A Post-Mortem Diagnosis of Idiopathic Giant Cell Myocarditis Presenting as Sudden Death: A Report of Two Cases
Purwa Patil1, Varsha Bhatia2*, Vidya Arole2
1 Associate Professor Grant Government Medical College and Sir JJ Group of Hospitals,Mumbai.
2 Assistant Professor Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai.
*Corresponding Author
Dr. Varsha Bhatia,
Department of Pathology, Grant Government Medical College & Sir JJ Group of Hospitals,
Mumbai, India.
Tel: 9867571769
E-mail: drvarshabhatia@gmail.com
Received: October 20, 2015; Accepted: November 27, 2015; Published: December 02, 2015
Citation: Purwa Patil, Varsha Bhatia, Vidya Arole (2015) A Post-Mortem Diagnosis of Idiopathic Giant Cell Myocarditis Presenting as SuddenDeath: A Report of Two Cases. Int J Forensic Sci Pathol. 3(12), 215-217. doi: dx.doi.org/10.19070/2332-287X-1500051
Copyright: Bhatia V© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Giant cell myocarditis is also known as ‘Granulomatous myocarditis’, of which Idiopathic giant cell myocarditis (IGCM) is a rare clinicopathological entity. IGCM is known to cause sudden death in healthy adults in the absence of any symptomatic heart disease. While performing autopsies if there is no apparent cause of death the autopsy surgeon must keep in mind IGCM, especially in healthy adults with an unexplained sudden death. We report here series of two cases of unexpected sudden death in an undiagnosed heart disease and the utility of histopathological diagnosis after autopsy when other ancillary techniques are unavailable.
2.Introduction
3.Case Report
3.1.Case 1
3.2.Case 2
4.Discussion
5.Conclusion
6.References
Keywords
Idiopathic Giant Cell Myocarditis; Sudden Death; Autopsy; Histopathology.
Introduction
Myocarditis is a group of inflammatory or infectious diseases of myocardium caused due to immunological destruction or products of toxin [1]. A rare type of myocarditis is Idiopathic giant cell myocarditis (IGCM) which is known to cause sudden death in more than 50% of cases [2]. The incidence of IGCM is very low and it is seen in relatively young and healthy adults [3]. The death is mainly due to heart failure and ventricular arrhythmia [2].
The term 'sudden death' is applied when a person previously in apparent good health falls ill and dies within minutes or few hours. In most postmortem examinations at least a few pathological conditions are identified. The most likely cause of death can be inferred by the pathologist on the basis of past experience and epidemiological studies.
We hereby present the case series of a young male and an adult female who had an unexpected sudden death. The nonspecific nature of their complaints and paucity of clinical signs misguided the clinicians on the potentially lethal outcome.
Case Report
A 15 year young male adult resident of Maharashtra, India was brought dead at Shatabdi Hospital. No other relevant information regarding his past illness and family history was available except that he had one episode of convulsion. Complete medico legal autopsy was performed.
On examination he was thin built, no injury marks.
Head - brain was found pale.
Chest- Both right and left lungs were congested.
Heart- Enlarged in size.
Liver- congested.
Spleen- congested.
Kidney- congested.
Pancreas-congested.
Probable cause of death was kept pending for histopathological examination by Medical Officer.
The above viscera was then sent for histopathological examination to Police Surgery Post mortem (PSPM) section in the Department of Pathology at Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra.
Grossly the weight of complete heart was 300 grams. The pericardial surface was unremarkable. On cutting open, the left ventricular thickness was 1.5 cm. There was diffuse involvement of left sided myocardium with grayish white areas on anterior and posterior wall (Figure 1). All coronary vessels were patent. All valves, chambers, chordae tendinae and papillary muscles were unremarkable. There was no evidence of atherosclerosis or infarction on gross examination. Other organs- cerebrum, cerebellum, lungs, liver, spleen, kidneys and pancreas were unremarkable on gross examination.
Multiple sections from heart revealed interstitial destruction of myocardial fibers with replacement by dense inflammatory cell infiltrate comprising of lymphocytes, plasma cells, macrophages and few eosinophils along with presence of large numbers of multinucleated giant cells (Figure 2a & 2b). The cytoplasm of giant cells showed no evidence of fungal bodies, asteroid or Schuaman’s bodies. Special stains for mycobacteria or fungus were negative.
Based on these histomorphological findings, the diagnosis of idiopathic giant cell myocarditis was given as the cause of sudden death.


Figure 1. Gross photograph of heart shows diffuse involvement of left sided myocardium with grayish white areas on anterior and posterior wall.
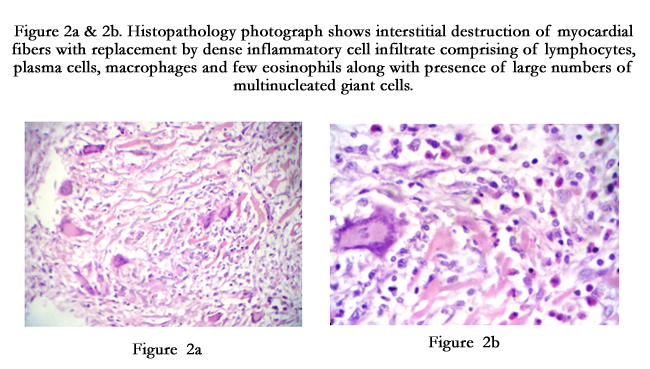
Figure 2a & 2b. Histopathology photograph shows interstitial destruction of myocardial fibers with replacement by dense inflammatory cell infiltrate comprising of lymphocytes, plasma cells, macrophages and few eosinophils along with presence of large numbers of multinucleated giant cells.
A 42 year old female patient resident of Maharashtra, India was brought unconscious and was declared dead at G.T hospital, Mumbai. Patient had no significant medical or family history. Complete medico legal autopsy was performed at G.T hospital, Mumbai.
Moderately built well- nourished female. No evidence of any injury mark.
Brain showed congestion & oedema
Lungs- cut surface showed congestion & oedema
Liver & Spleen were congested
Heart was enlarged in size
Final opinion regarding cause of death was kept pending for histopathology examination.
The above viscera was sent for histopathological examination to Police Surgery Postmortem (PSPM) section in the Department of Pathology at Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra.
Gross and Microscopy Examination was similar to case 1.
Final Cause of sudden death was Idiopathic Giant Cell Myocarditis.


Table 1. Summary of Observations in both the cases.
Discussion
Granulomatous myocarditis, this term was used by Miller to describe the changes in heart in cases of sudden death on autopsy with evidence of myocardial necrosis [4].
Sudden cardiac death is defined as unexpected death within one hour due to cardiac causes in individuals without heart disease [5]. Myocarditis has an incidence of only 1-4% of all cases at autopsy [5]. This may be due to lack of knowledge and awareness of this entity by medical officer performing the medical autopsy. Thus most cases are clinically silent and are diagnosed only at autopsy. Of all myocarditis, IGCM is a rare clinicopathological disease known to cause death in more than half of the cases of sudden death.
IGCM is mainly a disease of young and healthy adults [3] as were seen in our cases. Although there are cases reported in children as well as in older patients [6]. Both sexes are equally affected. The death in patients with IGCM is mainly due to heart failure or ventricular arrhythmias [2], The typical histopathological failure of idiopathic GCM is characterized by a rich cellular infiltration of lymphocytes, macrophages, eosinophils, plasma cells and multinucleated giant cells with necrotic areas [1] which were seen in our cases. Thus disorders associated with giant cells along with necrosis can be mistaken for rheumatic myocarditis, tuberculosis, cryptococcosis, sarcoidosis and syphilitic myocarditis [3]. Thus special stains are helpful to exclude the other disorders. In our cases special stains for mycobacteria and fungi were negative. Also syphilis, sarcoidosis, rheumatic myocarditis have a distinct clinical presentations which were absent in our cases.
Giant cell myocarditis is also associated with autoimmune disorders like inflammatory bowel disease, lymphomas, thymomas, myasthenia gravis and hypersensitivity reactions [2]. In such cases treatment includes immunosuppressive therapy [7]. History related to autoimmune disorder were absent in our cases. Whenever the symptoms are present it is mainly rapidly progressive heart failure or concomitant ventricular arrhythmias [6]. Our patients were completely asymptomatic.
Conclusion
Whenever there is sudden death in young and healthy asymptomatic individuals, a careful and thorough search of cardiac findings at autopsy as well as histopathological evidence of giant cell myocarditis should be made to ascertain the cause of sudden death.
References
- Momin YA, Raghuvanshi SR, Lanjewar DN (2008) Idiopathic Giant Cell Myocarditis Leading to Sudden Death- A Case Report. Bombay Hospital J 50(2): 288-289.
- Permi HS (2014) Idiopathic Giant Cell Myocarditis Presenting as sudden cardiac death- A Rare Case Report. Nitte University Journal of Health Science 4(2): 142-143.
- Kumari K, Mysorekar VV, Praveen S (2012) Idiopathic giant cell myocarditis: A case report. J Clin Diagn Res 6(8): 1425-1427.
- Singh AM, Debnath K, Devi S, Devi G, Konjengbam R, et al. (2003) An Autopsy Case of Sudden Death in a Patient with Giant Cell Myocarditis. Indian J Chest Dis Allied Sci 45: 195-198.
- Konapur PG, Dhaded AV, Udaykumar M (2003) Idiopathic giant cell myocarditis- a case report and review of literature. Indian J Pathol Microbiol 46(2): 241-243.
- Cooper LT, Berry GJ, Shabetai R (1997) Idiopathic giant cell myocarditis- Natural history and treatment. N Engl J Med 336(26): 1860-1866.
- Gamit B, Shah P, Padsala S, Patel RD (2015) Idiopathic Giant Cell Myocarditis leading to sudden death. Pathology and Laboratory Medicine.





