Sympathetic Ophthalmia as a Major Sight-threatening Disorder
Mohammed A
Department of Ophthalmology, King Fahd Specialist Hospital, Tabuk, Saudi Arabia.
*Corresponding Author
Mohammed Alkhaibari, MD,
Department of Ophthalmology ,
King Fahd Specialist Hospital,
Tabuk , Saudi Arabia.
Tel: 501343132.
E-mail: m.s.a.007@hotmail.com
Received: April 07, 2016; Accepted: May 18, 2016; Published: May 23, 2016
Citation: Mohammed A (2016) Sympathetic Ophthalmia as a Major Sight-threatening Disorder. Int J Ophthalmol Eye Res. 4(4), 202-205.DOI : dx.doi.org/10.19070/2332-290X-1500041
Copyright : Mohammed A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Sympathetic Ophthalma: Iris and eyeball inflammatory condition affecting both eyes that occurs after a penetrating injury as a delayed autoimmune reaction to eye injury. Patients present with pain, photophobia, paresis of accommodation, metamorphopsia and mild to significant visual loss. The granulomatous anterior uveitis is accompanied by posterior segment findings including moderate to severe vitritis, choroiditis, papillitis, perivasculitis, and yellow-white lesions of the retinal pigment epithelium (Dalen-Fuchs nodules). The inflammation can lead to serious retinal detachment and macular edema. Extraocular symptoms include headache, meningitis or cerebrospinal fluid pleocytosis, hearing loss, poliosis and vitiligo.
The inflammation is caused by a cell-mediated immune mechanism and autoimmune inflammatory response directed against ocular self-antigens released after the initial injury. SO may occur after ocular trauma (47 to 65 % of patients) or contusions. Wounds involving the ciliary body are associated with the highest risk. Surgical interventions may also trigger SO, with posterior segment surgery carrying a higher risk than anterior segment surgery.
Diagnosis of SO is mainly based on patient history and clinical presentation. Imaging studies (fluorescein or indocyanine green angiography, B-scan ultrasonography and optical coherence tomography) may be useful to confirm the diagnosis.
2.Introduction
3.Clinical Feature
3.1.Ophthalmic
3.2.Systemic
4.Work-Up
5.Pathology
5.Deferential Diagnosis
6.Conclusion
7.References
Keywords
Sympathetic Ophthalmia; SO; Vogt– Koyanagi–Harada Syndrome; VKH; Ophthalmic Injuries; Ocular Trauma.
Introduction
Definition: Sympathetic ophthalmia is defined as a rare and Specificbilateral granulomatous pan-uveitis that occurs after the uvea of one eye (inflammation of the uveal tract due to chronic irritation [1]. is subjected to a penetrating injury due to either accidental trauma or surgery, that develops in the normal fellow eye [2]. It's bears remarkable parallels to VKH (Vogt– Koyanagi–Harada Syndrome) but differs in being causally related to antecedent ocular trauma or surgery. Although this response to injury can occur within a few days or over 60 years later, it usually arises between 1 and 12 months after injury [3].
The injured eye is termed the “exciting” eye and the non-injured eye is referred to the “sympathizing” eye [4].
The term “sympathetic ophthalmia” was coined by Mackenzie in the first half of the 19th century [5].
Prevalence: Difficult to measure because it has always been a relatively rare disease; as a result of improvements in modern surgical and medical treatment, it has become even more uncommon [5].
Etiology: Sympathetic uveitis can occur in an otherwise unaffected eye even years after penetrating injuries or intraocular surgery in the fellow eye, especially where there was chronic irritation. Tissues in the injured eye (uveal tract, lens, and retina) act as antigens and provoke an autoimmune disorder in the unaffected eye [1].
Pathogenesis: Approximately two-thirds of SO cases occur within the period of two weeks to two months following injury, with 90% occurring within the first year. Usually patients notice blurry vision and pain in both eyes without other symptoms outside the eyes. Eye examination usually shows red and painful eyes with a swollen middle layer of the eye [4].
It has long been thought that uveal pigment is somehow released by trauma and incites an inflammatory reaction [5]:
- Neurogenic (extension from one eye to the other through the optic nerves or via the ciliary nerves)
- Infectious theory: tuberculosis, Actinomyces, Rickettsia, virus
- Combined ciliary nerve and bacterial theories
- Allergic or Anaphylactic theory: Autoimmunity against uveal melanin, uveal melanocytes, retinal pigment epithelium, or retinal antigens (S & IRBP)
- Role of Ocular Immune Privilege
Clinical Feature
The earliest symptoms include limited range of accommodation and photophobia. Later there is diminished visual acuity and pain [1]. Bilateral eye pain, photophobia, decreased vision (near vision is often affected before distance vision), red eye. A history of penetrating trauma or intraocular surgery (most commonly vitreoretinal surgery) to one eye (usually 4 to 8 weeks before, but the range is from 5 days to 66 years, with 90% occurring within 1 year) may be elicited [6].
- Anterior: bilateral granulomatous anterior uveitis with mutton-fat keratic precipitates (KP), posterior synechiae. Bilateral severe anterior chamber reaction with large muttonfat KP; may have asymmetric involvement with typically more reaction in sympathetic eye.
- Posterior: vitritis, choroidal infiltration, Dalen–Fuchs nodules, macular edema, exudative retinal detachment; the inciting eye may be phthisical.Posterior segment findings include small depigmented nodules at the level of the retinal pigment epithelium (Dalen–Fuchs nodules), and thickening of the uveal tract.
- Complications: cataract, secondary glaucoma, end-stage disease (optic atrophy, chorioretinal scarring).
Features are the same as for VKH, but systemic involvement is less common.
Critical Suspect any inflammation in the uninvolved eye after unilateral ocular trauma. Signs of previous injury or surgery in one eye are usually present.
Nodular infiltration of the iris, peripheral anterior synechiae, neovascularization of the iris, occlusion and seclusion of the pupil, cataract, exudative retinal detachment, papillitis.
The earliest sign may be loss of accommodation or a mild anterior or posterior uveitis in the uninjured eye [6].
The disorder has a chronic clinical course and may involve severe complications of uveitis such as secondary glaucoma, 8 Uveal Tract (Vascular pigmented layer) secondary cataract, retinal detachment, and shrinkage of the eyeball. Sympathetic ophthalmia can lead to blindness in particularly severe cases.
When the injured eye is blind, prophylactic enucleation is indicated before the onset of sympathetic ophthalmia in the fellow eye. An early sign of sympathetic ophthalmia is a limited range of accommodation with photophobia [1].
There are no tests that can tell an eye doctor without a doubt that a patient has SO. However, a history of eye injury or surgery combined with the finding of inflammation in both eyes raises SO as a possible diagnosis. The eye doctor will obtain a complete history and perform a careful examination of the eyes, including tests of vision, eye pressure, and inflammation in the eye, using special instruments which magnify the dilated eyes under bright light. Special testing such as fluorescein angiograms, indocyanine green angiography, or ultrasound may be performed. The eye doctor will likely obtain blood tests and a chest X-ray to ensure that other diseases which may look similar to SO are not present. Some of these include Vogt-Koyanagi-Harada disease, sarcoidosis, intraocular lymphoma, and the white dot syndromes [7].
Patients will have bilateral uveitis with mutton fat keratic precipitates along with variable inflammation of the choroid manifesting as vitritis, optic nerve swelling (papillitis), and choroiditis [8]. Patients classically have exudative retinal detachments that are visible on dilated fundus exam and can be captured on optical coherence tomography. These areas of serous retinal detachments correspond to pinpoint hyperfluorescence and leakage on fluorescein angiogram [9].
Work-Up [6]
- History: Any prior eye surgery or injury, Venereal disease,Difficulty breathing.
- Complete ophthalmic examination, including a dilated retinal examination.
- CBC, RPR, FTA-ABS, and ACE level.
- Consider a chest radiograph to evaluate for tuberculosis or sarcoidosis.
- IVFA or B-scan US, or both, to help confirm the diagnosis.
Pathology [4]
The inflammatory changes in the exciting and sympathizing eyes are the same, except for features of trauma in the exciting eye.
Granulomatous Uveitis: The minimal and classic changes for the histopathologic diagnosis of sympathetic ophthalmia are diffuse lymphocytic infiltration of the uveal tract with epithelioid cell nests, pigment phagocytosis by the epithelioid cells, absence of necrosis, and sparing of the retina and choriocapillaris by the granulomatous process.
The uveal tract is usually diffusely thickened (massively in some) by an infiltration of lymphocytes in which various numbers of nests of epithelioid cells displaying pigment phagocytosis are present.
Atypical Pathologic Features
- Focal nongranulomatous to diffuse non-necrotizing granulomatous infiltrate
- Focal choriocapillary involvement
- Chorioretinal adhesions
- Retinal detachment
- Optic atrophy
- Retinal perivasculitis
- Mild inflammatory involvement of the meninges
- Preferential anterior segment inflammation
- VKH syndrome: Similar signs, but no history of ocular trauma or surgery. Other systemic symptoms. See table, Vogt– Koyanagi–Harada Syndrome.
- Phacoanaphylactic endophthalmitis: Severe anterior chamber reaction from injury to the lens capsule. Contralateral eye is uninvolved. Lens-Induced (Phacogenic) Glaucoma.
- Sarcoidosis: Often elevated ACE level. May cause a bilateral granulomatous pan-uveitis.
- Syphilis: Positive FTA-ABS. May cause bilateral granulomatous pan-uveitis.
- Tuberculosis: Positive PPD and CXR. May cause bilateral granulomatous pan-uveitis.
- Other granulomatous uveitis induced by mycobacteria or fungi
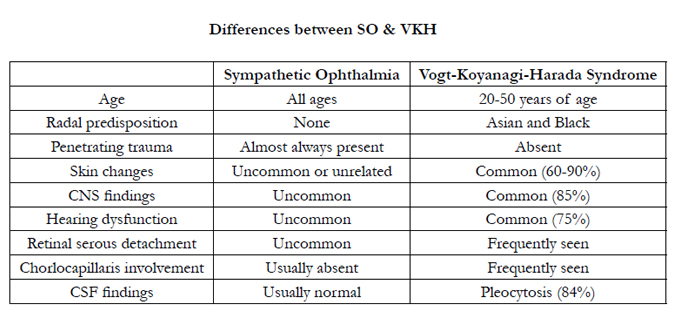

Differences between SO & VKH
Treatment: The risk of this increases if a penetrating eye injury is left untreated. All penetrating eye injuries should receive immediate specialist ophthalmic management without delay. Treatment typically requires oral corticosteroids (eg, prednisone, 1 mg/kg po once/day) followed by long-term use of a noncorticosteroid immunosuppressive drug. Prophylactic enucleation of a severely injured eye should be considered within 2 weeks of vision loss to minimize the risk of sympathetic ophthalmia developing in the other eye, but only when the injured eye has no vision potential [10]. Some patients may require admission to the hospital to receive medications through their veins. SO can be a difficult disease to treat and may require additional therapy, including the use of more than one immunosuppressive medication [7].
Prognosis: SO remains a serious disease that may result in a very poor visual outcome without therapeutic intervention. Some studies suggest that SO may be more aggressive in African Americans. When diagnosed early and treated appropriately, patients with SO have a good chance of retaining useful vision [7]. Sympathetic Ophthalmia is a serious vision-threatening disease. Half of all patients will have 20/40 or worse vision and one third of all patients will end up legally blind [11]. Complications include macular edema, CNV, and continued inflammation [12].
Conclusion
SO is a rare disease, and it is one of major sight-threatening disorder.it has a high index of suspicion must be maintained whenever inflammation occurs in fellow eyes of an eye that has suffered penetrating trauma or intraocular surgery.
Diagnosis is made clinically, histological proof is not required. The injured eyes which have potential vision should not be enucleated in an attempt to prevent or lessen SO or to provide confirmatory pathology.
Prognosis was considered poor prior to the use of systemic immunosuppression. Today, it should no longer be regarded as a blinding disease. Prompt and adequate systemic immunosuppressive therapy with systemic steroids and steroidsparing agents has improved prognosis
References
- Gerhard K Lang (2000) Ophthalmology a Short Textbook. chapter 8 Uveal Tract (vascular pigmented layer). 214.
- PT Khaw ,P Shah, AR Elkington (2004) ABC of eye, acute visual disturbance. (4th edn), BMJ Publishing Group, London. 32.
- Tsai J, Denniston A, Murray P, Huang J, Aldad T (2010) Oxford American handbook of ophthalmology. Oxford University Press,New York. 344.
- Chi-Chao Chan (2003) Sympathetic Ophthalmia. A Patient Education Monograph prepared for the American Uveitis Society. National. National Eye Institute/National Institutes of Health Bethesda, USA. 1-2.
- Rajesh Babu B,Lecture presentation of Uveitis, Ocular Immunology &Ocular Epidemiology for Community Eye Health.
- Adam T Gerstenblith, Michael P Rabinowitz (2012) The Wills eye manual: office and emergency room diagnosis and treatment of eye disease. (6th edn),Lippincott Williams & Wilkins, Philadelphia. 392-393
- Chi-Chao Chan (2003) A Patient Education Monograph prepared for the American Uveitis Society, National Eye Institute/National Institutes of Health.
- Gupta V, Gupta A, Dogra MR (2008) Posterior sympathetic ophthalmia: a single centre long-term study of 40 patients from North India. Eye 22(12): 1459–1464.
- American Academy of Ophthalmology Eyewiki
- Emmett T. Cunningham (2014) Sympathetic Ophthalmia.Merck Manual professional version.
- Chan CC, Roberge RG, Whitcup SM, Nussenblatt RB (1995) Thirty two cases of sympathetic ophthalmia. A retrospective study at the National Eye Institute Bethesda, MD from 1982–1992. Arch Ophthalmol 113(5): 597–600.
- Damico F, Kiss S, Young LH (2005) Sympathetic Ophthalmia. Semin Ophthalmol 20(3): 191–197.





