MicroRNAs as Potential Therapeutic Targets in Peripheral Arterial Disease
Alexis Cunningham MD1 and Ayotunde Dokun MD PhD2*
1 Robert M Bernes Cardiovascular Research Center, University of Virginia Charlottesville, Virginia 22908, USA.
2 Assistant Professor, Division of Endocrinology and Metabolism,Department of Medicine University of Virginia Charlottesville, Virginia 22908, USA.
*Corresponding Author
AyotundeDokun MD PhD,
Assistant Professor,
Division of Endocrinology and Metabolism,
Department of Medicine University of Virginia Charlottesville,
Virginia 22908, USA.
Tel: 434-243-9559
E-mail: doa3q@virginia.edu
Article Type: Research Article
Received: August 19, 2014; Accepted: September 30, 2014; Published: September 30, 2014
Citation: Cunningham A and Dokun AO (2014) MicroRNAs as Potential Therapeutic Targets in Peripheral Arterial Disease. Int J DiabetolVasc Dis Res. 2(6), 67-70. doi: dx.doi.org/10.19070/2328-353X-1400013
Copyright: Dokun AO© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Micro RNAs (miRNAs)are small non-coding RNAs that play a role in many biological processes. Many studies have shown that miRNAs are involved in ischemic conditions and emphasized their role as negative or positive modulators in angiogenesis. In vivo studies using various models bring light to the potential benefits of these miRNAs in perfusion recovery following surgically induced hind limb ischemia (HLI), a model of Peripheral arterial disease (PAD). PAD remains a major healthcare burden, affecting millions of Americans. With little advancement in effective therapy the morbidity and mortality of this disease continues to rise. A better understanding of how miRNAs modulate perfusion recovery may provide a potential effective therapy for PAD.
2.Introduction
3.MicroRNA expression in proangiogenic cells of CLI patients
4.MiRNAs in ischemic vs. non-ischemic muscle
5.Differentially regulated microRNAs in two phenotypically distinct mouse strains
6.MicroRNAs in a diabetic ischemic model
7.MicroRNAs in Arteriosclerosis Obliterans
8.Discussion
9.References
Key Words
MicroRNA, Peripheral arterial disease, Ischemia, Angiogenesis
Introduction
Micro RNAs (miRNAs) are small (~22 nucleotide long) non-coding RNAs that regulate gene expression at the post-transcriptional level by degradation of mRNAs or inhibition of protein translation [1]. The first micro RNA, lin-4, was discovered in Caenorhabditiselegans (C. elegans) by Rosalind C. Lee et al in 1993[2]. Currently,over 1600 miRNA precursors are thought to be included in the human genome, producing over 2,000 mature miRNAs[3]. Initially thought to have little significance it is now known that microRNAs play crucial roles in many biological processes such as cell growth, embryogenesis, apoptosis, and are also involved in numerous disease processes[4].
Peripheral arterial disease is caused by atherosclerosis leading to narrowing of the blood flow to the lower limbs. This leads to two distinct clinical manifestations, symptoms of discomfort and pain on walking known as intermittent claudication (IC) or pain at rest sometimes associated with gangrene or ulceration also known as critical limb ischemia (CLI). Risk factors for PAD include cigarette smoking, diabetes mellitus (type 1 and 2), hypertension, hypercholesterolemia, hyperhomocysteinemia, elevated fibrinogen levels and elevated C-reactive protein level [6]. In individuals with PADand diabetes, the disease is more likely to develop below the knee (femoral-popliteal and tibial) while those without diabetes are more likely to develop proximal disease (aorto-ilio-femoral) [7]. Many individuals with diabetes suffer from peripheral neuropathy, resulting in impaired sensory function. As a result, the classic history of claudication may be less common in these individuals [7]. Moreover, as much as 1/3 to 1/2 of individuals with PAD remain without the 2 classic symptoms of PAD. Approximately 8 millions Americans are affected with PAD, with African Americans having higher rates[8].PAD affects up to 10% of people younger than 70 and 15-20% of those older than 70[9]. About 10% of individuals with IC go on to develop CLI within 5 years[10].Within the first year after presentation an estimated 25% of patients with CLI die, 35% remain alive with amputations, 25% have resolution while 20% continue to be symptomatic[10]. The burden on the health system has been catastrophic, with an estimated 4 billion dollars spent on PAD related treatment in the year 2001[11].
The diagnosis of PAD begins with a thorough history and examination of the patient. Several test are available to diagnose PAD, however themost common initial test used is the ankle-brachial index (ABI). The test involves measuring the blood pressure in the ankle compared to that in the arm to give an idea of the circulation of blood. A normal ABI value ranges from 0.9-1.3, while values ≤ 0.9 are considered diagnostic and values greater than 1.4 are abnormal, indicating non-compressible arteries. In patients with rigid arteries a toe brachial index (TBI) is usually indicated. Beyond the ABI Further tests may be indicated to help localize the occlusion as well as determine disease severity, these include Doppler ultrasound, magnetic resonance angiogram and arteriogram[12].
To date, the general treatment of PAD involves improving walking distance and reducing risk factors to decrease associatedmorbidity and mortality. Two important management strategies involve smoking cessation and exercise[13]. Medications that have been used in the treatment of PAD include cilostazol, statins, calcium channel blockers and antithrombotic therapy[14-17] However, these medications have not been very effective in treating the main defect in PAD i.e they are not very effective in improving perfusion.
The adaptive process of neovascularization following vascular occlusion is an important mechanism involved in perfusion recovery[18]. The area distal to the occlusion suffers from ischemia, which promotes proliferation of preexisting collateral arteries and formation of new capillaries[19]. An approach to the treatment of CLI known as therapeutic angiogenesis has gained some attention. The idea of therapeutic angiogenesis involves promoting the growth of new blood vessels or changes in existing vessels in order to improve blood flow.Although a number of angiogenic factors have been successfully used for therapeutic angiogenesis in pre-clinical models (eg. VEGF, FGF, and HGF), these agents have had very limited success in human clinical studies[6,20,21]. Therefore, other approaches are being investigated to explore the possibility of bringing the promise of therapeutic angiogenesis to fruition. One approach includes the investigation of miRNAs as a potential factor that could be manipulated to improve microvascular blood flow in PAD. This review aims to summarize different approaches that have been used to identify miRNAs involved in PAD and the potential for miRNAs as a therapy for PAD.
MicroRNA expression in proangiogenic cells of CLI patients
The vascular system develops during the process of embryogenesis. This vasculogenesis was initially thought to occur only during embryonic development, howeverit is now known that this process occurs to some degree in the postnatal life[22].Situated within the bone marrow are non-hematopoietic progenitors, including endothelial progenitor cells (EPCs)/ Proangiogenic Cells (PACs)[23]. These EPCs are capable of being recruited to sites of arterial injury to participate in neovascularization[24].Specific markers expressed by these cells include VEGR2, VE-cadherin, CD31 and CD133[25]. Spinetti et al. screened the PACs of CLI patients with and without diabetes and controls for 28 miRs that potentially modulated angiogenesis and found eighteen differentially regulated miRs. Two miRs, miR-15a and 16 were chosen for further analysis based on their potential role in angiogenesis and ischemia. PCR analysis revealed an elevation of miR-15a and 16 in the PACs as well as in the serum of CLI patients with or without diabetes. When hypoxia was used to stimulate ischemia in vitro, increased miR15a and 16 expressionwas noted in healthy PACs. Overexpression of both miRs in PACs increased apoptosis, while inhibition corrected it. Additionally, in vivo studies confirmed that ischemic mouse adductor muscles treated with anti-miR-15a/16 PACs had increased blood flow recovery and arteriole density, while those receiving pre-miR-15a/16 PACs displayed impaired perfusion recovery and a reduced number of capillaries compared to negative controls[26].This model provides preliminary data that PACs enriched with miR15a/16 may serve as a potential therapeutic target in PAD.
MiRNAs in ischemic vs. non-ischemic muscle
A cluster of microRNAs, miR-17~92, has been shown to be upregulated in tumors and promotes tumor angiogenesis[27,28]. Bonaeur et al. showed that this microRNA cluster, particularly mir-92a, is expressed in human endothelial cells. Using a mouse hind-limb ischemic model, they showed an upregulation in the expression of miR-92a in the ischemic limb compared to the nonischemic limb, with maximal effects seen within the first three days following injury. Furthermore, mice injected with an inhibitor, antagomir-92a, had a significant reduction in toe necrosis and improved perfusion compared to those injected with a negative control[29].
Similar results were observed in a different ischemic condition, whereacute myocardial infarction was also found to upregulate miR92a.Bonaeur et al. injected antagomir-92a or a control at various days following left coronary artery occlusion. Mice treated with anatgomir-92a exhibited improved left and right ventricular function compared to controls. Additionally, infarct size and number of apoptotic cells were also reduced. Despite being proangiogenic in tumor cells, miR92a was found to be antiangiogenic in ischemic endothelial cells.
Grundman et al. performed a microarray analysis on RNA isolated from adductor muscle of C57BL/6J mice at baseline and multiple time points following femoral arterial ligation.
They identified numerous miRNAs that were upregulated and downregulated, however, miR-100 was the most consistently downregulatedmiR at day three after femoral artery ligation. To confirm that these changes in expression were related to vascular structures collateral arteries from hind limb at day 3 after femoral artery ligation were isolated. Both the growing collateral arteries of the ischemic limb and the non-proliferating arterial anastomosis of the non-ischemic limb expressed miR-100. However,the expression of miR-100 was significantly decreased in the growing collateral arteries of the ischemic limb compared to nonproliferating, quiescent vessels from ischemic limb. No differences were noted between the growing and quiescent vessel of the non-ischemic limb. Moreover, endothelial cells were isolated and revealed a decrease miR-100 expression in ischemic endothelial cells compared to non-ischemic endothelial cells at day 3 following ligation[30].
To investigate targets of miR-100, endothelial cells over expressing miR-100 were analyzed by micro array which revealed hundreds of potential mRNA targets. These potential targets were entered in two bioinformatics algorithms and 8 targets were common to both, including the mammalian target of rapamycin (mTOR), a proangiogenic gene. Furthermore, inhibition of miR-100 with an anatagomir injection given to C57BL/6J mice before and for two days following hind-limb ischemia resulted in enhanced perfusion recovery measured by Doppler imaging[30].Mice receiving an mTOR inhibitor, rapamycin, resulted in reduction of blood flow recovery following 7 days after femoral artery ligation.
Differentially regulated microRNAs in two phenotypically distinct mouse strains
It has been established that two mouse strains, BALB/cJ and C57Bl/6J, recover differently following hind-limb ischemia (HLI). Whereas the C57Bl/6J strain recovers well following HLI, BALB/cJ miceexhibit poor perfusion recovery[31,32].With this knowledge, Hazarikaet al. performed a miroRNAmicro-array analysis of ischemic gastrocnemius muscles of these two strains and found that C57BL/6J had a greater upregulationof miR-93 following ischemia.The expression of miR-93 was increased in ischemic muscle of C57Bl/6J at a time point when perfusion recovery in both strains were similar (day 3), and remained elevated at day 7 post-surgery. Moreover, the C57BL/6 strain also expressed higher levels of miR-93 in the non-ischemic muscle compared to BALB/c[33].
In vivo studies involving gain of function and loss of function further solidified the role of miR-93 in perfusion recovery. C57Bl/6J mice treated with antagomir-93 at day 0, 7 and 14 post HLI had impaired perfusion starting at day 14 compared to the negative control. Moreover, a gain of function technique in which BALBC/cJ mice received a local intramuscular injection of premiR 93, resulting in overexpression of the miR93, showed enhanced perfusion recovery as well as higher capillary density compared to the negative control. The effects of this microRNA are thought to be the result of multiple genes[33]. Taken together, this unbiased model using distinct phenotypic outcomes between two inbred mouse strains following HLI confirmed miR-93 as the most consistent differentially regulated micro-RNA based on strain and ischemia and solidifies its role in perfusion recovery.
MicroRNAs in a diabetic ischemic model
As stated before, diabetes is a major risk factor for PAD. The hyperglycemic state leads to endothelial cell dysfunction and vessel wall remodeling and thus an increase in ischemic complications [34]. Diabetics have poor recovery following ischemic insults due to impaired reparative angiogenesis[34]. Caporali et al. found an upregulation of miR-503 in cultured conditions mimicking diabetes mellitus (DM) and ischemia. This prompted further in vivo studies of this miR. They used a type 1 diabetic mice model using CD1 male mice and found that expression of miR-503 was significantly higher in the ischemic adductor muscles of diabetic mice compared to non-diabetic and/or non-ischemic controls at day 3 post ischemia[35].
Moreover, efficient inhibition of miR-503 using a decoy for miR-503, Ad.decoymir-503, improved blood flow recovery in diabetic mice as well as increased capillary and arteriolar density in ischemic muscle. The target genes, cdc25A and CCNE1, were down regulated by diabetes mellitus but returned to normal levels by inhibition of miR-503 at day 3 and 21 post ischemia. To further strengthen the role of miR-503 in diabetes and ischemia, it was found that diabetic patients undergoing amputation for CLI had an increase expression of miR-503 in calf muscle compared to non-diabetics and non-ischemic control patients undergoing saphenous vein stripping (n=11 each group, p<0.05)[35].
MicroRNAs in Arteriosclerosis Obliterans
Li et al. designed a study which enrolled 104 patients with arteriosclerosis obliterans (ASO) and 105 age-matched controls in order to determine which miRNAs were differentially expressed between these two groups. Based on their known association with vascular biology, a selected set of miRNAs, (miR-21, miR-221, miR-222, miR-145, miR-143, miR-27b, miR-130a, let-7f, miR-378, miR-210, miR-15, miR-16 and miR-126) were examined in intima samples. Levels of miR-21, miR-130a, miR-27b, let-7f and miR- 210 showed significant increase, while miR-221, miR-222 were downregulatedin diseased samples compared to controls[36].
After establishing the expression levels in the intima, these miRs were then examined in the serum of the 104 ASO patients and105 controls. Results revealed an increase in miR-21, miR-130a, miR-27b and miR-210 with no difference in the expression of miR-221, miR-222 or let-7f. Furthermore, serum levels of mi- R130a, miR27b and miR-210 were increased at each fontaine stage, with the expression of miR-27b significantly increasing with each advancement offontaine stage[36].Taken together these results suggest that these miRNAs may be used as potential risk markers for diagnosing ASO at earlier stages or serve as a severity indicator. With further studies and better understanding of the microRNAs it may be possible to manipulate their effects fto establish a therapeutic agent.
Discussion
Peripheral arterial disease affects millions of individuals worldwide, yet treatment strategies remain subpar. Late diagnosis coupled with ineffective treatment has led to a large burden on the healthcare system as well as increasing mortality rate.Understanding the mechanisms involved in the pathophysiology of PAD is crucial in identifying new therapeutic agents. The ability to form new blood vessels is an important mechanism following occlusion of an artery and multiple studies have shown that many microRNAs play a role in inhibiting and stimulating this angiogenic process. Though surgical intervention has been used in patients with CLI, many patients may not be candidates for such surgical treatment and those experiencing initial success may then face complications such as graft failure or stenosis. Additionally, there is evidence that repairing occlusions of large vessels may not improve perfusion or ABI, suggesting at least in some individuals, the disease is primarily in the microvasculature.
MiRNA’s have been successfully manipulated to improve outcomes in the above preclinical models of PAD.Table 1 suggests a strategy that involves overexpression of miR-93 or inhibition ofmiR-15a, miR-16, miR-92a, miR-100 and miR-503 may be effective. However, many factors must be taken into account in the development of these therapeutic approaches in order to achieve success.For example, the current studies have been inpre-clinical models of PAD in mice, where systemic injection or local injection of microRNA mimics or antagomirs have been used successfully. However, the sort of dosing regimen used in mice may not be translatable to humans. It would be important to determine whether systemic vs local administration would be the most effective in achieving expression of pre-miRNA or antagomirs in the lower extremities of humans with PAD. Another concern is the possibility of off target effects of these miRNAs which has the potential to increase side effects.Research involving microRNAs is evolving due to its emerging roles in disease pathophysiology. With the first therapeutic microRNA currently in phase I clinical trials for the treatment of liver cancer, manipulation of mRNAs holds promise for a potential target for improving patient outcomes in PAD.
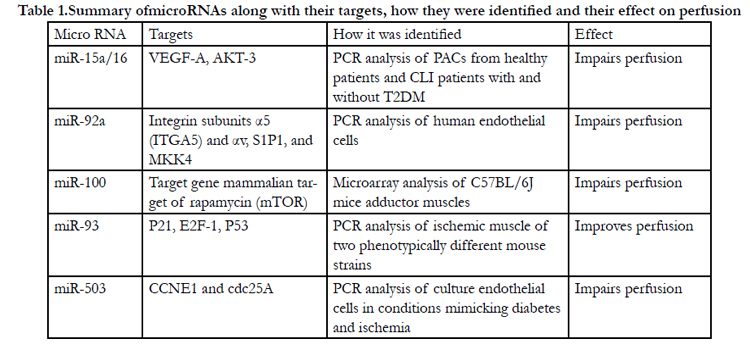

Table 1.Summary ofmicroRNAs along with their targets, how they were identified and their effect on perfusion.
References
- Bartel DP (2004) MicroRNAs: genomics, biogenesis, mechanism, and function. Cell 116: 281-97.
- Lee RC, Feinbaum RL, Ambros V (1993) The C. elegans heterochronic gene lin-4 encodes small RNAs with antisense complementarity to lin-14. Cell 75: 843-54.
- Griffiths-Jones S (2004) The microRNA Registry. Nucleic Acids Res 32(Database issue): D109-11.
- Jiang Q, Wang Y, Hao Y, Juan L, Teng M et al. (2009) miR2Disease: a manually curated database for microRNA deregulation in human disease. Nucleic Acids Res 37(Database issue):98-104.
- Gornik HL and Beckman JA (2005) Peripheral Arterial Disease. Circulation 111:e169-e172.
- Annex, BH (2013) Therapeutic angiogenesis for critical limb ischaemia. Nat Rev Cardiol 10: 387-396.
- American Diabetes Association (2003) Peripheral Arterial Disease in people with diabetes. Diabetes Care 26: 3333-3341
- Allison MA, Ho E, Denenberg JO, Langer RD, Newman AB et al. (2007) Ethnic-specific prevalence of peripheral arterial disease in the United States. Am J Prev Med 32: 328-333.
- Shammas NW (2007) Epidemiology, classification, and modifiable risk factors of peripheral arterial disease. Vasc Health Risk Manag 3: 229-34.
- Woelk CJ (2012) Management of critical limb ischemia. Can Fam Physician 58: 960-963. [11]. Hirsch AT, Hartman L, Town RJ (2008) National health care costs of peripheral arterial disease in the Medicare population. Vasc Med 13: 209-215.
- How Is Peripheral Arterial Disease Diagnosed? 2014; Available from: http://www.nhlbi.nih.gov/health/health-topics/topics/pad/diagnosis.html
- Mukherjee D, Yadav JS (2001) Update on peripheral vascular diseases: from smoking cessation to stenting. Cleve Clin J Med 68: 723-733.
- Dawson DL, Cutler BS, Hiatt WR, Hobson RW 2nd, Martin JD et al.(2000) A comparison of cilostazol and pentoxifylline for treating intermittent claudication. Am J Med 109: 523-530.
- Aronow WS,Nayak D, Woodworth S, Ahn C (2003) Effect of simvastatin versus placebo on treadmill exercise time until the onset of intermittent claudication in older patients with peripheral arterial disease at six months and at one year after treatment. Am J Cardio 92: 711-2.
- Mondillo S, Ballo P, Barbati R, Guerrini F, Ammaturo T et al. (2003) Effects of simvastatin on walking performance and symptoms of intermittent claudication in hypercholesterolemic patients with peripheral vascular disease. Am J Med 114: 359-364.
- CAPRIE Steering Committee (1996) A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 348: 1329-1339.
- Zhang C (2008) MicroRNAs: role in cardiovascular biology and disease. Clin Sci (Lond) 114: 699-706.
- Carmeliet P (2000) Mechanisms of angiogenesis and arteriogenesis. Nat Med 6: 389-395.
- Murakami M, Simons M (2008) Fibroblast growth factor regulation of neovascularization. Curr Opin Hematol 15: 215-220.
- Sengupta S,Gherardi E, Sellers LA, Wood JM, Sasisekharan R et al. (2003) Hepatocyte growth factor/scatter factor can induce angiogenesis independently of vascular endothelial growth factor. Arterioscler Thromb Vasc Biol 23: 69-75.
- Timmermans F,Plum J, Yöder MC, Ingram DA, Vandekerckhove B, et al. (2009) Endothelial progenitor cells: identity defined? J Cell Mol Med 13:87-102.
- Fadini GP, Albiero M, Vigili de Kreutzenberg S, Boscaro E, Cappellari R, et al. (2013)Diabetes impairs stem cell and proangiogenic cell mobilization in humans. Diabetes Care 36: 943-949.
- Iwakura A, Luedemann C, Shastry S, Hanley A, Kearney M, et al. (2003) Estrogen-mediated, endothelial nitric oxide synthase-dependent mobilization of bone marrow-derived endothelial progenitor cells contributes to reendothelialization after arterial injury. Circulation 108: 3115-3121.
- Eggermann J, Kliche S, Jarmy G, Hoffmann K, Mayr-Beyrle U, et al.(2003) Endothelial progenitor cell culture and differentiation in vitro: a methodological comparison using human umbilical cord blood. Cardiovasc Res. 58: 478-86.
- Spinetti G,Fortunato O, Caporali A, Shantikumar S, Marchetti M et al.(2013) MicroRNA-15a and microRNA-16 impair human circulating proangiogenic cell functions and are increased in the proangiogenic cells and serum of patients with critical limb ischemia. Circ Res 112: 335-46.
- Ota A, Tagawa H, Karnan S, Tsuzuki S, Karpas A (2004) Identification and characterization of a novel gene, C13orf25, as a target for 13q31-q32 amplification in malignant lymphoma. Cancer Res 64: 3087-3095.
- Dews M,Homayouni A, Yu D, Murphy D, Sevignani C, et al.(2006) Augmentation of tumor angiogenesis by a Myc-activated microRNA cluster. Nat Genet 38: 1060-1065.
- Bonauer A,Carmona G, Iwasaki M, Mione M, Koyanagi M, et al.(2009) MicroRNA-92a controls angiogenesis and functional recovery of ischemic tissues in mice. Science 324: 1710-1713.
- Grundmann S,Hans FP, Kinniry S, Heinke J, Helbing T, et al.(2011) Micro- RNA-100 regulates neovascularization by suppression of mammalian target of rapamycin in endothelial and vascular smooth muscle cells. Circulation 123: 999-1009.
- Dokun AO, Keum S, Hazarika S, Li Y, Lamonte GM, et al. (2008) A quantitative trait locus (LSq-1) on mouse chromosome 7 is linked to the absence of tissue loss after surgical hindlimb ischemia. Circulation 117: 1207-1215.
- Chalothorn D,Clayton JA, Zhang H, Pomp D, Faber JE (2007) Collateral density, remodeling, and VEGF-A expression differ widely between mouse strains. Physiol Genomics 30: 179-191.
- Hazarika S,Farber CR, Dokun AO, Pitsillides AN, Wang T, et al. (2013) MicroRNA-93 controls perfusion recovery after hindlimb ischemia by modulating expression of multiple genes in the cell cycle pathway. Circulation 127: 1818-1828.
- Spinetti G,Kraenkel N, Emanueli C, Madeddu P (2008) Diabetes and vessel wall remodelling: from mechanistic insights to regenerative therapies. Cardiovasc Res 78: 265-273.
- Caporali A,Meloni M, Völlenkle C, Bonci D, Sala-Newby GB, et al. (2011) Deregulation of microRNA-503 contributes to diabetes mellitus-induced impairment of endothelial function and reparative angiogenesis after limb ischemia. Circulation 123: 282-291.
- Li T, Cao H, Zhuang J, Wan J, Guan M, et al. (2011) Identification of miR-130a, miR-27b and miR-210 as serum biomarkers for atherosclerosis obliterans. Clin Chim Acta 412: 66-70.





