Relation of Pupil Size and retinal diseases
Rickmann A1*, Waizel M1, Kazerounian S1, Szurman P1,2, Boden KT1
1 Knappschaft Eye Clinic Sulzbach, Knappschaft Hospital Saar, Sulzbach, Saar, Germany.
2 University Eye Clinic Tuebingen, Centre for Ophthalmology, Tuebingen, Germany.
*Corresponding Author
Dr. Annekatrin Rickmann,
Knappschaft Eye Clinic Sulzbach, Knappschaft Hospital Saar, An der Klinik 10,
66280 Sulzbach/Saar, Germany.
Tel: 06897574-1119
Fax: 06897574-2139
E-mail: annekatrinrick@gmail.com
Received: June 26, 2016; Accepted: August 05, 2016; Published: August 09, 2016
Citation: Rickmann A, Waizel M, Kazerounian S, Szurman P, Boden KT (2016) Relation of Pupil Size and Retinal Diseases. Int J Ophthalmol Eye Res. 4(7), 242-245.DOI : dx.doi.org/10.19070/2332-290X-1500050
Copyright: Rickmann A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: The aim of this study was to evaluate differences in pupil size of subjects with diabetes mellitus, age-related macular degeneration and retinal vein occlusion at different illumination levels with a novel pupilometer.
Methods: The pupil size of study participants was measured with an infrared-video pupillometer (PupilX, Albomed) at 5 different illumination levels (0, 0.5, 4, 32 and 250 lux). Measurements were performed by the same investigator. 90 images were executed during a measurement period of 3 seconds.
Results: This cross-sectional study analysed 484 eyes of 242 patients with diabetes mellitus (DM), age-related macular degeneration (AMD) and retinal vein occlusion (RVO); mean age 73.8 ± 12 years, range 45-92 years. A healthy control group had 342 eyes, mean age 61.4 ± 12.5 years, range 40-87 years. There was a statistically significant smaller pupil size at the DM-group in comparison to AMD, RVO and control group at all illumination levels, except 250 lux (p=0.041, Kruskal Wallis test). There was no statistically significant difference in pupil size of RVO and AMD in comparison to the control group. Conclusion: This study provides comparative data for pupil size at different retinal diseases at different illumination conditions measured with PupilX. Pupil size in diabetic patients was significantly smaller at scotopic and mesopic illuminance conditions. Therefore we confirm using pupillometry as a noninvasive and simple tool for additive detection of autonomic dysfunction in diabetes mellitus.
2.Introduction
3.Methods
3.1.Patients
3.2.Technical procedure
3.3.Data analysis
4.Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.References
Keywords
Diabetic Neuropathy; Pupilometer; PupilX; Retinal Vein Occlusion.
Introduction
Pupillometry is a simple and sensitive tool for detection of autonomic dysfunction [1]. The relationship between dynamic pupillary function and peripheral nerve function was already described by Levy et al., [2]. The Parasympathetic and sympathetic pupillary dysfunction appears to be a common feature of autonomic impairment in diabetes mellitus [3] and is evidenced by diminished amplitude reflexes and significant smaller pupil diameter [1]. Furthermore, Ko et al., showed that the pupillary diameter is related to poor metabolic control, long diabetes duration, and also to other indices of microvascular diseases in patients with diabetes [4].
The autonomic neuropathy is a common and serious complication of diabetes mellitus. Therefore an early detection is essential to enable appropriate interventional therapy and management [5]. The pupillometer is proven reliable and effective for diagnosing diabetes in an early stage [4].
Previously, pupillometric analyses were performed with variable devices and under variable test conditions. The PupilX (Albomed) device defines a new standard for digital pupillometry. PupilX enables to measure bilateral pupil sizes simultaneously under constant and adjustable illumination levels, fascilitating comparable measurements under scotopic, mesopic and photopic conditions [6]. Schilde et al., reported on most precise measurements with PupilX [6].
The aim of this study was to evaluate the pupil size for diabetes mellitus patients in comparison to a healthy control group and other retinal diseases like age-related macular degeneration and retinal vein occlusion at different daily light conditions and to ascertain whether the new pupilometer is a simple tool for detection of diminished pupillary responses in different conditions and diseases.
Methods
The pupil size of healthy participants (control group) and patients was measured using the PupilX pupillometer (Albomed). Inclusion criteria were diagnosis of diabetic macular oedema, exsudative age-related macular degeneration or macular oedema caused by retinal venous occlusion. Exclusion criteria were rubeosisiridis, trauma or interfering topical or systemic medication. Exclusion criteria for the healthy control group were additional any history of eye disease or loss of vision. An additional slitlamp examination excluded other morphological abnormalities of the anterior eye segment. All participants were pseudophakic.
Patient’s eyes were measured at 5 illumination levels with 0, 0.5, 4, 32 and 250 lux. The protocol order proceeded from the dimmest to the brightest condition. No subject was exposed to bright light directly before measurement. Furthermore, all patients underwent a 2 minute retinal adaptation phase in the same room under low mesopic conditions (darkened room where the only light was from the device). This was monitored by the same investigator. By using light-tight rubber eyecups, the PupilX pupillometer allows for measurements under scotopic conditions without the need to completely darken the examination room. The participants saw a white uniform LED field with adjustable brightness, which could be switched off for scotopic conditions. The subjects were requested to look straight ahead and keep their eyes open for the whole measurement period. Patient’s eyes were measured at 5 illumination levels, starting at 0 Lux. We performed the measurements at 0.5, 4, 32 and 250 lux, allowing 5-10 seconds for participants to adapt to the illuminance level in advance. All measurements were performed and observed via display by the same investigator.
At each continous level of illumination, 90 images were acquired,30 images per second over a measurement period of 3 seconds. The absolute linear camera resolution was approximately 20 pixels per mm. The resolution of measurements of the entire system is +/- 0.1 mm for pupils < 3.3 mm and +/- 3% for pupils > 3.3 mm. Pupil tracking circles were automatically fitted to image data indicating the pupil borders. This could be observed on the monitor. Recordings with blink artefacts were automatically discarded and repeated. Both eyes were recorded simultaneously. The software analyzed average pupil size with standard deviation (i.e. short term variability within the measurement period) and anisocoria over the measurement period of 3 seconds. Data could also be selected for all 90 single measurements taken during the measurement period. The accepted thresholds for the CIE (international Commission on Illumination) curve for vision are: scotopic = illuminance levels below 0.05 lux, photopic = illuminance levels above 50 lux (National Physical Laboratory, London, United Kingdom). Statistical analysis was performed with Matlab® R2014b (The MathWorks, Version 8.4.0). All data were not normally distributed, so non parametric tests were performed.
Results
This cross-sectional study analysed 484 eyes of 242 patients with retinal disorders, 107 male and 135 female. The mean age was 73.8 ± 12 years; participants ranged in age from 45-92 years. The healthy control group had 342 eyes of 171 participants, 84 male and 87 female. The mean age was 61.4 ± 12.5 years; participants ranged in age from 40-87 years.
On average, at the group with retinal disorders pupil diameter decreased with increasing light intensities, with a mean pupil diameter of 4.66 ± 1.03 mm at 0 lux, 4.52 ± 1.01 mm at 0.5 lux, 3.99 ± 0.90 mm at 4 lux, 3.34 ± 0.73 mm at 32 lux and 2.71 ± 0.49 mm at 250 lux illumination.
At the healthy control group, pupil diameter also decreased with increasing light intensities, with a mean pupil diameter of 4.98 ± 0.9 mm at 0 lux, 4.84 ± 1.01 mm at 0.5 lux, 4.35 ± 1.03 mm at 4 lux, 3.51 ± 0.96 mm at 32 lux and 2.75 ± 0.74 mm at 250 lux illumination. In comparison to the patient group, there was a statistically significant larger pupil size at all illumination levels, except 250 lux (p<0.05, Kruskal Wallis test).
We subdivided the patient group into diagnosis groups of diabetes mellitus (DM) (n=134), age-related macular degeneration (AMD) (n=274) andretinal vein occlusion (RVO) (n=76). There was a statistically significant smaller pupil size at the DM-group in comparison to AMD, RVO and control group at all illumination levels, except 250 lux (p=0.04, Kruskal Wallis test) (Table 1). The differences in pupil size at the subgroups were higher at scotopic and low mesopic conditions (0, 0.5 lux). There was no statistically significant difference in pupil size of RVO and AMD in comparison to the control group. The linear plot analysis illustrates these results of a statistically significant difference in the pupil size between the diagnosis groups (Figure 1).
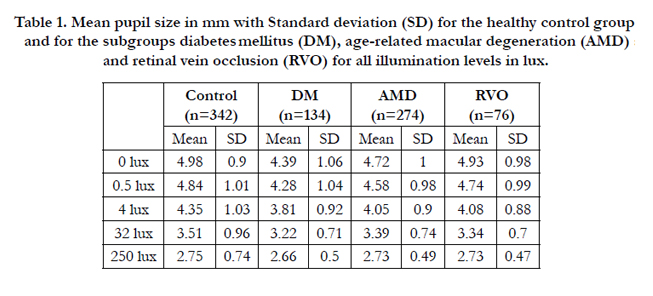

Table 1. Mean pupil size in mm with Standard deviation (SD) for the healthy control group and for the subgroups diabetes mellitus (DM), age-related macular degeneration (AMD) and retinal vein occlusion (RVO) for all illumination levels in lux.
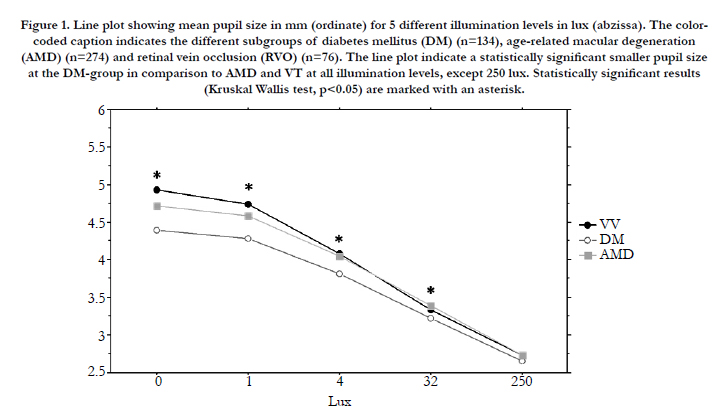
Figure 1: Line plot showing mean pupil size in mm (ordinate) for 5 different illumination levels in lux (abzissa). The color-coded caption indicates the different subgroups of diabetes mellitus (DM) (n=134), age-related macular degeneration (AMD) (n=274) and retinal vein occlusion (RVO) (n=76). The line plot indicate a statistically significant smaller pupil size at the DM-group in comparison to AMD and VT at all illumination levels, except 250 lux. Statistically significant results (Kruskal Wallis test, p<0.05) are marked with an asterisk.
Sub dividing the subgroups, we found no statistically significant difference in pupil size between central vein occlusion (n=50) versus branch retinal vein occlusion (n=26) (p=0.68, Mann- Whitney-U-Test). Non perfusion areas were already treated with panretinal photocoagulation before. Those ischemic group (n=58) versus non-ischemic group (n=18) had no statistically significant difference in pupil size (p=0.83, Mann-Whitney-U-Test). Even so was no statistically significant difference in pupil size between the diabetic groups of mild non-proliferative (n=88) versus severe non-proliferative diabetic retinopathy (n=46) (p=0.59, Mann- Whitney-U-Test).
We found no statistically significant difference ofanisocoriain the subgroups at all illumination levels (p=0.3, Kruskal Wallis test). The pupil size decreases symmetric with increasing illumination level at all subgroups.
Discussion
This study provides data of pupil size for patients with diabetic macular edema (DM), exsudative age-related macular degeneration (AMD) or macular edema caused by retinal venous occlusion (RVO) at scotopic, mesopic and photopic illuminance conditions in comparison to a control group. There was a significant smaller pupil size at scotopic and mesopic illumination conditions at the DM-group in comparison to AMD, RVO and the control group. This is consistent with previous studies [4, 7, 8].
Patients with diabetes mellitus are known to have sympathetic and parasympathetic dysfunction, evidenced by diminished amplitude reflexes and significant smaller pupil diameter [1]. Autonomic neuropathy is a common and serious complication of diabetes. The pupillary autonomic dysfunction is suggested to occur before a more generalized involvement of the autonomic nervous system [1]. Therefore, an early detection is essential to enable appropriate interventional therapy and management [5]. Pena et al., showed that pupillometry appears to be an even more sensitive test of automatic nerve dysfunction in patients with diabetes than assessment of cardiovascular reflexes [9]. Therefore pupillometry could be used to detect early autonomic dysfunction [1, 4]. In comparison with these suggestions, we could also recommend to use pupillometry because of noninvasive and easy handling. However, a more specific study protocol in comparison to further autonomic dysfunction tests might be necessary.
It is well known, that diabetic patients have a significantly smaller median pupillary diameter in relation to healthy subjects [4, 7, 8]. This study is in accordance with these results. Previous studies could show that the constriction velocity and amplitude of pupil size is decreased in patients with diabetes and furthermore highly correlated with the severity of diabetic retinopathy [5, 9-11]. Ko et al., specified that the pupillary diameter is significantly related to diabetes duration, HbA1c, systolic and diastolic blood pressure and albumin/creatinine ratio [4]. Further internal medicine associated study protocols might be interesting with that new device.
This study found no statistically significant difference in the pupil size between AMD and the control group. However, Aspinall et al. found a significantly greater pupil diameter in the early AMD group compared with the control group at a navigation test [12].
A strong correlation of relative afferent pupil defect with the area of retinal ischaemia is already known [13]. Furthermore the relative afferent pupil defect is a reliable indicator for early differentiation of ischemic from non-ischemic central retinal vein occlusion [14]. Patients who developed rubeosis had significantly greater differences of latency rate, maximum and minimum pupillary diameters than patients without rubeosis [14]. Bloom et al., concluded that the pupillary reaction has a relationship to the development of rubeosis, and might be useful in planning the follow up of these patients, like deciding whether to apply panretinal photocoagulation [15]. Our study did not find a difference in pupil size in patients with macular oedema caused by RVO. However, all patients did not have a rubeosisiridis and non perfusion areas were already treated by panretinal photocoagulation.
Conclusion
This study provides comparative data for pupil size at different retinal diseases at different illumination conditions measured with PupilX. Clinical relevant is just the smaller pupil size at diabetes patients. We confirm using pupillometry as a noninvasive and simple tool for additive detection of autonomic dysfunction in patients with diabetic mellitus. However further internal medicine associated study protocols should be investigated.
Acknowledgements
We thank Axel von Wallfeld (MEye Tech GmbH) for material and technical support.
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript. Concluding there is no conflict of interest.
References
- Giselle L Ferrari, Jefferson LB Marques, Rajiv A Gandhi, Simon R Heller, Fábio K Schneider, et al., (2010) Using dynamic pupillometry as a simple screening tool to detect autonomic neuropathy in patients with diabetes: a pilot study. Biomed Eng Online 9: 26.
- Levy DM, Rowley DA, Abraham RR. (1992) Portable infrared pupillometry using Pupilscan: relation to somatic and autonomic nerve function in diabetes mellitus. Clin Auton Res. 2(5): 335-41.
- Yuan D, Spaeth EB, Vernino S, Muppidi S (2014) Disproportionate pupillary involvement in diabetic autonomic neuropathy. Clin Auton Res. 24(6):305-9.
- Ko ML, Chen YY, Ouyang Y, Huang TW, Tsuen BS, et al., (2014) Design and analysis of wearable pupillometer for autonomic neuropathy of diabetic patients. Appl Opt. 53(29):H27-34.
- Ferrari GL, Marques JL, Gandhi RA, Emery CJ, Tesfaye S, et al., (2007) An approach to the assessment of diabetic neuropathy based on dynamic pupillometry. Conf Proc IEEE Eng Med Biol Soc. 557-60.
- Schilde, Bende, Matallana, Kohlhaas. (2013) Messung des Pupillendurchmessers. Der Augenspiegel 32-34.
- Karachaliou F, Karavanaki K, Greenwood R, Baum JD (1997) Consistency of pupillary abnormality in children and adolescents with diabetes. Diabet Med. 14(10): 849-53.
- Karavanaki K, Davies AG, Hunt LP, Morgan MH, Baum JD (1994) Pupil size in diabetes. Arch Dis Child. 71(6):511-5.
- Pena MM, Donaghue KC, Fung AT, Bonney M, Schwingshandl J, et al. (1995) The prospective assessment of autonomic nerve function by pupillometry in adolescents with type 1 diabetes mellitus. Diabet Med. 12(10):868-73.
- Hayashi K, Hayashi H (2004) Pupil size before and after phacoemulsification in nondiabetic and diabetic patients. J Cataract Refract Surg. 30(12):2543- 50.
- Ortube MC, Kiderman A, Eydelman Y, Yu F, Aguilar N, et al., (2013) Comparative regional pupillography as a noninvasive biosensor screening method for diabetic retinopathy. Invest Ophthalmol Vis Sci. 54(1): 9-18.
- Aspinall PA, Borooah S, Al Alouch C, Roe J, Laude A, et al., (2014) Gaze and pupil changes during navigation in age-related macular degeneration. Br J Ophthalmol. 98(10):1393-7.
- Grey RH, Bloom PA (1991) Retinal ischaemia and relative afferent pupil defects in central retinal vein occlusion. Eur J Ophthalmol.1(2):85-8.
- Menon V, Nachiketa MS, Kumar A (1995) Relative afferent pupillary defect and edge light pupil cycle time in the early differentiation of central retinal vein occlusion. Indian J Ophthalmol. 43(3):127-30.
- Bloom PA, Papakostopoulos D, Gogolitsyn Y, Leenderz JA, Papakostopoulos S, et al., (1993) Clinical and infrared pupillometry in central retinal vein occlusion. Br J Ophthalmol. 77(2):75-80.





