Endophthalmitis Vitrectomy Study: Effectiveness of Guidelines in Cases of Endophthalmitis Following Manual Small Incision Cataract Surgery
Shah M*, Shah S, Shah A, Kalyani P
Drashti Netralaya, Nr. GIDC, Chakalia Road, Dahod-389151, Gujarat, India.
*Corresponding Author
Mehul Shah,
Drashti Netralaya, Nr. GIDC,
Chakalia Road, Dahod-389151,
Gujarat,India.
Tel: 00-91-2673-645364; Fax: 00-91-2673-221232
E-mail: omtrust@rdiffmail.com
Article Type: Research Article
Received: April 23, 2014; Accepted: June 12, 2014; Published: June 30, 2014
Citation: Shah M, Shah S, Shah A, Kalyani P. (2014). Endophthalmitis Vitrectomy Study: Effectiveness of Guidelines in Cases of Endophthalmitis Following Manual Small Incision Cataract Surgery, Int J Ophthalmol Eye Res, 2(3), 30-33. doi: dx.doi.org/10.19070/2332-290X-140006
Copyright: Shah M© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To validate Endophthalmitis vitrectomy study guidelines in cases of post-operative endophthalmitis following Manual small incision cataract surgery.
Setting: Tertiary eye care centre in western central India.
Participants: 36 eyes with endophthalmitis following Manual small incision cataract surgery.
Methods: We enrolled all post cataract endophthalmitis patients following manual small incision cataract surgery with specific inclusion and exclusion criteria. Treatment planned according to severity as in Endophthalmitis vitrectomy study, all eyes are given intra vitrealvancomycine+ceftazidim injection using standard protocol and dosages. Patients who have visual acuity more than hand motion were treated only with intravitreal injections and patients who had only perception of light undergone vitrectomy. Patients who were not ready for surgical intervention excluded from analyses of visual outcome. Patients were followed up according to standard schedule and protocol.
Results: Our cohort consisted of total 36 cases of acute post-operative endophthalmitis following manual small incision cataract surgery
within six weeks. Our cohort consisted of 20(55.6%) male 16(44.4%) female;the age range was 44 - 85 years with mean age of 56.9 +/- 19.5 years. The mean duration of presentation and duration following cataract surgery was 6.7 +/- 8.1 days and 7.1 +/- 10.9 days respectively.
Visual outcome 11 eyes (42.3%) regained vision more than 20/40 and 15 eyes (57.7%) regained more than 20/60, 20 eyes(76.9%) regained more than 20/200 and 23 eyes (88.4%) regained more than 20/400.
Conclusion: Results and recommendations of Endophthalmitis Vitrectomy Study are very effective and useful in treatment post cataract surgery endophthalmitis by manual small incision cataract surgery.
2.Introduction
3.Method
3.1.Objective
3.2.Methods
3.3.Exclusion
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Endophthalmitis; Manual Small Incision Cataract Surgery; Vitrectomy For Endophthalmitis; Endophthalmitis Vitrectomy Study.
Introduction
Cataracts are responsible for 47% of all cases of blindness worldwide. The epidemiological impacts of cataracts are uneven among different countries, and the rate is associated with economic conditions. In developed countries, where healthcare is good, cataracts account for only 5% of cases of blindness, whereas cataracts are still responsible for 50% of such cases in developing countries. After a brief overview of historical, clinical, and therapeutic aspects, this article presents an update on global epidemiological cataract data. It also provides insight into political, socioeconomic, and cultural factors that adversely affect the availability of healthcare in developing countries, making cataracts a major public health problem and an obstacle to development [1].
Blindness has been recognised as an important publichealth problem in India, [2,3] recently, a nationwide survey was undertaken (1999–2001)to document the current situation, trends over the past threedecades, and to evaluate the impact of the World Banksupported Cataract Blindness Control Project in the country [4].
Estimated cataract blindness rate in India is 1.38% during 2010 As a cataract blindness elimination initiative IAPB and WHO launched VISION 2020 program resulting in increase in Cataract Surgery Rate globally as well as in India [5].
Cataracts are cured by surgery, but this is not equally available, and the surgical methods that are available do not produce equal outcomes. A total of 5,906,016 cataract surgeries were performed worldwide during 2009–2010. The number of cataract surgeries in India was 5156/million during the same period [5].
Monitoring of outcome of surgical treatment of cataract is important and is possible [6].
Surgical techniques used cataract surgery is performed mainly by phacoemulcification, but manual small incision cataract surgery is important technique is being used in developing countries, surgical outcome safety and efficacy also found comparable [7,8].
Cataract surgery may result in to complications, hampering visual improvement. Post-operative endophthalmitis is one of the most serious complications of cataract surgery. [9,10] Incidence of Post cataract surgery Endophthalmitis varies from0.05 to 0.17 [11,12,13] Variations may be according to transition in surgical techniques and minimal reported with injectable intra ocular lens [12]
Treatment of post-operative endophthalmitis varies may be in form of intravitreal injection, topical treatment or surgery. [14,15,16,17]
Treatment of acute post-operativeendophthalmitis is standardized following Endophthalmitis Vitrectomy Study [18]. Are many studies favouring [19,20] or opposing Endophthalmitis Vitrectomy Study [21,22].
Endophthalmitis vitrectomy study has standardized treatment for post cataract endophthalmitis but did not specify about surgical techniques, since surgical technique is different pathophysiology and results of complications also different.
We would like to validate results of Endophthalmitis Vitrectomy Study in case of manual small incision cataract surgery. [18]
Method
Evaluate treatment guidelines ofEndophthalmitis vitrectomy study how much effective for manual Small incision cataract surgery which is being performed in large number of cases.
Inclusion post cataract surgery patients presenting with acute post-operative infection causing severe visual impairment within six weeks.
Any other surgery, previous treatment of endophthalmitis done.
Our institution is a referral tertiary centre we keep getting referrals from various secondary centers, we have enrolled cases from 2009 to 2012.
When patient with similar criteria presented enrolled for study.Detailed history and examination done.
Anterior segment examination done with slit lamp and documented in online pre tested format. Specific documentation about main incision, side port, aqueous flare, aqueous cells, exudates in anterior chamber, membrane over intraocular lens, hypopyon, corneal condition including edema and infiltrate studied and documented. Posterior segment examination performed indirect ophthalmoscope, Fundal glow evaluated if possible if no glow found patient subjected to B scan and findings evaluated. [23].
Treatment planned according to severity as in Endophthalmitis vitrectomy study, all eyes are given intra vitreal vancomycine and ceftazidim injection using standard protocol and dosages. Patients who have visual acuity more than hand motion were treated only with intravitreal injections and patients who had only perception of light undergone vitrectomy. Patients who were not ready for surgical intervention excluded from analyses of visual outcome. Patients undergoing surgeries treated by pars plana vitrectomy using 23 or 20 g vitrectomy and wide angle non-contact viewing system.
Eyes grouped according to immediate surgical intervention done or not.
Data Collection done in excel sheet after exported from online pre tested format. Data opened in spss is 15 and using descriptive analyses frequency counted stastical analyses done using cross tabulation and chi square test.
Results
Our cohort consisted of total 36 cases of acute post-operative endophthalmitis following manual small incision cataract surgery within six weeks. Our cohort consisted of 20(55.6%) male 16 (44.4%) female;the age range was 44 - 85 years with mean age of 56.9 +/- 19.5 years. The mean duration of presentation and duration following cataract surgery was 6.7 +/- 8.1 days and 7.1 +/- 10.9 days respectively.
Mean follow up duration was 6 months.
17(47.2%) undergone pars plana vitrectomy10(27.8%) did not agree for further intervention9(%) treated only with intra vitreal vancomycine injection.
We have studied clinical finding specific to manual small incision cataract surgery and found infiltration of main wound and side port. (Table.1)
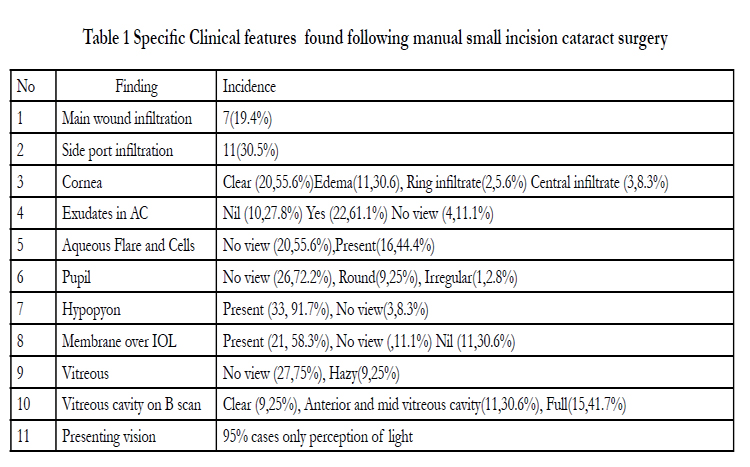

Table 1 Specific Clinical features found following manual small incision cataract surgery
We have done comparative study of different variables and did not find making significant difference in post treatment outcome. (Table.2)
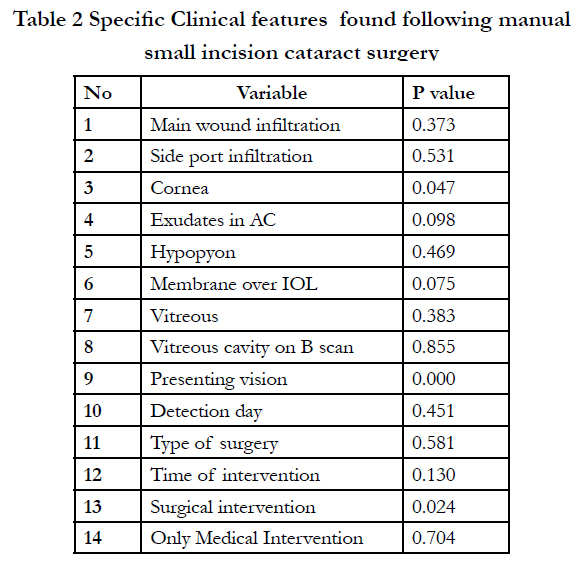
Table 2 Specific Clinical features found following manual small incision cataract surgery
Visual outcome 11 eyes (42.3%) regained vision more than 20/40 and 15 eyes (57.7%) regained more than 20/60, 20 eyes(76.9%) regained more than 20/200 and 23 eyes (88.4%) regained more than 20/400.(Table.3)
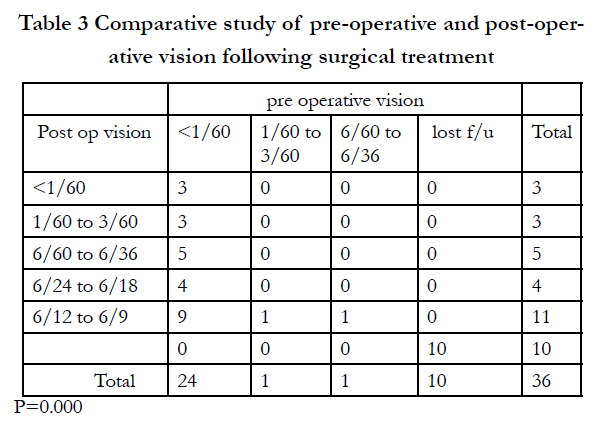
Table 3 Comparative study of pre-operative and post-operative vision following surgical treatment
We have done comparative study of pre and post treatment visual outcome we found significant difference concluding our treatment has done significant difference.(Table.3) When we studied comparatively two groups we found group with surgical intervention has better outcome.(Table.4 P=0.000)
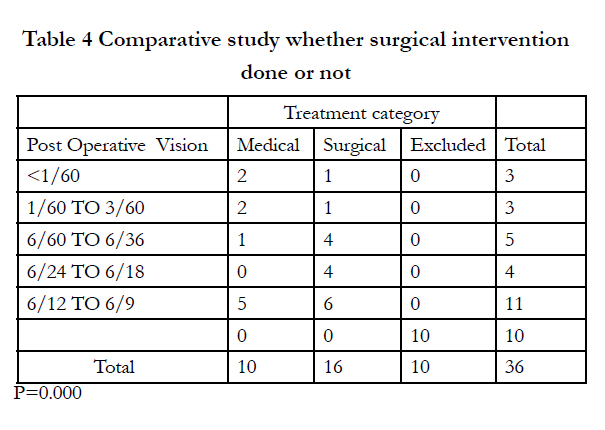
Table 4 Comparative study whether surgical intervention done or not
We have also studied reason for no improvement in visual acuity. Our patients presented with very poor visual acuity 95% patients presented with vision of perception of light.
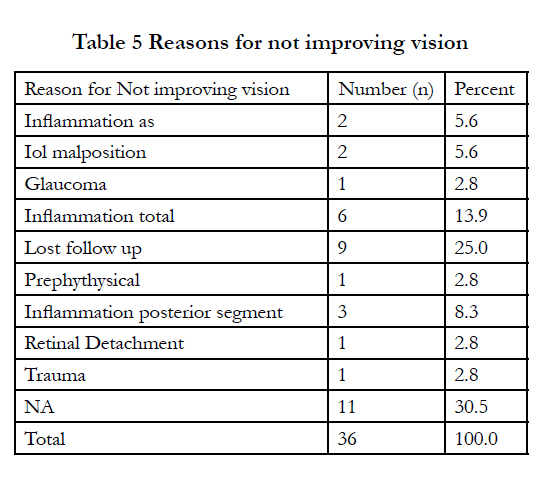
Table 5 Reasons for not improving vision
Discussion
Manual small incision cataract surgery is a popular surgical technique for high volume cataract surgeries in developing countries with comparable safety and efficacy [7,8].
Endophthalmitis vitrectomy study has been studied for treatment for post cataract endophthalmitis but did not specify about surgical techniques, since surgical technique is different pathophysiology ocular and visual outcome may differ.
Wongreported incidence of endophthalmitis increased with phacoemulcification [13] Strmen, P., K. Hlavackovareported reduced after injectable intra ocular lens [14].
When we have followed guidelines of endophthalmitis vitrectomy study for manual small incision cataract surgery We have performed pars plana vitrectomy in 47% of our patients and regained 20/400 in 88.4% of cases at end of 6 months.(Table.3) thapa reported improvement in 67.7%[25], malhotra reported improvement in 33%[26], Strmen, P., K. Hlavackova[14] reported 6/36 in 50% eyes, Doft, B. H., S. F. Kelsey At the 9-month visit, visual acuity was 20/50 or better in 49% of all eyes, 20/200 or better in 79%, and 5/200 or better in 91%.[27].
We observed specific findings in endophthalmitis following manual Small Incision Cataract Surgery infiltration of main wound and side port which is not reported till now but has not caused significant difference in visual outcome(Table-2).
We reported central corneal infiltrates and ring infiltrates causing significant difference in visual outcome, Malhotra reported similar finding not causing significant difference in visual outcome. [26]
Kodjikian, L., A. Salvanet-Bouccara, reported presenting visual acuity 5/200 or more in 18.9% compared to only perception of light in 95% eyes in our study, may reduce number of vitrectomies according to Endophthalmitis vitrectomy study [28].
Versteegh, M. F., J. M. Hooymans, reported After treatment a visual acuity of 0.1 or more was achieved in 62% of the patients. The best final results were achieved in the patients with an initial visual acuity of 1/300 or more [15].
Strmen, P., K. Hlavackova, reported the final visual acuity was better than 2/60 in70% of the eyes and better than 6/36 in 50% of the eyes without vitrectomy. [14].
Doft, B. H., S. F. KelseyBermig, J., P. Meier, Meier, P. And P. Wiedemann ,Talley, A. R., D. J. D'Amico, reported that intravitreal antibiotics and pars plana vitrectomy according to Endophthalmitis vitrectomy study guidelines has better visual outcome and functional success in cases of post cataract surgery endophthalmitis, Which are supporting our results.[27,29,30,31]
Conclusion
Results and recommendations of Endophthalmitis vitrectomy study are very effective and useful in treatment post cataract surgery endophthalmitis by manual small incision cataract surgery.
References
- Lawani R, Pommier S, Roux L, Chazalon E, Meyer F (2007) Magnitude and strategies of cataract management in the world. Med Trop (Mars) 67:644-50.
- Dandona L, Dandona R, Naduvilath TJ (1998) Is current eye-care-policy focus almost exclusively on cataract adequate to deal with blindness in India? Lancet 351:312–16.
- Thulasiraj RD, Nirmalan PK, Ramakrishna R (2003) Blindness and vision impairment in a rural south Indian population: the Aravind Comprehensive Eye Survey. Ophthalmology 110:1491–8.
- Jose R, Bachani D (1995) World Bank assisted cataract blindness control project. Indian J Ophthalmol 43:35–43.
- Murthy G, Gupta SK, John N, Vashist P (2008) Current status of cataract blindness and Vision 2020: the right to sight initiative in India. Indian J Ophthalmol 56:489-94.
- (1999) Bulletin of the World Health Organization 77 (6)
- Hennig A, Kumar J, Yorston D, Foster A (2003) Sutureless cataract surgery with nucleus extraction: outcome of a prospective study in Nepal. Br J Ophthalmol 87:266–270.
- Gogate PM, Kulkarni SR, Krishnaiah S, Deshpande RD, Joshi SA, Palimkar A, et al. (2005) Safety and efficacy of phacoemulsification compared with manual small incision cataract surgery by a randomized controlled clinical trial: six-week results. Ophthalmology 112: 869–74
- Bourne RR, Dineen BP, Ali SM, Huq DM, Johnson GJ (2003) Outcomes of cataract surgery in Bangladesh: results from a population based nationwide survey. Br J Ophthalmol 87: 813–9.
- Mathenge W, Kuper H, Limburg H, Polack S, Onyango O, Nyaga G, et al.( 2007) Rapid assessment of avoidable blindness in Nakuru district, Kenya. Ophthalmology 114: 599–605.
- Norregaard J. C, H. Thoning (1997) Risk of endophthalmitis after cataract extraction: results from the International Cataract Surgery Outcomes study. Br J Ophthalmol 81(2): 102-6.
- Mayer E, D. Cadman (2003) A 10 year retrospective survey of cataract surgery and endophthalmitis in a single eye unit: injectable lenses lower the incidence of endophthalmitis. Br J Ophthalmol 87(7): 867-9.
- Wong T. Y, S. P. Chee (2004) The epidemiology of acute endophthalmitis after cataract surgery in an Asian population. Ophthalmology 111(4): 699-705
- Strmen P, K. Hlavackova (1998) Endophthalmitis after lens surgery. Cesk- SlovOftalmol 54(3): 141-7.
- Versteegh M. F, J. M. Hooymans (2000). Acute bacterial endophthalmitis after cataract extraction: results of treatment. Doc Ophthalmol 100(1): 7-15.
- Bermig J, P. Meier (1997) Primary vitrectomy in endophthalmitis. Ophthalmologe 94(8): 552-6.
- Ozer-Arasli A, O. Schwenn (1997) Endophthalmitis after cataract surgery: long-term follow-up. Klin Monbl Augenheilkd 211(3): 178-82.
- (1995) Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Arch Ophthalmol 113(12): 1479-96.
- Doft B. H, S. F. Kelsey (1994) Treatment of endophthalmitis after cataract extraction. Retina 14(4): 297-304.
- Doft B. H. (1991) the endophthalmitis vitrectomies study. Arch Ophthalmol 109(4): 487-9.
- Siddiqui F, C. Crippen (2002) Do we heed the endophthalmitis vitrectomy study in Canada. Can J Ophthalmol 37(7): 395-8.
- Kaynak S, F. H. Oner (2003) surgical management of postoperative endophthalmitis: comparison of 2 techniques. J Cataract Refract Surg 29(5): 966-9
- Huang J, Z. Wang (2004) Diagnostic ultrasound and pars plana vitrectomy in endophthalmitis. Yan Ke Xue Bao 20(3): 149-54.
- Wong T. Y, S. P. Chee (2004) the epidemiology of acute endophthalmitis after cataract surgery in an Asian population. Ophthalmology 111(4): 699-705.
- Thapa R, G. Paudyal (2011) Clinical profile and visual outcome following pars plana vitrectomy in acute post-operative endophthalmitis. Nepal J Ophthalmol 3(2): 102-8.
- Malhotra S, P. Mandal (2008) Clinical profile and visual outcome in cluster endophthalmitis following cataract surgery in Central India. Indian J Ophthalmol56(2): 157-8.
- Doft B. H, S. F. Kelsey (1994) Treatment of endophthalmitis after cataract extraction. Retina 14(4): 297-304.
- Kodjikian L, A. Salvanet-Bouccara (2009) Postcataract acute endophthalmitis in France: national prospective survey. J Cataract Refract Surg 35(1):89-97.
- Bermig J, P. Meier (1997) Primary vitrectomy in endophthalmitis. Ophthalmologe 94(8): 552-6.
- Meier P, P. Wiedemann (1997) Endophthalmitis--clinical picture, therapy and prevention. Klin Monbl Augenheilkd 210(4): 175-91.
- Talley A. R, D. J. D'Amico (1987) The role of vitrectomy in the treatment of postoperative bacterial endophthalmitis. An experimental study. Arch Ophthalmol 105(12): 1699-702.





