Assessment of Some Heavy Metals, Electrolytes and Nutritional Status of Masons (Cement Brick Layers) in Uromi, Nigeria
Dic-Ijiewere Ebenezer O1*, Okogun GRA2, Akhogba OI2
1 Department of Chemical Pathology, Faculty of Clinical Sciences, Ambrose Alli University, Ekpoma, Nigeria.
2 Department of Medical Laboratory Science, Faculty of Basic Medical Sciences, Ambrose Alli University, Ekpoma, Nigeria.
*Corresponding Author
Dic-Ijiewere Ebenezer O,
Department of Chemical Pathology, Faculty of Clinical Sciences,
Ambrose Alli University, Ekpoma, Nigeria.
E-mail: ebenexar@gmail.com
Received: February 19, 2018 Accepted: May 25, 2018; Published: May 31, 2018
Citation: Dic-Ijiewere Ebenezer O, Okogun GRA, Akhogba OI. Assessment of Some Heavy Metals, Electrolytes and Nutritional Status of Masons (Cement Brick Layers) in Uromi, Nigeria. Int J Natural Disaster Health Secur. 5(1), 36-41. dx.doi.org/10.19070/2572-7540-180007
Copyright:Dic-Ijiewere Ebenezer O© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: This study determined the effect of exposure to cement on plasma concentrations of heavy metals such as Silicon, Aluminium, and Chromium, electrolytes and the effect on nutritional parameters such as Protein (Albumin and globulin), and Total Cholesterol in the plasma of cement handlers from the study area.
Introduction: Production and usage of cement is a dusty industrial process and the health of the workers have been studied for many years and cement dust has been mostly implicated in various associated diseases.
Objective: To determine the level of exposure of cement handlers to the heavy metals commonly present in cement by measuring the plasma concentration, to determine the level of lipid peroxidation by cement components by assessment of the total plasma cholesterol and to determine the health implication of prolonged exposure to cement by assessment of nutritional parameters.
Design: A total of fourty Masons (Popularly referred to as Bricklayers) were randomly selected for the study and twenty controls who were office workers/students not resident in a town were a cement factory is located, and have never worked as cement handlers.
Result: Plasma Aluminium (μg/mL) level was significantly higher for bricklayers of 1-10 years (B1) (0.56 ± 0.08) and bricklayers of >10 years (0.68 ± 0.08), plasma chromium (μg/mL) levels of bricklayers of 1-10 years (0.36 ± 0.06) and bricklayers of >10 years (32 ± 0.05) in comparison with the control (0.31 ± 0.05) was significantly higher. Silicon (μg/mL) levels were not significant for both bricklayers of 1-10 years (0.04 ± 0.05) and bricklayers of >10 years (0.03 ± 0.00). Plasma Magnesium (mmol/l) in comparison with control (0.67 ± 0.11) was significantly higher for bricklayers of 1-10 years (0.76 ± 0.12) and bricklayers of >10 years (0.76 ± 0.07). Plasma Calcium (mg/dl) for bricklayers of 1-10 years (8.62 ± 0.60) was not significant, but significantly higher levels was observed for bricklayers of >10 years (9.99 ± 0.87). Plasma Sodium levels (mmol/l) in comparison with the control (138.30 ± 3.28) was significantly higher for bricklayers of 1-10 years (140.75 ± 2.36), but was statistically not significant for bricklayers of >10 years (139.70 ± 2.64). Potassium (mmol/l) was not signifiant for both groups (3.90 ± 0.21 and 3.91 ± 0.31).Total Protein(g/dl) levels in comparison with control (8.54 ± 1.19) was not significant for both groups..Significantly lower levels of cholesterol (mg/dl) were observed for both groups (138.85 ± 30.07 and 127.00 ± 30.35).
Conclusion: The study revealed that some of the heavy metals and other elements present in the composition of cement such as Chromium, Aluminium, Calcium and Magnesium were detected in significantly higher amounts in the test subjects (Bricklayers) in comparison with the control. Lipid peroxidation may have also occurred as a result of the effect of the heavy metals and other components of cement.
2.Abbreviations
3.Introduction
4.Methods
4.1 Famine-1974 in Bangladesh and entitlement approach
4.2 Ethical Consideration
4.3 Inclusion and Exclusion Criteria
4.4 Sample size
4.5 Sampling Technique
4.6 Analytical Techniques
4.7 Data Collection and Analysis
5.Results
6.Discussion
7.Conclusion
8.References
Keywords
Cement; Bricklayers; Heavy Metals; Aluminium; Silicon; Chromium Magnesium; Electrolytes; Calcium; Sodium; Potassium; Nutritional; Total Protein; Albumin; Globulin; Cholesterol.
Abbreviations
AAS: Atomic Absorption Spectrophotometry; O-CPC: O-Cresolphthalein Complexone; ISEs: Ion-Selective Electrodes; BCG: Bromocresol Green; ANOVA: Analysis Of Variance.
Introduction
Cement is a binder, a substance that sets and hardens and can bind other materials together. The word "cement" can be traced back to the Roman term opus caementicium, used to describe masonry resembling modern concrete that was made from crushed rock with burnt lime as binder. The volcanic ash and pulverized brick supplements that were added to the burnt lime, to obtain a hydraulic binder, were later referred to as cementum, cimentum, cäment, and cement. Production and usage of cement is a dusty industrial process and the health of the workers have been studied for many years. Silica which is a major constituent of cement dust has been mostly implicated [1-3]. Basically, the sections in cement factory can be grouped into crushing, milling and packing sections and each of these sections are known to differ in releasing different toxic constituents [3] with the introduction of various additives and via different mechanical processes [3]. These constituents (such as chromium and silica) when inhaled by cement handlers stimulates inflammatory responses from workplace exposures and result in specific target organs derangement such as the lungs, skin, liver and the immune system might be affected [4].
It has been reported that chronic exposures to aluminum could increase lipid peroxidation in different tissues resulting in neurotoxicity, renal failure and anaemia [5]. Inflammatory response to workplace exposures to silica has been reported to be observed in specific organs, such as lungs, skin and the liver and if persistent may progress to fibrosis, granulomatous diseases and even cancer [6]. Also, chromium is present in cement dust product via scrapes of refractory lining of kiln and steel balls used in the mills [7] and has been reported to be highly toxic and a strong oxidising agent, especially Cr (VI) which is highly present in cement dust due to oxidation, exposure to this Cr (VI) results in toxic effects in vital organs such as respiratory (lungs), kidney and liver [8] via generation of free radicals and resultant inflammatory reactions. Continuous efflux of reactive oxygen species from endogenous and exogenous sources has been known to result in accumulative oxidative damage to cellular component and alters many cellular functions [9, 10].
Heavy metals are relatively dense metals or metalloids that are noted for their potential toxicity, especially in environmental contexts, and generally toxic in low concentrations to plants and animals [11]. The term heavy metal has particular application to Cadmium, Mercury, Lead and Arsenic [12], all of which appear in the World Health Organization’s list of 10 chemicals of major public concern. Others include Chromium, Aluminum, Cobalt, Nickel, Copper, Zinc, Selenium, Silver, Antimony and Thallium [13]. Heavy metals have many industrial uses such as in materials used in the manufacturing of cement, chrome plating, cadmium in nickel based rechargeable batteries. Many chemical and agricultural materials such as Printers dye, organic based paints, tobacco products, metal alloys, automobile waste, insecticides, and herbicides amongst others contain large amounts of heavy metals [14].
The basic components of cement are calcium oxide, silicon dioxide, aluminum trioxide and iron oxide [4]. However, the burning and calcination process of cement produces pollutants such as heavy metals, dioxin, particulates, chromium, sulphur dioxide, nitrogen dioxide and carbon dioxide [15]. These toxic elements and gases have been fingered in a lot of diseases including respiratory diseases, genetic diseases, hematology problems, multiorgan damage and cancer [3]. It has been reported that chronic exposures to aluminium could increase lipid peroxidation in different tissues resulting in neurotoxicity, renal failure and anaemia [5]. Furthermore, various residents of cement plants are protesting against health problems affecting them which they attribute to the quality of the air they breathe in. Despite these claims, cement manufacturers, marketers and building contractors have continued to deny the health effects of their activities. Their argument is being supported by the fact that most of the studies mentioned above were done on the basis of radiology or spirometry [2] which give rooms for controversy. Because the study organism, man, is mobile and could have developed the diseases from other environmental pollutants such as contaminated water, food etc [3].
Therefore, to clear this controversy, a research, assessing the presence of cement components alongside the nutritional and electrolyte status of cement handlers such as masons (brick layers) and cement sales individuals who have spent some time of their life around Cement and cement materials is needed. This is to determine whether these toxic components of cement are present in significant toxic levels in their body and the impact on their nutritional status, and suggest ways to protect these individuals.
This study was carried out in Uromi, Esan North East Local Government Area of Edo State, Nigeria. Edo state lies between longitude 06° 04IE and 06° 43IE and latitude 05° 44IN and 07° 34IN with a land mass of 17,450 sq.km located in the South geopolitical zone of Nigeria. The city of Uromi lies in north-eastern Esan in Edo State, Nigeria, located on longitude 3° 24' E and latitude 6° 27' N. Almost the whole of the city is covered with land. Uromi is an urban town with the major occupation of farming, trading, artisans, civil servants and students [16].
Ethical approval was obtained from the Health Research Ethics Committee of Ambrose Alli University, Ekpoma, Nigeria and informed consent was sought from the various research subjects and control subjects.
Individuals with any acute and chronic illness were excluded from the study. Healthy individuals who had never worked with cement or lived to a cement manufacturing town were included in the study.
A total of fourty Cement handlers or Masons (Popularly referred to as Bricklayers) were randomly selected for the study after obtaining an informed consent and twenty controls who were office workers/students not resident in a town were a cement factory is located, and have never worked as cement handlers. Smokers, alcoholics and those with chronic illnesses were excluded from this study. Questionnaires were administered to obtain vital information.
Simple random sampling technique was used to select the subjects for this research.
Ten milliliter of venous blood was withdrawn and dispensed into Lithium-heparin bottles to obtain plasma.
Calcium, Total Cholesterol, total protein and albumin were determined spectrophotometrically based on standard methods while globulin was computed by subtracting albumin level from total protein concentration.
The samples were analyzed for heavy metals with the help of atomic absorption spectrophotometer as described by Walsh [17], and the concentration of the following; Silicon, Aluminium, Chromium and Magnesium were analyzed.
In practice, Atomic Absorption Spectrophotometry (AAS) methodology entails the aspiration of a sample into a flame, where it becomes atomized. A light beam is directed through the flame into a monochromator and onto a detector. The detector then measures the intensity of light absorbed by the atomized elements in the flame. Thus, the amount of light intensity absorbed in the flame is proportional to the element in the sample.
Measurement of total Calcium was done Spectrophotometrically using the o-cresolphthalein complexone (CPC) alkaline solution. CPC formed a red chromophore with calcium, which was measured at 570 to 580 nm [18]. Ion-selective electrode method (ISEs) was used for the determination of Potassium and Sodium, as described by Csoregi et al., [19].
Total protein was determined colorimetrically using the biuret quantitative test method by Piotrowski [20]. Albumin was determined colorimetrically with the bromocresol green reagent. Albumin binds with bromocresol green (BCG) to produce a bluegreen color with an absorbance maximum at 628 nm [21].
Plasma total Cholesterol was determined colorimetrically using cholesterol oxidase method as described by Allain et al., [22].
The data generated from the study was subjected to basic statistical measurement of central tendency and dispersion, and comparisons was carried out to test for significant differences in the concentration of the heavy metals and other biochemical parameters, using parametric analysis of variance (ANOVA) using the computer SPSS 16.0 windows application.
Results
From Table 1, when the plasma aluminum levels of the bricklayer subjects in the study area were compared with the plasma aluminum levels of the control subjects, It was significantly higher for bricklayers of 1-10 years (B1) and bricklayers of >10 years(fvalue= 27.84, p-value =0.00). Multiple comparisons showed that B1 was also significantly higher in comparison with B2 (p-value= 0.00).
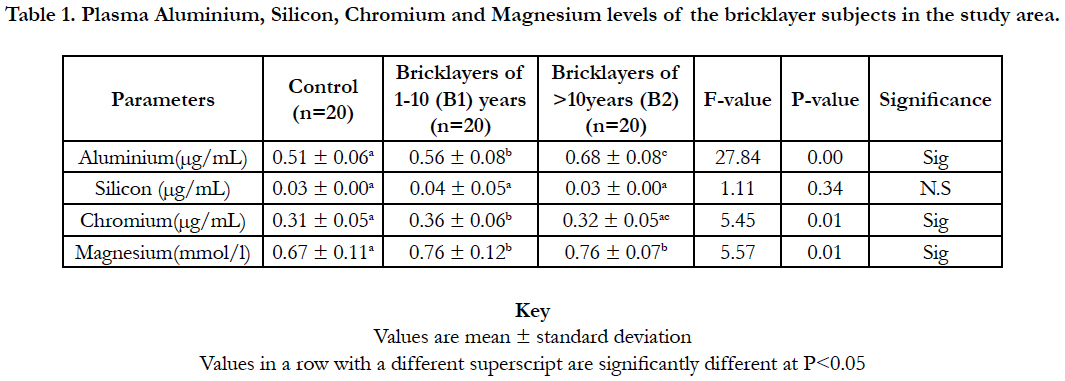

Table 1. Plasma Aluminium, Silicon, Chromium and Magnesium levels of the bricklayer subjects in the study area.
When the plasma silicon levels of the bricklayer subjects in the study area were compared with the plasma silicon levels of the control subjects, It was not statistically significant for bricklayers of 1-10 years (B1) and bricklayers of >10 years(B2) (f-value=1.11, p-value =0.34).
When the plasma Chromium levels of the bricklayer subjects in the study area were compared with the plasma chromium levels of the control subjects, It was significantly higher for bricklayers of 1-10 years (B1)(p=0.00) and not statistically significant for bricklayers of >10 years(p-value =0.57). Multiple comparisons showed that B1 was also significantly higher in comparison with B2 (p-value= 0.01).
When the plasma Magnesium levels of the bricklayer subjects in the study area were compared with the plasma Magnesium levels of the control subjects, It was significantly higher for bricklayers of 1-10 years (B1) and bricklayers of >10 years(f-value=5.57, p-value =0.01). Multiple comparisons showed that B1 was not statistically significant in comparison with B2 (p-value=0.84).
From Table 2, when the plasma Calcium levels of bricklayer subjects in the study area were compared with the plasma calcium levels of the control subjects, it was not statistically significant for bricklayers of 1-10 years (p-value=0.26). In comparison with the control the plasma calcium levels was significantly higher for bricklayers of >10 years (p-value =0.00). Multiple comparisons showed that B1 was also significantly lower in comparison with B2 (p-value= 0.00).
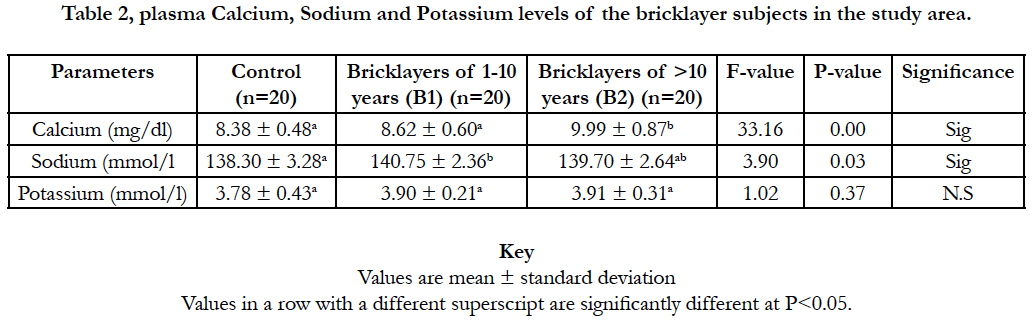
Table 2. Plasma Calcium, Sodium and Potassium levels of the bricklayer subjects in the study area.
When the plasma Sodium levels of the bricklayer subjects in the study area were compared with the plasma sodium levels of the control subjects, It was significantly higher for bricklayers of 1-10 years (B1) (p-value=0.01) and statistically not significant for bricklayers of >10 years(p-value =0.12). Multiple comparisons showed that B1 was also not statistically significant in comparison with B2 (p-value=0.24).
When the plasma Potassium levels of the bricklayer subjects in the study area were compared with the plasma Potassium levels of the control subjects, It was not statistically significant for bricklayers of 1-10 years (B1) and bricklayers of >10 years(B2) (f-value=1.02, p-value =0.37).
From table 3, When the plasma Total protein levels of the bricklayer subjects in the study area were compared with the plasma Total protein levels of the control subjects, It was not statistically significant for bricklayers of 1-10 years (B1) and bricklayers of >10 years(B2) (f-value=1.23, p-value =0.30).
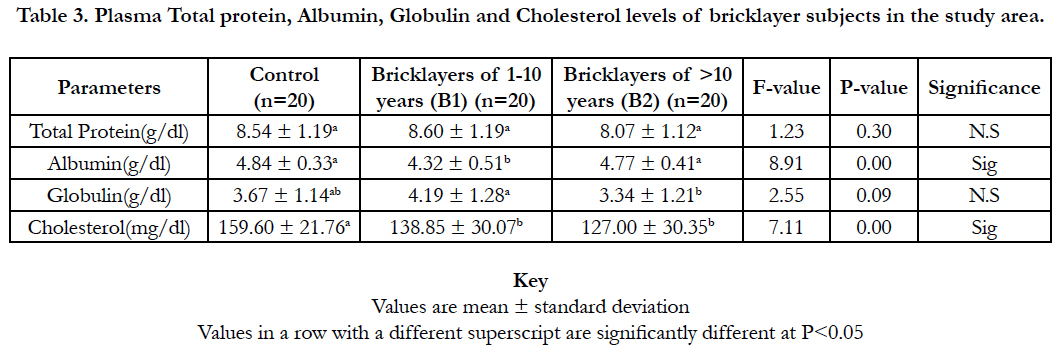
Table 3. Plasma Total protein, Albumin, Globulin and Cholesterol levels of bricklayer subjects in the study area.
When the plasma albumin levels of the bricklayer subjects in the study area were compared with the plasma albumin levels of the control subjects, it was significantly lower for bricklayers of 1-10 years (B1) and It was not statistically significant for bricklayers of >10 years(B2) (f-value=8.91, p-value =0.00). Multiple comparisons showed that B1 was also significantly lower in comparison with B2 (p-value=0.00).
When the plasma Globulin levels of the bricklayer subjects in the study area were compared with the plasma Globulin levels of the control subjects, It was not statistically significant for bricklayers of 1-10 years (B1) and bricklayers of >10 years(B2) (f-value=2.55, p-value =0.09). Multiple comparisons showed that B1 was significantly higher in comparison with B2 (p-value=0.03).
When the plasma Cholesterol levels of the bricklayer subjects in the study area were compared with the plasma cholesterol levels of the control subjects, It was significantly lower for bricklayers of 1-10 years (B1) and bricklayers of >10 years(f-value=7.11, pvalue =0.00). Multiple comparisons showed that B1 was not statistically significant in comparison with B2 (p-value=0.18).
Discussion
Production and usage of cement is a dusty process and the health of the workers has been studied. In this study, the plasma aluminum levels of the bricklayer subjects when compared with the plasma aluminum levels of the control subjects, was significantly higher for bricklayers of 1-10 years and also for bricklayers of >10 years. Multiple comparisons showed that plasma aluminium levels of bricklayers of 1-10 years were also significantly higher than bricklayers of >10 years. This shows that longer exposure to cement could result in increased plasma levels and possible increased exposure to diseases, as most of the bricklayers of >10 years were more involved in supervisory work than cement handling. In a study on the oxidative stress status among cement plant workers by Pournourmohammadi et al., [23], the results indicated a significant increase in Aluminium levels (p= 0.001) in direct-exposed workers in comparison to healthy control group. Further, a significant increase in Aluminium levels (p= 0.002) was observed in direct-exposed workers as compared to indirect-exposed one.
From the study, the plasma silicon levels of the bricklayer subjects in comparison with the control subjects was not statistically significant for bricklayers of 1-10 years and bricklayers of >10 years. This disagrees with the work done by Tajudeen, and Okpuzor [24] who monitored the variation in the degrees of exposure to elements in cement dust and health implications arising from working with cement or living within the vicinity of a cement company using fourty albino rats aged between four and five weeks old. From the study, atomic absorption spectroscopy of the lung tissues of the exposed rats showed significant levels of calcium, silicon, aluminum, chromium. Non significant plasma silicon levels may be attributed to the permeability of the pulmonary epithelium to silicon compounds with high molecular polar surfce area.
The plasma Chromium levels of the bricklayer subjects was significantly higher for bricklayers of 1-10 years and not statistically significant for bricklayers of >10 years. Multiple comparisons showed that bricklayers of 1-10 years was also significantly higher in comparison with bricklayers of >10 years. The study on the oxidative stress status among cement plant workers by Pournourmohammadi et al., [23], showed a significant increase in Chromium levels (P = 0.009) in direct-exposed workers in comparison to healthy control group. Further, a significant increase in Chromium levels (P = 0.009) was observed in direct-exposed workers as compared to indirect-exposed one. The lower levels of bricklayers of >10 years could be attributed to a reduction in the less aggressive work activity due to increasing age, although this postulate is subject to further research. Further correlation was found among serum level of Chromium and those of platelets, and chronic disease by Pournourmohammadi et al., [23].
The plasma Magnesium levels of the bricklayer subjects in the study was significantly higher for bricklayers of 1-10 years (B1) and bricklayers of >10 years). The plasma Calcium levels of bricklayer subjects in comparison with the plasma calcium levels of the control subjects was not statistically significant for bricklayers of 1-10 years. In comparison with the control, plasma calcium level was significantly higher for bricklayers of >10 years. Multiple comparisons also showed that bricklayers of 1-10 years was also significantly lower in comparison with bricklayers of >10 years. This finding agrees with the work done by Haitham [25], which showed that there was a significant increase in calcium level in the plasma of cement workers. This result also agrees with Fatima et al., [26] who found a significant increase in calcium level in the serum of workers exposed to cement dust of hydrated cement factory - India. The increase might be due to the fact that calcium compounds are the major components of cement [27].
This study showed that the plasma Sodium level of the bricklayer subjects was significantly higher for bricklayers of 1-10 years and was statistically not significant for bricklayers of >10 years. Multiple comparisons showed that plasma Sodium level of bricklayers of 1-10 years was also not statistically significant in comparison with bricklayers of >10 years. The plasma Potassium levels of the bricklayer subjects was not statistically significant both for bricklayers of 1-10 years and bricklayers of >10 years. This finding agrees with the research work done by Babalola and Babajide [28] at ceramic and cement industries at Ewekoro, Abeokuta North and South Local government areas of Ogun state, Nigeria.
From this study the plasma total protein levels of the bricklayer subjects in comparison with the plasma total protein levels of the control subjects was not statistically significant for bricklayers of 1-10 years (B1) and bricklayers of >10 years. The plasma albumin levels of the bricklayer subjects was significantly lower for bricklayers of 1-10 years and was not statistically significant for bricklayers of >10 years. Multiple comparisons showed that the plasma albumin levels of bricklayers of 1-10 years was also significantly lower in comparison with bricklayers of >10 years. The plasma Globulin levels of the bricklayer subjects was not statistically significant for bricklayers of 1-10 years and bricklayers of >10 years. Multiple comparisons showed that plasma Globulin levels of bricklayers of 1-10 years was significantly higher in comparison with bricklayers of >10 years, which may be due to the lower albumin levels of bricklayers of 1-10 years. Although no significant decline in Total protein as a whole was observed, plasma albumin levels of the bricklayer subjects was significantly lower for bricklayers of 1-10 years. In a study carried out by Khaled [29], in exposed workers of the cement factory of Libya, a decline in plasma total protein primarily due to a reduction in albumin fraction was due to exposure to cement. Oluwayernis [30] showed that the reduction in plasma protein in workers exposed to environmental pollutants (cement dust) could be attributed to changes in protein and free amino acid metabolism and their synthesis in the liver. Additionally, the protein depression in the blood was also reported to be mainly due to excessive loss through nephrosis. It may also be due to reduced protein synthesis or increased proteolytic activity or degradation [31]. From this study, the plasma Cholesterol levels of the bricklayer subjects in the study area when compared with the plasma cholesterol levels of the control subjects was significantly lower for bricklayers of 1-10 years (B1) and bricklayers of >10 years. This agrees with research work by Aydin et al., [32] whose findings indicate that cement workers are exposed to more oxidative stress as evidenced by increased concentration of lipid peroxidation(Lipid peroxidation is the oxidative degradation of lipids).
In a study done by Tajudeen and Okpuzor [24], Atomic absorption spectroscopy of the lung tissues of exposed rats showed significant levels of calcium, silicon, aluminum, chromium compared to the un-exposed rats (p<0.05). The histopathology study of the lung tissues of the exposed rats showed abnormal alveolar architecture, disrupted bronchus, damaged bronchioles, degenerated epithelium lining, weak respiratory connective tissues. Hence, the potential danger posed by continuous exposure to cement.
Conclusion
The objectives of this study which was; to determine the level of exposure of cement handlers to the heavy metals commonly present in cement by measuring the plasma concentration, to determine the level of lipid peroxidation by cement components by assessment of the total plasma cholesterol, to determine the health implication of prolonged exposure to cement was achieved, as the study revealed that some of the heavy metals and other elements present in the composition of cement such as Chromium, Aluminium, Calcium and Magnesium were detected in significantly higher amounts in the test subjects(Bricklayers) in comparison with the control. Lipid peroxidation may have also occurred as a result of the effect of the heavy metals and other components of cement, as significantly lower levels of total Cholesterol was observed in this study. In relation to previous studies, the presence of these elements in the plasma and continuous exposure to cement are a risk factor for various disease conditions, as demonstrated by Tajudeen and Okpuzor [24], using animal models.
References
- Ding M, Chen F, Shi X, Yucesoy B, Mossman B, Vallyathan V. Diseases caused by silica: mechanisms of injury and disease development. Int Immunopharmacol. 2002 Feb;2(2-3):173-82. PubMed PMID: 11811922.
- Meo S, Rasheed S, Khan M, Shujauddin S, Al-Tuwaijri A. Effect of cement dust exposure on phagocytic function of polymorphonuclear neutrophils in cement mill workers. Int J Occup Med Environ Health. 2008;21(2):133-9. PubMed PMID: 18715837.
- Ogunbilege JO, Akinosun OM, Akinduti PA, Nwaobi LA, Ejilude OA. Serum levels of some trace metals and leucocyte differential count in Nigeria cement factory workers; Possible toxicityimplications. Florida Int J. 2010;2:55-8.
- Fell AK, Thomassen TR, Kristensen P, Egeland T, Kongerud J. Respiratory symptoms and ventilatory function in workers exposed to Portland cement dust. J Occup Environ Med. 2003 Sep;45(9):1008-14. PubMed PMID: 14506344.
- Mohammadirad A, Abdollah M. A systematic review on oxidant/antioxidant imbalance in aluminium toxicity. Int J Pharmacol. 2011 Jan 1;7(1):12-21.
- Aminian O, Sharifian SA, Mehrdad R, Narooey HK, Giahi O. Humoral Immune system alterations in silica exposed workers. Iran J Public Health. 2008;37(3):142-5.
- Bhatty JI. Role of minor elements in cement manufacture and use.1995.
- ATSDR. Chromium toxicity physiologic effects. Agency for Toxic Substances and Disease Registry. CSEM. 2000.
- Kohen R, Nyska A. Oxidation of biological systems: oxidative stress phenomena, antioxidants, redox reactions, and methods of their quantification. 2002;30(6):620-50.
- Adly AA. Oxidative stress and disease: an updated review. Res J Immunol. 2010;3(2):129-45.
- Bánfalvi G. Heavy metals, trace elements and their cellular effects. InCellular effects of heavy metals. Springer Netherlands; 2011. p.3-28.
- Baldwin DR, Marshall WJ. Heavy metal poisoning and its laboratory investigation. Ann Clin Biochem. 1999 May;36 ( Pt 3):267-300. PubMed PMID: 10376071.
- World Health Organization. Guidelines for drinking-water quality: recommendations. World Health Organization; 2004.
- Roper WL, Houk VN, Falk H, Binder S. Preventing lead poisoning in young children: A statement by the Centers for Disease Control, October 1991. Centers for Disease Control, Atlanta, GA (United States); 1991 Oct 1.
- Akinola MO, Okwok NA, Yahaya T. The effects of cement dust on albino rats (Rattus norvegicus) around West African portland cement factory in Sagamu, Ogun state, Nigeria. Res J Environ Toxicol. 2008;2:1-8.
- Post Offices- with map of LGA. NIPOST. 2009 Oct 20. Retraction in: NIPOST. 2009 Oct 20.
- Walsh A. The application of atomic absorption spectra to chemical analysis. Spectrochimica Acta. 1955 Jan 1;7:108-17.
- Gitelman H. Clinical Chemistry-Calcium-O-Cresolpthalein complexone method. Anal Biochem. 1967;20:521.
- Csoregi E, Quinn CP, Schinidtke DN. Design, Characterization and calibration of ion selective electrode. Anal Chem. 1994.
- Piotrowski G. A new reaction to albuminous bodies and their near descendants: (Mitthlg adkk physiol. Inst. Krakow.) (From April 1857 d. Sitzgsber dm-nat. Cl. Of the k. Ak. D. Wiss XXIV., P. 335). 1857.
- Bishop M, Fody EP, Schoeff LE. Clinical chemistry–principles, procedures, correlation. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins Quality assurance; 2000.
- Allain CC, Poon LS, Chan CS, Richmond WF, Fu PC. Enzymatic determination of total serum cholesterol. Clin Chem. 1974 Apr;20(4):470-5. PubMed PMID: 4818200.
- Pournourmohammadi S, Khazaeli P, Eslamizad S, Tajvar A, Mohammadirad A, Abdollahi M. Study on the oxidative stress status among cement plant workers. Hum Exp Toxicol. 2008 Jun;27(6):463-9. PubMed PMID: 18784198.
- Tajudeen Y, Okpuzor J. Variation in exposure to cement dust in relation to distance from Cement Company. RJET. 2011 May 1;5(3):203.
- Al-Hayali HL. Effect of Cement Pollution on some Biochemical Parameters in the Blood Serum of Hamam AL-Alil Cement Factory Workers. J. Raf. Sci. 2009;20(2):19-28.
- Fatima SK, Ramana Devi V, Aruna PP, Reddy PP. Blood serum protein and calcium levels in portland cement factory workers. Indian J Environ. Toxicol. 1997;7(2):56-7.
- Mwaiselage J, Bråtveit M, Moen B, Yost M. Variability in dust exposure in a cement factory in Tanzania. Ann Occup Hyg. 2005 Aug;49(6):511-9. PubMed PMID: 15845607.
- Babalola OO, Babajide SO. Selected heavy metals and electrolyte levels in blood of workers and residents of industrial communities. Afr J Biochem. Res. 2009 Mar 31;3(3):37.
- Al Salhen KS. Assessment of oxidative stress, haematological, kidney and liver function parameters of Libyan cement factory workers. Am J Sci. 2014;10(5):58-65.
- Oluwayernis B. Antioxidant status and hepatic lipid peroxidation in albino rats exposed to cement Dust. Trans J Sci Tec. 2012;2:50-9.
- Rana SV, Singh R, Verma S. Protective effects of few antioxidants on liver function in rats treated with cadmium and mercury. Indian J Exp Biol. 1996 Feb;34(2):177-9. PubMed PMID: 8641719.
- Aydin S, Aral I, Kilic N, Bakan I, Aydin S, Erman F. The level of antioxidant enzymes, plasma vitamins C and E in cement plant workers. Clin Chim Acta. 2004 Mar;341(1-2):193-8. PubMed PMID: 14967176.





