1-2]. palpebral localization is rare and is encountered mostly in patients with AIDS, in some cases as the first clinical presentation [3, 4]. We report a case of an immunocompetent patient with a superior eylid CKD, managed with surgical excision.
Case Report
A 70-year-old male presented with a 4 month history of a gradually growing mass on his left upper eyelid, with swelling, irritation and pain on this eyelid. Clinical examination showed a purplish erythematous patch , although limited firm, 1 cm in diameter sitting as the level of the upper eyelid, annoying vision (Figure 1), This was an ocular involvement in a HIV-negative patient, with no clinical evidence of immunosuppression and unremarkable general health. the rest of the skin examination revealed multiple erythematous papules and purplish plaques finely squamous place by the levels of before the arms and legs, the dermoscopic examination of the lesions showed a dark purple color with scales and appearance rainbow (Figure 2). The rest of the physical examination was unremarkable, especially the lymph nodes that were free. The patient underwent surgical resection with good aesthetic and functional result. Histological examination confirmed the diagnosis showing Double fusiform and vascular cell proliferation with extravasation of erythrocytes and hemosiderin deposition(Figure 3). Cell proliferation is of endothelial origin associated with inflammatory cells, presence of spindle cells positive on CD31, CD34.
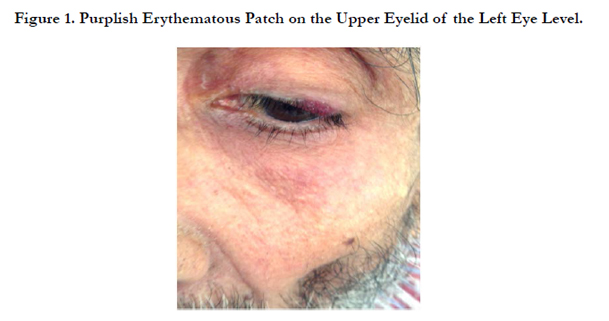
Figure 1. Purplish Erythematous Patch on the Upper Eyelid of the Left Eye Level.
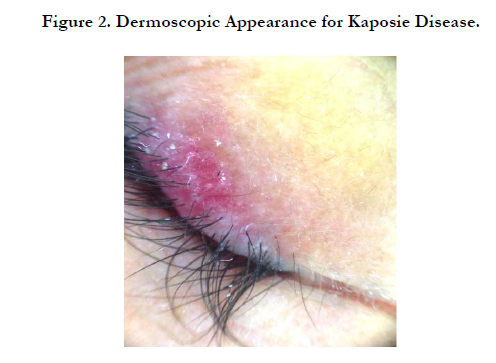
Figure 2. Dermoscopic Appearance for Kaposie Disease.
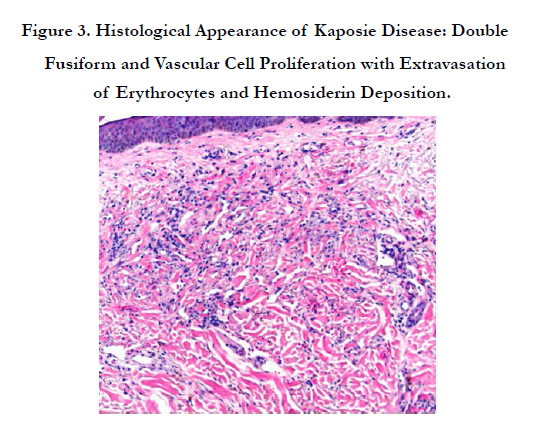
Figure 3. Histological Appearance of Kaposie Disease: Double Fusiform and Vascula
Discussion
CKD is a vascular proliferative lesion first recorded in 1872, when the Hungarian dermatologist syphilologist Moric Kaposi described 5 cases of an unusual tumor that principally affected the skin of the lower extremities of elderly patients [5]. In HIV-negative patients, this rare endothelial and vascular smooth muscle cell neoplasm follows an indolent, slowly expanding course and is typically characterized by purplish to red cutaneous macules on the hands and feet. It usually progresses up the limbs to form nodules and culminates with visceral or mucosal involvement in some patients.
Ocular CKD is rare in HIV-negative patients with less than 30 cases being reported before 1982. Only 20% of AIDS patients suffering from CKD have ocular manifestations (lids or conjunctiva) and in 12% of cases ocular involvement is the primary manifestation of systemic disease [6-7]. Ron et al., [3] and Munteanu et al., [8] have reported 2 cases similar to ours: both patients were HIV-seronegative and had a palpebral-conjunctival involvement of CKD, together with systemic skin lesions. Similar cases have been reported in HIV-positive patients, who display additional lesions elsewhere [9]. The case reported by Shields et al., [10] is also of interest: these authors described an HIV-positive man with a 4-month history of progressively enlarging bilateral eyelid tumors. Because these lesions did not respond to systemic medications, he was successfully treated with radiotherapy. Simple complete surgical excision was curative in our case. Differential diagnosis of similar lesions should include arteriovenous shunt, pyogenic granuloma, malignant blue nevus, bacterial angiomatosis and vascular malformations [3]. The clinic and dermoscopy can eliminate other differential diagnoses. The etiology of CKD has been linked to an HHV-8, also called the CKD-associated herpesvirus, which was identified in 1994 by Chang et al and belongs to the family of F-herpesviruses, a subgroup whose best-known type is the Epstein-Barr virus [11]. Isolated CKD of the conjunctiva unrelated to AIDS have been reported previously, Complications eyelid locations are represented by entropion, ectropion, trichiasis, providers lagophthalmos, eye irritation, corneal ulcer and abscess or haemorrhages. When the disease begins to progress, both local and systemic therapies can be used. These include conventional surgery, cryotherapy, laser therapy, intralesional injections of vinblastine or bleomycin, interferon, radiotherapy with a multiple- fraction regimen, and systemic chemotherapy with liposomal daunorubicin or paclitaxel [12]. In our case the management was surgical because eyelid lesions are always trouble some functionally.
Conclusion
Eyelid locations of classical Kaposi's disease are rare. The lesions often have a nodulo-tumor character and are associated, in aggressive forms, secondary ocular complications, Surgical treatment is usually made because of the functional gene.
References
- Verma V, Shen D, Sieving PC, Chan CC (2008) The role of infectious agents in the etiology of ocular adnexal neoplasia. Surv Ophthalmol. 53(4): 312–331.
- Lieberman PH, Llovera IN (1972) Kaposi’s sarcoma of the bulbar conjunctiva. Arch Ophthalmol. 88(1): 44–45.
- Ron IG, Kremer I, Lowenstein A, Chaitchik S (1994) Conjunctival involvement in classic (indolent) HIV negative Kaposi’s sarcoma. Br J Ophthalmol. 78(6): 488-489.
- Kurumety UR, Lustbader JM (1995) Kaposi’s sarcoma of the bulbar conjunctiva as an initial clinical manifestation of acquired immunodeficiency syndrome. Arch Ophthalmol. 113(8): 978.
- Kaposi M (1872) Idiopatisches multiples Pigmentsarkom der Haut. Arch Dermatol Syph. 4: 265-273.
- Schmid K, Wild T, Bolz M, Horvat R, Jurecka W, et al., (2003) Kaposi’s sarcoma of the conjunctiva leads to a diagnosis of acquired immunodeficiency syndrome. Acta Ophthalmol Scand. 81(4): 411–413.
- Kalinske M, Leone CR Jr (1982) Kaposi’s sarcoma involving eyelid and conjunctiva. Ann Ophthalmol. 14(5): 497– 499.
- Munteanu G, Munteanu M, Giuri S (2003) Conjunctival-palpebral Kaposi’s angiosarcoma: report of a case. J Fr Ophtalmol. 26(10): 1059-1062.
- Corti M, Solari R, de Carolis L, Corrar R (2001) Eye involvement in AIDSrelated Kaposi sarcoma. Enferm Infecc Microbiol Clin. 19(1): 3-6.
- Shields JA, De Potter P, Shields CL, Komarnicky LT (1992) Kaposi’s sarcoma of the eyelids: response to radiotherapy. Arch Ophthalmol. 110: 1689.
- Chang Y, Cesarman E, Pessin MS, Lee F, Culpepper J et al., (1994) Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi_s sarcoma. Science. 266: 1865-1869.
- Shepherd FA, Maher E, Cardella C, Cole E, Greig P et al., (1997) Treatment of Kaposi’s sarcoma after solid organ transplantation. J Clin Oncol. 15(6): 2371-2377.





