CCR5 Genotyping and Chemokine Receptor usage among HIV-1 Treatment - Naive and Experienced Patients in India
Vadwai V, Mandsaurwala A, Mukherjee S, Vora S, Das BR*
SRL Ltd., Primer Square Building, Plot No. 1, Gaiwadi Industrial Estate, S.V. Road, Goregaon (W), Mumbai, India.
*Corresponding Author
Dr. Bibhu Ranjan Das,
SRL Limited, Goregaon (W),
Mumbai-400062, India.
Tel: 022-6780 1212 / 9820227743
E-mail: brdas@srl.in
Received: July 27, 2015; Accepted: December 02, 2015; Published: December 03, 2015
Citation: Das BR, et al., (2015) CCR5 Genotyping and Chemokine Receptor usage among HIV-1 Treatment - Naive and Experienced Patients in India. Int J AIDS Res. 02(5), 43-45. doi: dx.doi.org/10.19070/2379-1586-1500010
Copyright: Das BR© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The reverse transcriptase and protease inhibitors form the backbone of the AIDS control programme in India. Increasing reports on transmitted and second line antiretroviral resistance alarms the need for new drugs that could be used for effective patient management. In 2007, the Food and Drug Administration approved the use of CCR5 antagonist in HIV-1 infected treatment-experienced patients. Thus, we aimed to determine the clinical feasibility of using CCR5 antagonist in HIV-1 infected treatment naïve (n=23) and experienced (n=22) patients. Cotropism testing, CCR5 genotyping and mutational resistance profile for first - and second - line antiretroviral drugs were determined for each patient. None of the patients (0%, 0/45) conferred mutant CCR5 genotype. HIV-1 subtype ‘C’ was found to be predominant in 95.6% (43/45, 95% CI:84-100) patients, while 4.4% patients (2/45, 95% CI:0-16) were infected with circulating recombinant forms. Mutational testing reported 43.4% (10/23, 95% CI:26-63) treatment naive and 36.3% (8/22, 95% CI:20-57) treatment experienced - patients to confer first - and/or second- line antiretroviral drug resistance. Further, cotropism testing revealed use of R5 coreceptor for viral entry in 80% (8/10, 95% CI:48-95) treatment naive and 37.5% (3/8, 95% CI:13- 70) treatment experienced- drug resistant patients; indicating CCR5 antagonists should be considered for treating HIV-1 infected patients in India.
2.Introduction
3.Materials and Methods
3.1.Setting and study approval
3.2.Routine specimen testing
3.3.Molecular laboratory testing
3.4.Statistical analysis
4.Results and Discussion
5.Conclusion
7.References
Keywords
Cotropism; CCR5; Treatment; India.
Introduction
Human immunodeficiency virus (HIV) enters the host cell through an interaction between its envelope protein (gp120) and the host chemokine receptors, CCR5 and/or CXCR4. Viruses using the CCR5 receptor are known as R5-tropic viruses, those using CXCR4 receptor are known as X4-tropic viruses and those using both receptors are known as dual-tropic viruses. CCR5 coreceptor has been used especially during initial infection, whereas CXCR4 coreceptor would be used much later in HIV infection when the infected individual would be progressing towards AIDS. Two mechanisms are known that could inhibit the fusion of the HIV envelope with the CCR5 coreceptor: 1) a 32-base pair (bp) deletion in the host CCR5 gene that results in a conformational change of the chemokine receptor and inhibits its interaction with the virus; and 2) use of CCR5 antagonists.The use of CCR5 antagonists is highly dependent on the coreceptor usage by the virus; and this could be predicted by analyzing the variable 3 region of the gp120 using bioinformatic algorithms like geno2pheno coreceptor [1].
The HIV-1 pandemic in India is characterized by the predominance of subtype ‘C’ conferring 1-7% and 2-20% primary resistance to reverse transcriptase and protease inhibitors respectively [2]. Hence, use of CCR5 antagonist could have great therapeutic implications in HIV-1 infected patients conferring transmitted drug resistance. A prior study from India has demonstrated a high prevalence of R5 tropism among HIV-1 subtype ‘C’ strains [3], but lacked paired data on CCR5 genotyping and genotypic resistance profile for reverse transcriptase and protease inhibitors. Thus, the objective of our pilot study was to estimate the clinical use of CCR5 antagonists in treatment naive and experienced HIV-1 infected patients.
Materials and Methods
The study was performed at a referral diagnostic laboratory at Mumbai and approved by the institutional review board.
EDTA whole blood and plasma samples were received as a part of the routine diagnostic services for CD4/CD8 count (by flow cytometry) and HIV-1 viral load testing (COBAS Taqman, Roche) respectively.
Genotypic drug resistance testing (reverse transcriptase and protease inhibitors) was performed on plasma samples using Viro- Seq HIV-1 Genotyping System version V.2.0, according to the manufacturer’s instructions (Celera, Alameda, California, USA). Sequences obtained were analyzed for resistance conferring mutations using the HIVdb programme of the Stanford University HIV Drug Resistance Database. Cotropism testing and CCR5 genotyping was performed as previously described (using 10% predictive cut-off) [4, 5].
Statistical calculations were performed using SPSS program ver.12.0 (SPSS Inc, Chicago, Illinois, USA). Fisher’s exact test was used to compare categorical variables between the two groups, with p-value < 0.05 considered to be statistically significant. Wilsons bionomial method was used to estimate 95% confidence interval (CI) [6].
Results and Discussion
A total of 45 patients (23, treatment naïve; 22, one-year treatment experienced) with a mean age of 45.1 years (±16.3 years, standard deviation) were included for the study analysis (January, 2015 to April, 2015). None (0% [0/45]; 95% CI:0-7) of the patients reported MTB co-infection and/or other opportunistic infections, unusual sexual behavioral patterns (male having sex with male, female having sex with female, multiple sex partners, incidence of having oral sex) or use of illicit injectible drugs. This information on sexual behavioral patterns and illicit drug use could be incorrect, as patients do not tend to share this information due to the social-stigma associated within the community [7, 8]. Statistical correlation revealed no significant association for CD4, CD8 counts and HIV-1 viral load among patients infected with R5- and X4- tropic viruses irrespective of their treatment status (p > 0.05, Table 1).
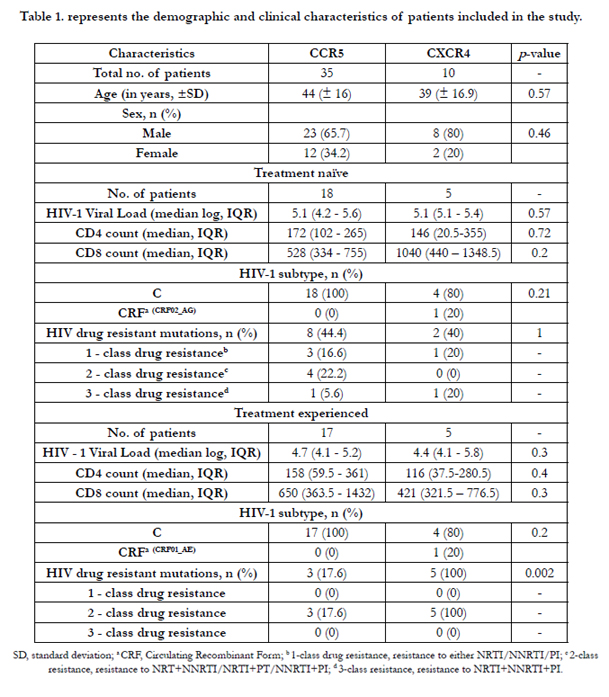

Table 1. represents the demographic and clinical characteristics of patients included in the study.
All patients (100%, 45/45) expressed a wild-type CCR5 genotype, but cotropism testing predicted the usage of X4 co-receptor for cellular entry in 21.8% (5/23) and 22.7% (5/22) HIV-1 treatmentnaive and experienced patients respectively. Previous studies have reported X4-tropic viruses to cause HIV-1 infections in treatment naive patients [3], but its preference for use over CCR5 receptors remains unknown. The finding of X4-tropic viruses in treatmentexperienced patients indicates the progression of the disease, but whether the HIV-1 virus has switched from R5 to X4 phenotype or the primary entry was using the X4 coreceptor cannot be determined [1, 9].
Genotyping analysis revealed the predominance of HIV-1 subtype ‘C’ (95.6% [43/45], 95% CI:84-100) irrespective of treatment status, while 4.4% patients (2/45, 95% CI:0-16) infected with CRF genotypes (CRF02_AG, treatment naive; CRF01_AE, treatment experienced) expressed X4 coreceptor usage (Table 1). Previous studies from West Africa and Europe have reported similar findings, wherein CRF02_AG and CRF01_AE infected individuals used X4 coreceptor for cellular entry [10, 11]. These CRF-infected patients conferred multi-class resistance (CRF02_ AG, NRTI+non-NRTI [NNRTI]+PI resistance; CRF01_AE, NRTI+NNRTI).
A total of 40% (18/45, 95% CI:27-55) conferred first and/or second line antiretroviral resistance (43.4% [10/23], 95% CI:26- 63), treatment naive; 36.3% [8/22, 95% CI:20-57], treatment experienced). Cotropism testing of these drug resistant subtypes revealed the usage of R5 coreceptor in 80% (8/10, 95% CI:48-95) treatment naive and 37.5% (3/8, 95% CI:13-70; p<0.05) treatment experienced patients. This indicates that CCR5 antagonists could be considered as a part of the therapeutic regimen for effective patient management.
Besides, our study also had a few limitations: 1) since there were no baseline genotypic drug resistance pattern for treatment-experienced cohorts, its mutational relevance could not be interpreted, 2) our results are based on a relatively small sample size and needs to be confirmed with a study on a large sample size including diverse HIV-1 subtypes; and, 3) the use of ultra-deep sequencing could help detect the minority viral population (X4 tropic viruses), hence our results could be an over-estimation for the prevalence of R5 coreceptor usage.
Conclusion
Our study revealed a high level of transmitted drug resistance among HIV-1 treatment naive patients; and, CCR5 antagonists should be considered as a part of an effective therapeutic management in both treatment naive and experienced HIV-1 infected Indian patients.
References
- Barmania F, Pepper MS (2013) C-C chemokine receptor type five (CCR5): An emerging target for the control of HIV infection. Applied & Translational Genomics 2: 3-16.
- World Health Organization. The HIV drug resistance report - 2012. World Health Organization, Geneva, Switzerland.
- Neogi U, Prarthana SB, D'Souza G, Decosta A, Kuttiatt VS, et al. (2010) Co-receptor tropism prediction among 1045 Indian HIV-1 subtype C sequences: Therapeutic implications for India. AIDS Res Ther 7: 24.
- Tsai HC, Chou PY, Wann SR, Lee SJ, Chen YS (2015) Chemokine coreceptor usage in HIV-1-infected treatment-naïve voluntary counselling and testing clients in Southern Taiwan. BMJ Open 5: e007334.
- Angelis DSA, Freire WS, Pannuti CS, Succi RC, Machado DM (2007) CCR5 Genotypes and Progression to HIV Disease in Perinatally Infected Children. Braz J Infect Dis 11(2): 196-198.
- Agresti A, Coull B (1998) Approximate is better than “exact” for interval estimation of binomial proportions. Am Stat 52(2): 119-126.
- Vlassoff C, Weiss MG, Rao S, Ali F, Prentice T (2012) HIV-related Stigma in Rural and Tribal Communities of Maharashtra, India. J Health Popul Nutr 30(4): 394-403.
- The magazine of the international red cross and red crescent movement. Stigma, Discrimination and HIV in India. www.redcross.int/EN/mag/magazine2007_2/10-11.html.
- Pollakis G, Abebe A, Kliphuis A, Chalaby MI, Bakker M, et al. (2004) Phenotypic and Genotypic Comparisons of CCR5- and CXCR4-Tropic Human Immunodeficiency Virus Type 1 Biological Clones Isolated from Subtype C-Infected Individuals. J Virol 78(6): 2841-2852.
- Esbjörnsson J, Månsson F, Martínez-Arias W, Vincic E, Biague AJ, et al. (2010) Frequent CXCR4 tropism of HIV-1 subtype A and CRF02_AG during late-stage disease - indication of an evolving epidemic in West Africa. Retrovirology 7: 23.
- Chalmet K, Dauwe K, Foquet L, Baatz F, Seguin-Devaux C, et al. (2012) Presence of CXCR4-using HIV-1 in patients with recently diagnosed infection: correlates and evidence for transmission. J Infect Dis 205(2): 174-184.





