Development of an In-House Enzyme-Linked Immunosorbent Assay Based on Helicobacter Pylori Sonicate Whole Cell Antigen for Diagnosis of Gastroduodenal Ulcer Disease in Karachi, Pakistan
Faisal Aziz1*, Yasmeen Taj 2, Shahana Urooj. Kazmi 1
1* Immunology and Infectious Diseases Research Laboratory, Department of Microbiology, University of Karachi, Karachi, Pakistan.
2 Department of Pathology, Dow Medical University, Dow University of Health Sciences, Karachi, Pakistan
*Corresponding Author
Faisal Aziz,
Immunology and Infectious Diseases Research Laboratory,
Department of Microbiology, University of Karachi,
Karachi, Pakistan.
Tel: 86-13019487160,86-13390064250
E-mail: faisalaziz.micro@yahoo.com
Article Type: Research Article
Received: September 04, 2013; Accepted: October 18, 2013; Published: October 21, 2013
Citation: Aziz F , Taj Y , Kazmi SU (2013) Development of an In-House Enzyme-Linked Immunosorbent Assay Based on Helicobacter Pylori Sonicate Whole Cell Antigen for Diagnosis of Gastroduodenal Ulcer Disease in Karachi, Pakistan. Int J Microbiol Adv Immunol. 1(4), 24-31. doi: dx.doi.org/10.19070/2329-9967-130005.
Copyright: Faisal Aziz © 2013. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Helicobacter pylori (H. pylori) is a causative agent of gastritis, gastroduodenal ulcers and gastric adenocarcinoma. Improper diagnostic facilities are responsible for the increasing incidence of H. pylori infections in Pakistan. ELISA is a noninvasive, less expensive assay for diagnosis of H. pylori . ELISA performance is mainly based on the H. pylori strain and nature of antigen. In this study, a total of 214 gastritis and ulcer patient’s serum samples were screened for anti- H. pylori IgG antibody. A 96-well plate coated with 10 μg/ml sonicate antigen and hundred-fold diluted patient’s serum was allowed to react. After extensive washing with buffer, 1:2,000 diluted conjugated secondary antibody was added. Later substrate was added to observe positivity by measuring the intensity of color. Statistical analyses were performed, and p value of < 0.01 was taken as significant; 84 % male patients and 96 % female patients, respectively, tested positive for H. pylori , while agewise distribution was 35–45 years males (40 %) and 35–45 years females (73 %) were found highest number of H. pylori infected patients. In-house ELISA based on sonicate whole cell antigen (sELISA) showed a sensitivity of 98 %, specificity of 100 %, accuracy 98 % and κ value 0.906 with significant correlation R—0.956; p < 0.0001. We conclude that ELISA for H. pylori sero-diagnostic infection should be based on the local strain for better sensitivity and specificity. sELISA is better and reliable diagnostic assay for the diagnosis of H. pylori infection in gastric patients of Karachi, Pakistan.
2.Introduction
3.Materials and Methods
i.Patients And Gastroendoscopy
ii.Preparation of H. pylori sonicate whole cell antigen
iii.Rabbit immunization with H. pylori antigen
iv.Requirement for acceptance of ELISA plates
v.Development of in-house ELISA for H. pylori sonicate whole cell antigen (sELISA)
vi.H. pylori titer optimization and application
vii.Quality control test of sELISA
viii.Application of sELISA
ix.Cutoff value estimation
x.Evaluation of sELISA
xi.Characterization of H. pylori sonicate whole cell protein by SDS-PAGE
xii.Ethical clearance
4.Results
i.Requirement for acceptance of ELISA plates
ii.Rabbit anti- H. pylori serum valuation
iii.Developed sELISA parameters
iv.sELISA cutoff estimatation
v.Quality control test of sELISA
vi.Analysis of H. pylori titer by sELISA
vii.Age- and sex wise distribution of gastric patients by sELISA
viii.sELISA comparison with serological assay
ix.Evaluation of sELISA
x.Characterization of H. pylori sonicate whole cell protein
5.Discussion
6.Disclosure
7.References
Keywords
Diagnosis; Helicobacter pylori ; Sonicate whole cell antigen; In-house Enzyme-linked immunoassay; Gastroduodenal ulcer disease.
Introduction
H. pylori is a gram-negative, spiral shaped, flagellated microaerophillic bacterium which colonizes 50 % of the humans’ stomach [1]. It is the major cause of active chronic gastritis and is strongly associated with gastritis, duodenal ulceration and carcinogenesis [2]. Several risk factors play an important role in H. pylori infection such as, gender, age, crowding and low socioeconomic status [3]. About 20–50 % of the adults in the developed countries and nearly 80–90 % in the developing countries were seropositive against H. pylori [4, 5]. In developing countries, infection is acquired early in life such as less than 5 years children (20 %) and at the age of 20 years (80 %), while the developed countries have high infection rate at the age of 60 years (50 %) [3].
H. pylori colonizes to human stomach lead to the activation of humoral and cell mediated immune response [6] which at circulating level predominantly stimulates immune responses of IgG class [2]. H. pylori have elevated titers of serum immunoglobulin because of elicits both local and systemic immune response [7]. The natures of antigen play a significant role in the improvement of ELISA sensitivity and specificity [8]. H. pylori have a diverse protein profile with different antigenic candidates which can use as putative components of vaccines such as, surface whole cell, sonicate and flagellar antigens [9-11]. H. pylori sonicate antigen activitate strong IgG immune response and significantly reduce the gastric bacterial load [12]. Whole cell sonicates antigen cover a broad range of antigens which were found to be more immunogenic [13].
H. pylori is diagnosed by different invasive test such as, microbiological culture, histological examination, and rapid urease tests, while nowadays H. pylori is diagnosed through a noninvasive test such as, PCR, urea breath test and Enzyme immunoassays. ELISA is simple, economical assay and has a less burden for the patient; these qualities make ELISA more attractive as compared to other non-invasive test [14]. It is better and reliable assay for the detection of H. pylori serum antibodies to evaluate prevalence in large communities [3]. A majority of serological studies are now conducted with commercial ELISA kits that have been optimized and evaluated in developed countries [13]. Commercial ELISA kits are too expensive for developing countries along with restricted ELISA sensitivity and specificity by using specific geographical related antigen [15-17]. H. pylori strains from Asian countries have different antigenic properties as compared to western countries [18]. In-house ELISA based on the H. pylori local strain can give better and reliable results as compared to commercial ELISA [15, 16]. We develop an in-house ELISA based on H. pylori sonicate whole cell antigen by using H. pylori local isolates for the diagnosis of H. pylori infection in Karachi, Pakistan.
Materials and Methods
All gastric patients were undergone through gastroendoscopy and examination in the Civil Hospital Karachi, Pakistan. Tissue biopsies were obtained from the antral and corpus part of the stomach during gastrointestinal endoscopy along with 214 blood samples from consenting patients. Gastric patient’s blood samples were characterized as chronic gastritis and gastric ulcer. All the samples were transported to Immunology & Infectious Diseases Research Laboratory (IIDRL) for further processes and frozen at -20 °C until tested. All gastric samples and the research protocols were in accordance with the Karachi University’s Ethical Committee.
Tissue biopsies were processed and cultured on Colombia agar (CA) plates containing 7 % lysed horse blood and antibiotics (amphotericin B, trimethoprim, cefsulodin and vancomycin). The CA plates were incubated for 4–5 days under microaerophillic conditions at 37 ºC and identification was carried out by different conventional and molecular methods. Several H. pylori strains were inoculated in the BHI broth, incubated at 37 ºC for 5 days in microaerophillic environment. H. pylori heavy growth was centrifuged at 10,000 rpm for 10 min, followed by 3 times washing with 20 mM Tris HCl buffer (pH 7.5) and suspended in the same buffer. Cells were sonicated on ice with 6 times for 30 s with a 60 s interval between each shock. The sonicated samples were centrifuged at 5000 rpm for 10 min to remove the cell debris. Then supernatant treated with 0.5 % formalized saline and makes the aliquots and kept frozen at -20 °C. Protein concentration was measured by Coomassie blue assay (Bio-Rad, USA), bovine serum albumin used as a standard.
Adult female rabbits were immunized intravenously with the increasing amount of antigen (3 × 108cells/ml) on the days of 1, 3, 5, 7 and 17. Blood was collected from a marginal ear vein and by cardiac puncture after the slide agglutination test. Pre-immunization sera were used as a negative control to standardization the ELISA based on sonicate whole cell antigen (sELISA).
The ELISA plate was examined by different negative and positive serum samples. All reference serum samples were obtained from IIDRL, Department of Microbiology. Serum from rabbit, sheep, and healthy human were used as a negative reference while gastritis patient serum was used as a positive control after confirmation by commercial ELISA Kit (Equipar, Italy). Different components of sELISA such as H. pylori antigens, PBS, blocking agent, enzyme conjugate and substrate were also used separately as negative control. The acceptance level of ELISA plate was OD >0.5 and < 0.20 for positive and negative control, respectively. ELISA value was calculated as (EV = OD of Test sample/OD of calibration unit) by taking 5 Uarb/ ml (OD450nm = 0.723) as a calibration unit (5 Uarb/ ml used to discriminate between negative and positive population). Data were present as mean ± SEM.
In order to develop sELISA, each component was separately optimized including antigen concentrations, enzyme conjugates, test serum and incubation times. Details of the sELISA standardization and development were indicated in the “Result” section.
In order to optimize primary antibody titer, we were tested anti-H. pylori sera between the range of 10-1 and 10-15 at constant antigen concentration (10μg/ml). Titer range was determined relative to the negative values which were greater than cutoff values. This optimized range was applied on a gastric patient serum to analyze the H. pylori titer status.
In order to check the comparable results of serological assay, it is necessary to execute the quality controls of the developed ELISA. Repeatability was determined by comparing coefficients of variation (CV) of strong positive (highest OD value) and weakest negative (lowest OD value) serum samples of the plate. Coefficient variation of each well was calculated by using the coefficient of variation of the plate as,
Developed sELISA was applied to gastric patient’s serum as; a 96-well plate (Sero-Wel, UK) were coated with 10 μg/ml (100 μl) of H. pylori sonicate whole cell antigen in coating buffer (Na2CO3, NaHCO3, pH 9.6) with overnight incubation at 4 ºC. Next day, it was washed five times with PBS-Tween 20 (0.05 %) (pH 7.2) and blocked free active sites by 3 % BSA. After washing, 100 μl (1:100 diluted) of patient serum was added into consecutive wells along with negative and positive controls and incubated at 37 ºC for 1 h. After extensive washing, HRP-conjugated goat anti-human IgG antibody (1:2,000) was added and incubated for 1 h at 37 ºC. Later, 100 μl of substrates (TMB One solution G7431, Promega, USA) was added and kept for 30 min at room temperature in dark place. The reaction was stopped by adding 0.3 M H2SO4 and color intensity was measured at 450 nm by an ELISA reader (STAT FAX-2100).
Receiver operating characteristic (ROC) curves [plots of sensitivity against (1-specificity)] were plotted to estimate the optimal cutoff value of different values of sensitivity (Se) and specificity (Sp). Area under the ROC curve (AUC) was estimated by two-tailed test with an accuracy value of 0.5 as significance level [19]. The perfect diagnostic test would appear as close as possible to the upper left-hand corner, where both sensitivity and specificity are 100 %. We select a cutoff value of higher sensitivity with minimum false-negative value and high specificity with minimum false-positive [20]. We also measure by the mean optical density of the known negative samples plus two or three times the standard deviation.
The sELISA was evaluated with previously reported commercial ELISA assay (kELISA) and in-house ELISA based on H. pylori surface whole cell antigen (wELISA) [21] by the κ statistic. Student’s t test (one sample and independent samples) was used to compare mean value. Linearity of correlation was calculated by the Pearson’s coefficient correlation method. p < 0.01 were considered as significant. The statistical software, namely SPSS 16.0, MedCalc 11.3.3 and Graph Pad Prism 5.03, was used for analyzing the data.
Tris-HCl buffer SDS-PAGE (Laemmli) was applied to separate the sonicate whole-cell antigen and serum at 10–8 % with 5 % stacking gel by using Bio-Rad Minigel apparatus. Coomassie staining was performed with Coomassie brilliant blue solution [Coomassie brilliant blue (CBB)-R250]. Relative molecular weight (Mr) of unknown protein was determined to calculate their Rf values by using a standard protein marker (Bio-Rad: 161-0318) with linear regression curve method (excel spreadsheet program) [22].
This study was approved by the Karachi University’s Ethical Committee in Karachi, Pakistan.
Results
This study was designed to develop an in-house ELISA for the diagnosis of H. pylori infection in gastritis and gastroduodenal ulcer patients of Karachi, Pakistan. A total of 214 blood samples were collected from patients reporting at Civil Hospital Karachi with the symptoms of gastritis and gastroduodenal problems. Blood collected from male or female patients (35 % and 65 % respectively) was processed in IIDRL (Immunology & Infectious Diseases Research Laboratory), Department of Microbiology, Karachi.
The reference negative and positive control values were found to be in the range of assay limit. Negative controls showed the mean OD values between the range of 0.079 ± 0.052 to 0.1525 ± 0.031, EV = 0.109–0.210, and positive controls showed values in the range of 1.045 ± 0.029 to 1.316 ± 0.055, EV=1.445–1.565. This result showed the correct validity of the controls with an acceptable level of ELISA value.
Different parameters were optimized to develop sELISA. We found 1.167 ± 0.046, EV = 1.614 of anti-H.pylori sera against H. pylori sonicate whole cell antigen, which was seventeen times more than the pre-bleed rabbit serum 0.0675 ± 0.004, EV = 0.093 and was considered as positive. The slide agglutination test was also shown significant agglutinates; hence, the batches of rabbit anti-H. pylori sera were used for the development of sELISA.
The optimized condition for sELISA was performed as we tested H. pylori antigen concentrations by checkerboard method from 5 mg/ml to 5.96 × 10-7 which was followed by selecting five optimal antigen concentrations of 40, 30, 20, 10 and 4 μg/ml (Fig. 1a). The optimal antigen concentration for sELISA was chosen as 10 μg/ml concentration with 1:10-2 working serum dilution (Fig. 1b). The primary antibody titer range was found to be optimum between 10-1 and 10-11of diluted serum at which the serum gives a positive result (Fig. 1c). An enzyme conjugate dilution of 1:2,000 was arbitrarily chosen and was subsequently used for detection of anti-H. pylori antibody (Fig. 1d).
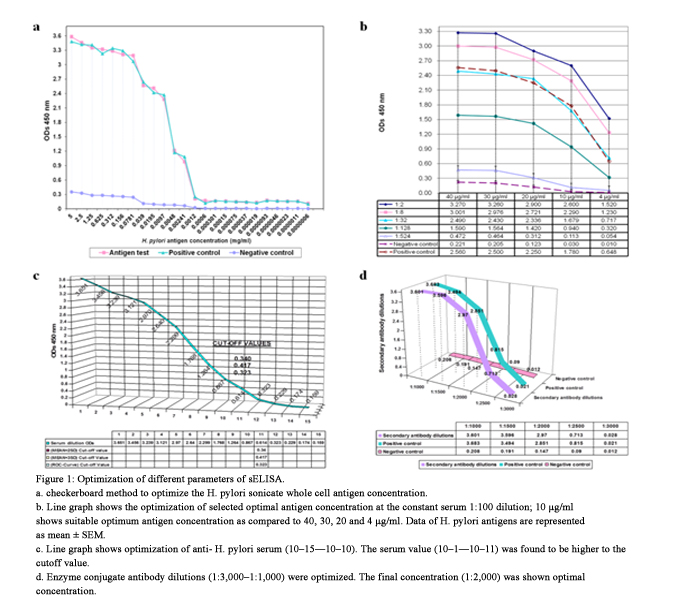
Figure 1: Optimization of different parameters of sELISA.
a. checkerboard method to optimize the H. pylori sonicate whole cell antigen concentration.
b. Line graph shows the optimization of selected optimal antigen concentration at the constant serum 1:100 dilution; 10 μg/ml shows suitable optimum antigen concentration as compared to 40, 30, 20 and 4 μg/ml. Data of H. pylori antigens are represented as mean ± SEM.
c. Line graph shows optimization of anti- H. pylori serum (10–15—10–10). The serum value (10–1—10–11) was found to be higher to the cutoff value.
d. Enzyme conjugate antibody dilutions (1:3,000–1:1,000) were optimized. The final concentration (1:2,000) was shown optimal concentration.
The diagnostic performance of a test was evaluated to discriminate between normal and diseases cases by using ROC curve analysis [23, 24]. In order to confirm the disease, we selected a cutoff value of 0.340 which has a higher sensitivity with negative predictive value and high specificity with a positive predictive value [20]. The cutoff values by mean ± 2SD and mean ± 3SD was found to be as 0.344 and 0.356, respectively. The ROC plot closer to the upper left corner indicated the perfect separation and no overlapping of the ODs of gastroduodenal ulcer patients with highest overall accuracy of the ELISA test [24]. The area under the ROC curve equals to 1 with a 95 % confidence interval (CI) from 1.00 to 1.00 (Fig. 2a). Scatter plot showed an optimum cutoff value of 0.340 (34.0 %) with highest sensitivity and specificity of 100 % (95 % CI 97.6–100) and 100 % (95 % CI 70.6–99.7), respectively (Fig.2b).
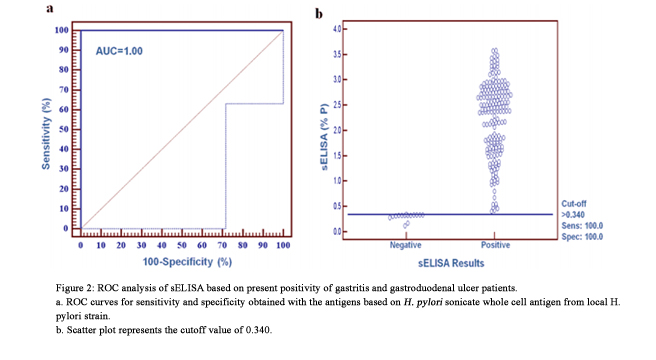

Figure 2: ROC analysis of sELISA based on present positivity of gastritis and gastroduodenal ulcer patients.
a. ROC curves for sensitivity and specificity obtained with the antigens based on H. pylori sonicate whole cell antigen from local H.pylori strain.
b. Scatter plot represents the cutoff value of 0.340.
In order to assess the real variability of sELISA, we run the quality control test and determine the variation between the intra- and inter-assay. The coefficient of variation of plate was found to be 13.16 % (in acceptance limit), indicated that each well of the plate was coated with equal antigen concentrations. Since the surety of the good quality and stable state of the antigen, it is necessary to run quality control test in the development of ELISA.
We found 48 % of patients have 1:10-11 anti-H. pylori titer, while 5 % showed 1:10-1 titer value. This result showed the inconsistency of H. pylori titer (1:10-11–1:10-1) in gastric patients (Fig. 3). There was significant difference between the mean values of each dilution (Table 1). In previous study we found a significant effect of H. pylori antigenic variation on H. pylori antibody titer between H. pylori sonicate and surface whole cell antigen. H. pylori sonicate whole cell antigen have significant variation effect on H. pylori antibody titer with H. pylori surface whole cell antigen [21].
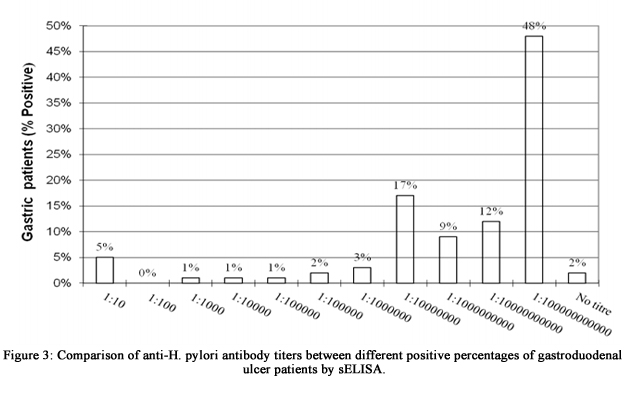
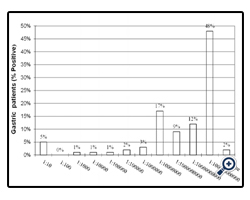
Figure 3: Comparison of anti-H. pylori antibody titers between different positive percentages of gastroduodenal ulcer patients by sELISA.
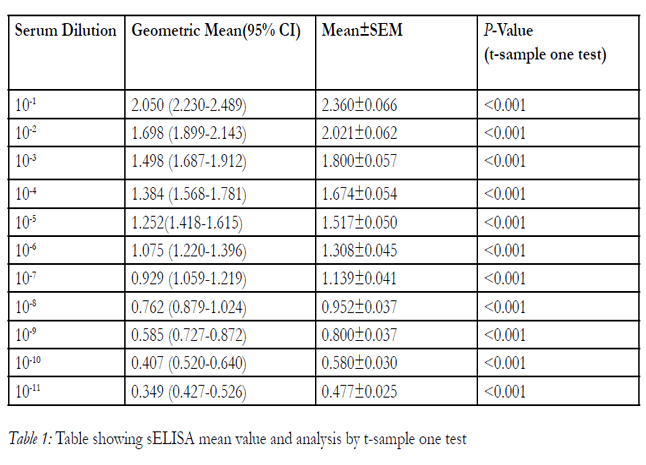

Table 1: Table showing sELISA mean value and analysis by t-sample one test
In this study, 214 patients were enrolled between the age of 15 and 75 years (65 % of females and 35 % of males); 92 % of the patients were found to be H.pylori positive while, sexwise distribution found as female (96 %) and male (84 %) by sELISA. We observed a high risk of H. pylori seropositive in middle-aged patients as compared to the old ages. High risk of infection was found in female between the ages of 35 and 45 years (73 %) as compared to ages of 15-25 years (55 %) have low risk of infections. Male patients (35–45 years) were showed high risk of infection (40 %) while an apparent decrease in the risk of infection were found at the ages of 65–75 (13 %).
Enzyme-linked immunosorbent assay based on sonicate whole cell antigen was evaluated by comparing with kELISA. sELISA showed high significant correlation between kELISA R— 0.9562 (95 % CI from 0.9430 to 0.9664), (p < 0.0001) as compared to previously reported data of wELISA [21].
In order to evaluate the authenticity of sELISA, we compare it with kELISA and wELISA. We found a more strong association of sELISA with kELISA (κvalue=0.906) as compared to previously reported wELISA [21]. A cutoff value of 0.344, 0.356 and 0.340 were recommended as the optimal cutoff value in order to maximize the accuracy and minimize false negativity. On the basis of the accuracy, we can say that the diagnostic value of sELISA were to be excellent (90–100 % = excellent test) (Table 2).
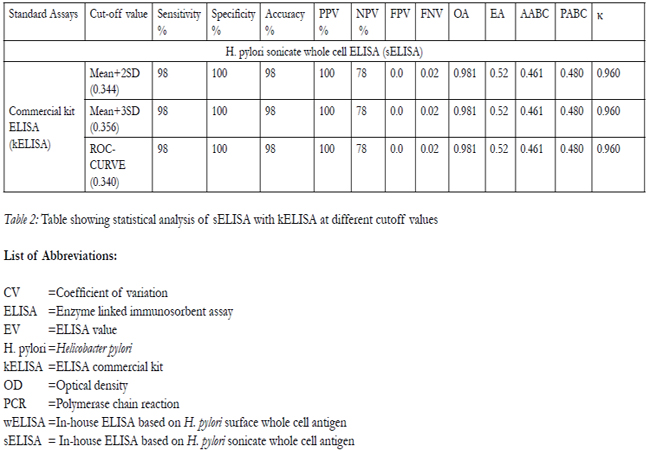
Table 2: Table showing statistical analysis of sELISA with kELISA at different cutoff values
List of Abbreviations:
CV =Coefficient of variation
ELISA =Enzyme linked immunosorbent assay
EV =ELISA value
H. pylori = Helicobacter pylori
kELISA =ELISA commercial kit
OD =Optical density
PCR =Polymerase chain reaction
wELISA =In-house ELISA based on H. pylori surface whole cell antigen
sELISA = In-house ELISA based on H. pylori sonicate whole cell antigen
Helicobacter pylori protein characterization showed quantitative and qualitative different H. pylori sonicate protein. Tris-HCl buffer resolves the H. pylori sonicate whole cell antigen into nine numbers of proteins with the protein size of 10 and 68 kDa (68, 59, 45, 32, 29, 24, 21, 17and 10 kDa), while their respective rabbit serum showed protein bands between the size of 7 and 55 kDa (55, 51, 40, 38, 36, 32, 30, 29, 24, 22, 21, 18, 17,14, 12, 10, 9 and 7 kDa) (Fig. 4).
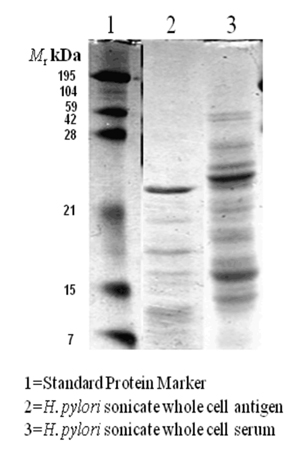

Figure 4: Sodium dodecyl sulfate–polyacrylamide gel electrophoresis analysis of H. pylori sonicate whole cell antigen (lane 2) (separated by 10 %) and their respected serum (lane 3) (separated by 8 %).
Discussion
Helicobacter pylori is a noninvasive bacterium which stimulates the immune response by releasing different immunogenic proteins and lipopolysaccharides. There are many serological assays for H. pylori detection which differs on the basis of their sensitivity [10, 25, 26]. ELISA is well formulated and standardized assay for the detection of the H. pylori antibodies [8]. The performance of ELISA is mainly based on the nature of antigen and H. pylori strain [27]. ELISA based on H. pylori local strains antigen have higher performance as compared to foreign strains [17]. H. pylori have different type of antigens such as formaldehyde- or heat-treated whole bacteria, sonic extract, acid glycine extract. Whole cell lysate is the best choice of antigen as compared to a purified antigen which unable to recognize various type of antibodies present in the population [28]. H. pylori whole-cell sonicates is an effective human vaccine which stimulate high immune response against H. pylori [29]. ELISA based on local H. pylori sonicated antigen is useful assay which give real status of H. pylori titre [17]. Acording to Megraud et al., ELISA based on H. pylori sonicate antigen have high sensitivity and specificity [30]. We developed an in-house ELISA from the local strain of H. pylori to investigate the H. pylori seroprevalence in the population of Karachi, Pakistan.
The quality of ELISA is varies and is largely depend upon the level of optimization. The reagents of ELISA were optimized according to the application and the assay format which can only be verified by trial and error method. In sELISA development, low antigen concentrations (1.218 × 10-3–5.96 × 10-7 mg/ml) were showing very low titer because of the unavailability of enough antigens to capture the antibody. However, high antigen concentrations (5–0.07 mg/ml) were shown very high titer and could produced signals even in the negative serum control indicated the presence of an adequate amount of antigen and availability of nonspecific antibody in the systems which results in nonspecific binding reaction (Fig. 1a). From five selected optimal concentrations, 40 and 30, 20 μg/ml of antigen concentration showed a high titer, even in negative control. The antigen concentration of 4 μg/ml gave the lowest titer which revealed that assay have very low specificity and sensitivity, while 10 μg/ml of antigen showed optimum titer even in the negative control which mean antigen was present in optimum concentration to capture the antibody with negligible nonspecific binding; 4 μg/ml of antigen concentration gave the negligible difference of optical density between the test sample and negative control, showed that there was no binding occur because of not enough antigen present in reaction to the capture antibody (Fig. 1b). The test serum working dilution of 1:10-3 showed low absorbance as compared to 1:10-2 serum dilution because of the too diluted concentration. The primary antibody titer was optimized by making serial dilution up to 10-15. The 10-12 diluted serums showed low absorbance value as compared to 10-11 diluted serum which showed a high absorbance to cutoff value.The 10-1–10-11 diluted serum range was found to be optimum at which the serum gives a positive result (Fig. 1c); 1:1,000 and 1:1,500 dilutions of conjugate were shown very high detection level as compared to the positive control, while 1:2,500 and 1:3,000 gave very low detection value almost near to the value of negative control. The enzyme conjugate dilution of 1:2,000 showed optimal antibody detection level (Fig. 1d). The higher conjugate concentration increased the nonspecific reading; while lower conjugate levels decreased the specific absorbance measurement but the nonspecific binding was remain unchanged. The cutoff values were validated from the pool of reference sera of H. pylori local isolates, which was helpful to constant the specificity because of the diverse H. pylori antibody profile [9]. Blecker et al. used the cutoff value derived from ROC curve analysis [28]. The low CV 13.16 % of sELISA indicated its repeatability was in agreement with international recommendation for CV of OD values of replicating samples [31].
ELISA based on sonicate whole cell antigen were developed to determine the presence of H. pylori infection with a high degree of specificity and sensitivity. sELISA was evaluated by comparing with other immunoassay such as in-house ELISA based on surface whole cell antigen (wELISA) and commercial kit ELISA (kELISA). We found high sensitivity (98 %), specificity (100 %) and accuracy (98 %) of sELISA in comparison with kELISA as compared to previously reported wELISA [21]. Our results showed comparable values with those from other published papers; for example, Krajaejun et al. reported the 100 % sensitivity with 95.07 % specificity of in-house ELISA [32]. Ghasemian et al. found sensitivity of 90 % with 88 % specificity [33]. There is a disparity between western countries ELISA (sensitivity 93 % and specificity 94 %) and Asian countries ELISA (50 % and specificity 72%). These disparities are caused by the H. pylori strain heterogeneity from different parts of the world [16]. The close perfect association of sELISA was found between kELISA (κ value = 0.960) in contrast to wELISA [21]. sELISA showed high significant correlation with kELISA (R—0.956) (p < 0.0001) as compared to wELISA [21]. Serum sample tested for anti-H. pylori antibodies using sonicated H. pylori antigen showed that sonicated antigen is better antigen in developing sensitive and specific ELISA. So ELISA developed by sonicated antigen is most specific and reliable tests for the serological diagnosis of H. pylori infection.
In the development of ELISA for antibody screening,it is important to determine the antibody titres. In our study, we found high percentage of patients (48 %) showed high H. pylori antibody titre (1:10-11), 17 % showed titre of 1:10-8 while 5 % showed very low titre of 1:10-1. The prevalence rate of H. pylori was found to be high in females (96 %) as compared to male (84 %) by sELISA. Previous results from our laboratory showed high H. pylori prevalence rates in male (59.36%) as compared to female (53.95 %) [10]. The agewise prevalence rate of H. pylori infection was highest among the age group of 35–45 (40 %) as compared to ages 15–25 (36 %). Female population showed high risk of infection between the ages of 35 and 45 (73 %). Male patients (35–45 years) were showed high risk of infection (40 %) while an apparent decrease in the risk of infection were found at the ages of 65–75 (13 %). Similar high prevalence rate of age group 35–45 was previously reported by our laboratory and the other researcher of the world [34, 35]. Our results showed a comparable prevalence with those from other [36, 37] parts of the world including Brazil, Korea, Japan, Canada and Turkey between the range of 31 and 78 %. This H. pylori incidence rate indicates a quite wide range from different parts of the world. In developed countries, 40 % of the adults are colonized by H. pylori as compared to children [38]. In France, less than 1 % of children were infected (>6 years), 5 % (6–12 years) and 15 % (15–18 years) as compared to developing countries such as Thailand which have 18 % (5–9 years), 15 % (15–18 years) and 55 % (30 years), while Vietnam have about 40 % of the infection rate in the teenagers [38, 30].
Proteomics used to identify the vaccine candidate and other important protein of H. pylori to further increase the sensitivity of test; we have to identify the epitope of antigen against which the antibody raised. We found low molecular weight protein of H. pylori sonicate whole cell antigen between 10 and 68 kDa (68, 59, 45, 32, 29, 24, 21, 17and 10 kDa), while their respected serum (anti-H. pylori serum) showed the proteins between 7 and 55 kDa (55, 51, 40, 38, 36, 32, 30, 29, 24, 22, 21, 18, 17, 14, 12, 10, 9 and 7 kDa) (Fig. 4). H. pylori low molecular weight antigen appears to be more reliable for the detection of H. pylori infection in children and adults [39]. Kimmel et al. reported different immunodominant antigens of H. pylori such as 44 kDa (translation elongation factor EF-Tu), 38 kDa (DNA-directed RNA polymerase), 28 kDa (conserved hypothetical protein), 25 kDa (3-oxoadipate coenzyme A transferase subunit A), 22 kDa (alkyl hydroperoxide reductase), 20 kDa (peptidoglycan-associated lipoprotein precursor (Omp18)), 17 kDa (biotin carboxyl carrier protein) and 14 kDa (ribosomal protein L7/ L12) which nearest to our H. pylori sonicate whole cell antigen relative molecular weight [40].According to Andersen et al., H. pylori low molecular antigen protein has dominative role in H. pylori infection [39]. Haque et al. reported the immunogenic proteins with molecular weight of 61, 58 and 24 kDa from H. pylori whole cell extract [41]. A diversified high number of H. pylori proteins reflects the host response to H.pylori infection and indicates the importance of using a multicomponent antigen for detection of H. pylori antibodies. The crude antigen contains a large number of different proteins which may play a major antigenic role. sELISA is a multicomponent antigen assay which can used to detect H. pylori antibodies in the gastritis and gastroduodenal ulcer patients.
We conclude that in-house ELISA based on H. pylori sonicate whole cell antigen is better and reliable diagnostic assay for H. pylori diagnosis, as the various parameters were adjusted according to their native environment and conditions. ELISA for serodiagnosis of H. pylori infection should be based on local strains for optimal sensitivity and specificity. In-house sELISA can provide a reliable and a clinically useful method for the diagnosis of H. pylori infection in gastric patients of Karachi, Pakistan.
Disclosure
We have no financial relationships or interests to disclosure.
References
- Borghese A, Mazzi M. Buffalo population and strategies in the world. FAO REU Technical series 67, FAO Rome. 2005;Buffalo Production and Research:1-40.
- Singh CV, Barwal RS. Buffalo breeding research and improvement strategies in India. 9th World buffalo Congress, Argentina. 2010:1024-31.
- Tripaldi C. Buffalo milk quality. FAO REU Technical series 67, FAO Rome. 2005;Buffalo Production and Research:173-84.
- Borghese A. Buffalo cheese and milk industry. . FAO REU Technical series 67, FAO Rome. 2005;Buffalo Production and Re search:185-96.
- Fagiolo A, Roncoroni C, lai O, Borghese A. Buffalo Pathologies.FAO REU Technical series 67, FAO Rome. 2005;Buffalo Production and Research:249-98.
- Butler JE. Immunoglobulin diversity, B-cell and antibody repertoire development in large farm animals. Rev Sci Tech. 1998 Apr;17:43- 70.
- Kabat EA, Wu TT, Perry HM, Gottesman KS, Foeller C. Sequences of Proteins of Immunological Interest. 5th ed. Bethesda, MD: Public Health Service, U. S. Department of Health and Human Services, National Institutes 205 of Health, 1991.
- Berens SJ, Wylie DE, Lopez OJ. Use of a single VH family and long CDR3s in the variable 206 region of cattle Ig heavy chains. Int Immunol. 1997 Jan;9:189-99.
- Saini SS, Hein WR, Kaushik A. A single predominantly expressed polymorphic immunoglobulin VH gene family, related to mammalian group, I, clan, II, is identified in cattle. Mol Immunol. 1997 Jun;34:641-51.
- Sinclair MC, Gilchrist J, Aitken R. Bovine IgG repertoire is dominated by a single diversified VH gene family. J Immunol. 1997 Oct 15;159:3883-9.
- Kaushik AK, Kehrli ME, Jr., Kurtz A et al. Somatic hypermutations and isotype restricted exceptionally long CDR3H contribute to antibody diversification in cattle. Vet Immunol Immunopathol. 2009 Jan 15;127:106-13.
- Koti M, Kataeva G, Kaushik AK. Novel atypical nucleotide insertions specifically at VH-DH junction generate exceptionally long CDR3H in cattle antibodies. Mol Immunol. 2010 Jul;47:2119-28.
- Saini SS, Allore B, Jacobs RM, Kaushik A. Exceptionally long CDR3H region with multiple cysteine residues in functional bovine IgM antibodies. Eur J Immunol. 1999 Aug;29:2420-6.
- Shojaei F, Saini SS, Kaushik AK. Unusually long germline DH genes contribute to large sized CDR3H in bovine antibodies. Mol Immunol. 2003 Sep;40:61-7.
- Saini SS, Farrugia W, Ramsland PA, Kaushik AK. Bovine IgM antibodies with exceptionally long complementarity-determining region 3 of the heavy chain share unique structural properties conferring restricted V222 H+V-lambda pairings. International Immunology.2003 Jul;15:845-53.
- Pasman Y, Saini SS, Smith E, Kaushik AK. Organization and genomic complexity of bovine lambda-light chain gene locus. Vet Immunol Immunopathol. 2010 Jun 15;135:306-13.
- Mousavi M, Rabbani H, Pilstrom L, Hammarstrom L. Characterization of the gene for the membrane and secretory form of the IgM heavy-chain constant region gene (C mu) of the cow (Bos taurus). Immunology. 1998 Apr;93:581-8.
- Saini SS, Kaushik A. Origin of bovine IgM structural variants. Mol Immunol. 2001 Sep;38:389-96.
- Zhao Y, Kacskovics I, Pan Q et al. Artiodactyl IgD: the missing link. J Immunol. 2002 Oct 15;169:4408-230 16.
- Xu B, Wang J, Zhang M et al. Expressional Analysis of Immunoglobulin D in Cattle (Bos taurus), a Large Domesticated Ungulate. PLoS One. 2012;7:e44719.
- Hassanane MS, Gu F, Chowdhary BP, Andersson L, Gustavsson I. In situ hybridization 233 mapping of the immunoglobulin gamma heavy chain (IGHG) gene to chromosome 20q23-q25 in river buffaloes. Hereditas. 1993;118:285-8.
- Satija KC, Rajpal S, Pandey R, Sharma VK. Electrophoresis of buffalo (bos bubalis) serum proteins including immunoglobulins. Infect Immun. 1979 May;24:567-70.
- Svasti MR, Prawatmuang P, Vajanamarhutue C, Kajadphai A, Wangthammang ST, N. The presence of two IgG subclasses in water buffalo immunoglobulins. J Sci Soc Thailand. 1976;2:56-66.
- Patri S, Nau F. Isolation and sequence of a cDNA coding for the immunoglobulin mu chain of the sheep. Mol Immunol. 1992 Jul- Aug;29:829-36.
- Putnam FW, Florent G, Paul C, Shinoda T, Shimizu A. Complete amino acid sequence of the Mu heavy chain of a human IgM immunoglobulin. Science. 1973 Oct 19;182:287-91.
- Rice P, Longden I, Bleasby A. EMBOSS: the European Molecular Biology Open Software Suite. Trends Genet. 2000 Jun;16:276-7.





