Gastroschisis with Multiple Skeletal Deformities, Imperforate Anus and Absent Genitalia : A Rare Presentation
Asaranti Kar*, Tushar Kar, GD Nayak, Biswal P, Susmita B, S Naik
Department of Pathology & O&G, S.C.B. Medical College, Cuttack, Odisha, India.
*Corresponding Author
Asaranti Kar,
Department of Pathology & O&G, S.C.B. Medical College, Cuttack,
Odisha, 753007, India.
E-mail: asarantikar@yahoo.co.in
Article Type : Case Report
Received: August 24, 2015; Accepted: October 13, 2015; Published: October 16, 2015
Citation: Asaranti Kar, et al., (2015) Gastroschisis with Multiple Skeletal Deformities, Imperforate Anus and Absent Genitalia : A Rare Presentation. Int J Forensic Sci Pathol. 3(10), 190-192. doi: dx.doi.org/10.19070/2332-287X-1500045
Copyright: Asaranti Kar© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Gastroschisis is a rare type of congenital abdominal wall defect involving full thickness of anterior abdominal wall. Out of different varieties, gastroschisis is one of the severe forms with an incidence of about 1 in 10,000 live births. The deformity is more commonly seen in young mothers less than 20 years. They are usually small for gestational age and have a high mortality rate. Only 60% survive till the end of first year. Gastroschisis with intact bowel is known as simple and those with intestinal atresia, perforation and/or necrosis are called complex gastroschisis. Usually it is not associated with any other congenital malformations. We present a rare case of gastroschisis associated with other anomalies like limb defects, kyphosis, talipes equinovarus, imperforate anus, absence of external genitalia and nipples. This congenitally abnormal fetus was delivered by a 23 year old primy at 24 weeks of gestation and was diagnosed by ultrasound.
2.Introduction
3.Case History
3.1.External Examination of fetus (Figure 3a)
4.Discussion
5.Conclusion
6.References
Keywords
Gastroschisis; Imperforate Anus; Kyphosis; Talipes Equinovarus.
Introduction
There are three distinct forms of presentation of congenital abdominal wall defects-gastroschisis, omphalocoele and umbilical cord hernia. Gastroschisis is a defect in the full thickness of anterior abdominal wall through which the abdominal content protrudes into the amniotic cavity [1, 2]. It is more severe and less common. It typically presents to the right of the umbilicus, although the defect may occasionally be to the left also [3]. The defect usually measures about 3-4cm. The organs are free floating in the amniotic fluid. In contrast, omphalocele is in umbilicus and is of small size with organs covered by membrane. In old lesions of gastroschisis, there may be a membrane covering the intestinal
contents.
In most cases, gastroschisis is an isolated birth defect. However, it can be associated with defects like anencephaly, cleft lip and palate, ectopia cordis, atrial septal defect, diaphragmatic hernia, scoliosis and amniotic band syndrome [4]. We hereby report a case of gastroschisis with multiple anomalies inclusive of skeletal defects and others like imperforate anus, absence of external genitalia and nipples with detailed autopsy findings.
Case History
A 23-year old primi aborted a fetus at approximate gestational age of 24 weeks. She did not have any antenatal check up earlier. Ultrasound at 23rd weeks revealed herniation of all abdominal contents outside suggesting a diagnosis of gastroschisis (Figure 1). The dead fetus was sent to Department of Pathology for detailed autopsy examination and confirmation of ultrasonographic diagnosis with finding of any other associated anomalies if any. X-ray examination showed skeletal defects clearly with kyphosis, pelvic abnormalities and talipes equinovarus of both feet (Figure 2).
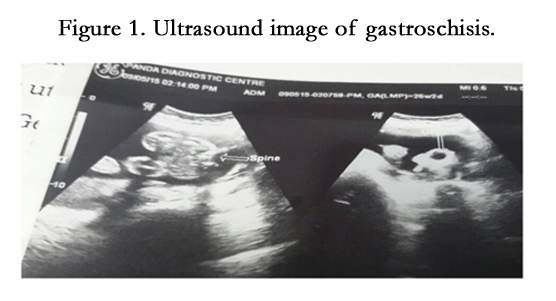

Figure 1. Ultrasound image of gastroschisis.
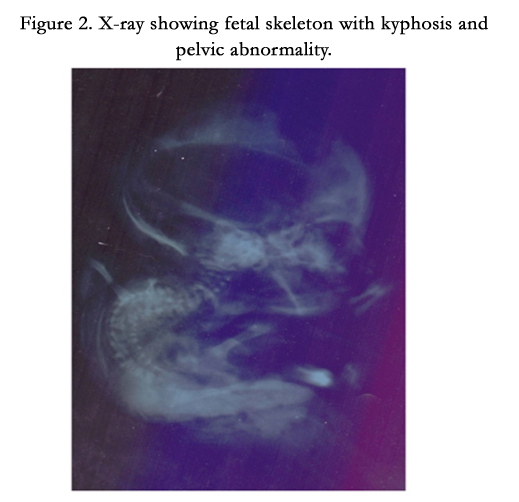
Figure 2. X-ray showing fetal skeleton with kyphosis and pelvic abnormality.
Weight of the fetus was 1.5kg, the crown-rump length -13.5cm, crown heel length -28.5cm, head circumference -21.5cm, chest circumference -14cm and foot length of right and left sides were 4.5cm and 3.5cm respectively. Hair, nail, fingers, toes, palmar creases were present and normal in number. Plantar crease was absent. There was absence of ear cartilage. Thorough examination of the fetus revealed that there was no nipple (Figure 3b) and external genitalia and the anus was imperforate (Figure 4a) and there was talipes equinovarus of both feet (Figure 3c). Both lower limbs were arising from same side (Figure 3d). Autopsy was carried out by giving an inverted Y'shaped incision starting from side of the ear till xiphisternum and then straight till umbilicus. Both flaps were reflected from midline and internal organs were examined for presence of any anomalies. The liver, spleen, kidneys were normal (Figure 4b). Only the GIT was outside. A section of intestine was subjected to histopatholgical examination and did not reveal any abnormality.
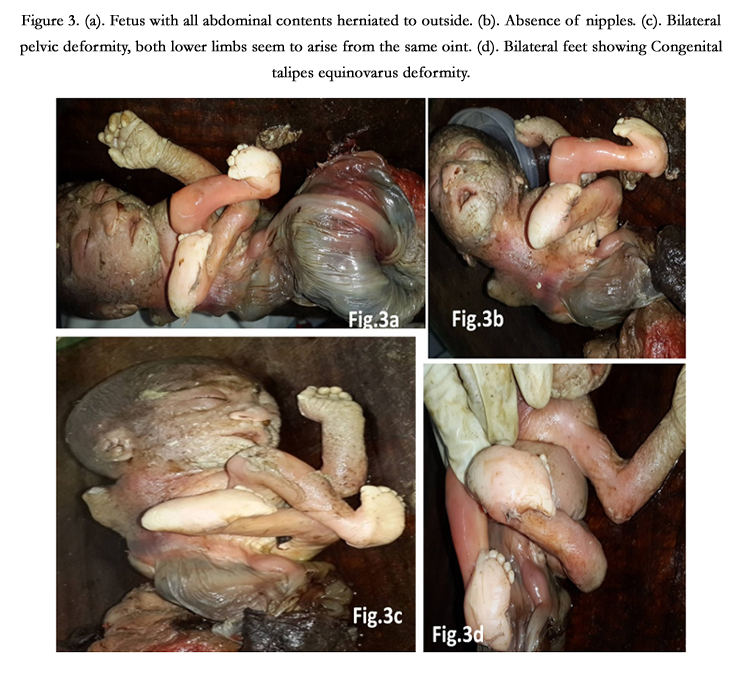

Figure 3. (a). Fetus with all abdominal contents herniated to outside. (b). Absence of nipples. (c). Bilateral pelvic deformity, both lower limbs seem to arise from the same point. (d). Bilateral feet showing Congenital talipes equinovarus deformity.
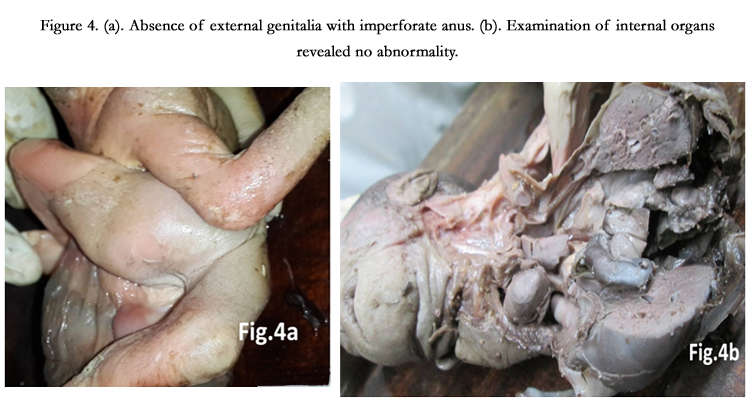
Figure 4. (a). Absence of external genitalia with imperforate anus. (b). Examination of internal organs revealed no abnormality.
Discussion
Gastroschisis is also known as paraomphalocele, laparoschisis, abdominoschisis and abdominal hernia. Contrary to the name gastrochisis it is a body wall musculoskeletal defect, not a gastrointestinal tract defect, but in turn it impacts upon gastrointestinal tract development. There is evisceration of the intestine outside the abdominal wall. It is commonly seen in young mothers less than 20 years of age and affects males predominantly. Gastroschisis can be simple or complex. Simple type presents with an uncompromised bowel whereas complex presents with bowel necrosis, atresia and perforation [5]. Histopathological examination of intestine was carried out and it revealed normal intestinal wall without features of necrosis or any other abnormality, proving the present case as simple gastrochisis.
Extra gastrointestinal manifestations are reported in approximately 5-29% cases which comprise of skeletal, cardiovascular and central nervous system anomalies [6]. Gastroschisis is an embryological developmental defect with male predominance. Causes of this severe congenital malformation may be maternal use of vasoconstrictive drugs like cocaine, ephedrine or smoking. The diagnosis can be made with endovaginal sonography as early as at 12 weeks of gestation [2, 7, 8]. Maternal serum alfafetoprotein (MSAFP) is elevated with fetal gastroschisis. Since MSAFP screening has become widespread, the prenatal diagnosis has increased significantly with about 95% cases being diagnosed at birth [3].
Singer et al., (August 2011) reported a case of ‘Omphalocele and Gastroschisis associated with multiple congenital abnormalities’ in which the baby had spinal deformity, imperforate anus, congenital talipes equinovarus, esophageal fistulas, webbing of neck, left upper limb cyanosis with gastroschisis and omphalocele [9].
The atypicalities of this case are that it was born to a mother older than 20 years, was delivered at 23 weeks but was not small for gestation, associated with skeletal defects like kyphosis, talipes equinovarus and pelvic abnormalities with both limbs arising from same side, imperforate anus, absence of external genitalia and nipples.
Conclusion
Gastroschisis associated with skeletal deformity and other abnormalities as described above is a rare presentation. Maternal factors contribute to developmental defects in the newborn. Regular antenatal check up with ultrasonography and serum alfa-fetoprotein estimation can help in early diagnosis. A detail autopsy examination can reveal all the abnormalities present and thereby aid in syndrome diagnosis and prenatal counselling in future pregnancies. No genetic abnormality has been detected in these cases till now [6] and it could not be done in the above case as the parents did not cooperate.
References
- Sadler TW (2011) Langmans Medical Embryology. (11th edition), Lippincott Williams and Wilkins, US. 227.
- Iyekeoretin Evbuomwan, Kokila Lakhoo, Congenital Anterior Abdominal wall defects: Exomphalos and Gastroschisis. chapter 56, page 348-351. www.global-help.org/publications/books/help_pedsurgeryafrica56.pdf.
- Durfee SM, Downard CD, Benson CB, Wilson JM (2002) Postnatal outcome of foetuses with the prenatal diagnosis of Gastroschisis. J Ultrasound Med 21(3): 269-274.
- Torfs CP, Lam PK, Schaffer DM, Brand RJ (1998) Association between mother’s nutrient intake and their offspring’s risk of gastroschisis. Teratology 58(6): 241-250.
- Brodnoch TJ, Marven S, Owen A, Johnson P, Kurinczuck JJ, et al. (2011) Gastroschisis: One year outcomes from national cohort study. BMJ 343.
- Ionescu S, Mocanu M, Andrei B, Bunea B, Carstoveanu C, et al. (2014) Differential diagnosis of abdominal wall defects-omphalocele versus gastroschisis. Chirurgia 109(1): 7-14.
- Chabra S, Gleason CA (2005) Gastroschisis: Embryology, Pathogenesis, Epidemiology. NeoReviews 6(11): e493-e499.
- Stoll C, Alembik Y, Dott B, Roth MP (2008) Omphalocoele and Gastroschisis and associated malformations. Am J Med Genet A 146A(10): 1280-1285.
- Singal R, Garg LN, Singal RP, Gupta S, Shahi SR, et al. (2011) Omphalocele and gastroschisis associated with multiple congenital abnormalities. J Med life 4(3): 295-296.





