A Cephalometric Evaluation of Oropharyngeal Airway Changes Duing Twin-Block Appliance Treatment
M. J. Trenouth1*, S. R. Desmond2
1 Consultant Orthodontist (Retired), Royal Preston Hospital, Sharoe Green Lane, Preston, England.
2 Formerly Hospital Practitioner in Orthodontics.
*Corresponding Author
M. J Trenouth B.Sc., M.D.S., Ph.D., F.D.S., D.Orth., D.D.O,
Consultant Orthodontist (Retired), Royal Preston Hospital, Sharoe Green Lane, Preston, PR2 9HT, England.
Tel: (+44/1772) 717016
E-mail: michaeltrenouth@hotmail.co.uk
Received: April 7, 2016; Accepted: May 12, 2016; Published: May 17, 2016
Citation: M. J. Trenouth, S. R. Desmond (2016) A Cephalometric Evaluation of Oropharyngeal Airway Changes Duing Twin-Block Appliance Treatment. Int J Dentistry Oral Sci. S4:004,22-30.DOI : dx.doi.org/10.19070/2377-8075-SI04004
Copyright: M. J. Trenouth© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: The research hypothesis under test was that functional orthopaedic treatment with the Twin-block appliance increases the oropharyngeal airway as well as correcting the jaw relationships in class II division 1 patients.
Method: 20 cases, 10 male, 10 female. Age range: 11-18 years, average treatment time 9.4 months were randomly selected from the records of a previously completed prospective trial. Cephalometric radiographs taken before and after treatment were analysed. p, the shortest distance between the soft palate and posterior pharyngeal wall and t, the shortest distance between the tongue and the posterior pharyngeal wall were measured.
Results: There was a statistically significant increase in both p and t after Twin-block appliance treatment (p=0.000). A control group selected from normative data matched individually for age and sex and treatment time showed no change over the same growth period.
Conclusions: In Class II division 1 malocclusion, the oropharyngeal airway is already reduced compared to Class I and Class II. Treatment involving premolar extraction and incisor retraction further reduces the airway as does headgear and is contraindicated. Functional appliance treatment is the method of choice as it enlarges the oropharyngeal airway reducing the potential for obstructive sleep apnoea.
2.Introduction
3.Methods
3.1 Subjects
3.2 Selection criteria
3.3 Interventions
3.4 Outcomes
3.5 Statistics
3.6 Error Analysis
4.Results
5.Discussion
6.Conclusions
7.References
Keywords
Twin-Block Treatment; Oropharyngeal Airway; Obstructive Sleep Apnoea; Cephalometric Analysis; Class II Division 1.
Introduction
In 1902 Pierre Robin invented the monobloc to treat mandibular hypoplasia and glossoptosis [1,2]. The retracted lower jaw and tongue gave rise to airway obstruction which was relieved using the monobloc to restore normal jaw relationships. Glossoptosis caused children to be pigeon chested, fail to thrive and be backward at school [3].
An increase in oropharyngeal airway size after functional appliance treatment was first demonstrated by Grim [4] on a series of six cases using measurements from lateral cephalometric radiographs. Ozbek et al[5] studied 26 patients treated with the Harvold activator and 15 controls. The treated cases showed a statistically significant increase in linear dimensions of the oropharynx taken from lateral cephalometric radiographs compared to no change in the control subjects. Similar studies have been reported by a number of authors using a variety of functional appliances (Table 1). All found a significant improvement in oropharyngeal airway dimensions as a result of functional appliance treatment except for three. Restrepo et al [12] did not report the skeletal changes in their study. Kinzinger et al [13] and Lin et al [14] demonstrated only small skeletal improvements which could well account for the lack of improvement in the oropharyngeal airway. Jena et al [9] found that the Twin-block appliance produced a greater change in the oropharyngeal dimensions than the MPA-IV and this was also reflected by a greater skeletal change.
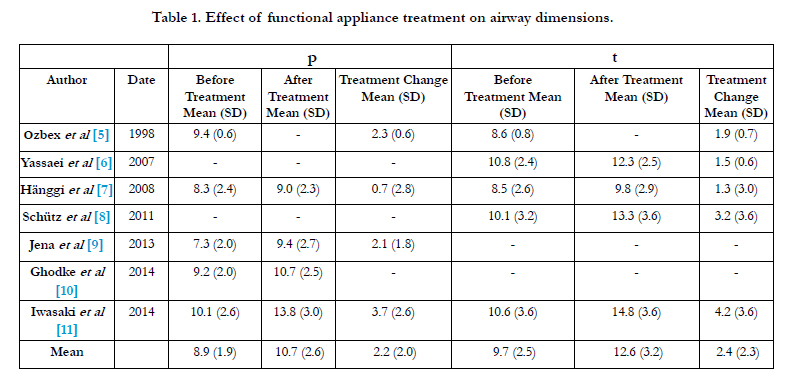

Table 1. Effect of functional appliance treatment on airway dimensions.
Whilst Singh et al [15], Yassaei et al [6] Schütz et al [8] all failed to use a control group; the dimensions of the oropharyngeal airway do not appear to change with age. Mislik et al [16] analysed lateral cephalometric radiographs from 880 patients (412F, 468M) aged 6-17 years. They found neither age-related changes nor sexual dimorphism for p, the shortest distance between the soft palate and the posterior pharyngeal wall and t, the shortest distance between the tongue and the posterior pharyngeal wall. These findings are consistent with those in the control groups of the studies by Ozbek et al [5], Hänggi et al [7], Jena et al [9], Ghodke et al [10], Iwasaki et al [11].
Although a wide variety of different linear measurements of the oropharynx have been used, most studies have included one or both of the following. P, the shortest distance between the soft palate and the posterior pharyngeal wall and t, the shortest distance between the tongue and the posterior pharyngeal wall. Since being introduced by McNamara [17] distances p and t have been used extensively in airway studies [18-21]. Such airway dimensions have been found to be highly reproducible [22].
Clearly a two-dimensional representation of a three-dimensional structure has its limitations [23,24,19]. Ideally three dimensional imaging such as computerised tomography or magnetic resonance imaging are needed for volumetric assessment [23,18]. However, the smallest cross-sectional area is of greatest relevance clinically because the conductance of respiratory gases is dictated by its narrowest part. Linear two dimensional cephalometric measurements relate well to three dimensional magnetic resonance imaging measurements [20]. Riley and Powell [25] reported a high correlation (r=0.92) between posterior airway space on cephalometric radiographs and the volume of the pharyngeal airway on CT scans. Hakan and Palomo [26] used three – dimensional cone beam computed tomography to study 101 patients of differing skeletal classifications. They found that the cross-sectional area at the most constricted region of the tongue base showed the best correlation with oropharyngeal volume (r=0.73 p<0.001). In a three-dimensional cone beam computed tomography study comparing OSA and non-OSA patients, Ogawa et al [27] found that the smallest cross-sectional airway area was the only significant difference between the groups. Systematic reviews have shown lateral cephalometric radiographs to be a reliable screening tool for upper airway obstruction [28,29]. Iwasaki et al [11] used three-dimensional cone beam computed tomography before and after Herbst appliance treatment to measure changes in pharyngeal airway. The increase in oropharyngeal airway volume in the Herbst group (24 patients 11M, 13F) was significantly greater than the control group (20 patients 9M, 11F). They also computed cross-sectional linear distances of the airway. Change in oropharyngeal depth measurements reached the same level of significance (p=0.004) as total airway volume and greater than oropharyngeal volume (p=0.015).
Li et al [30] used cone beam computed tomography to measure volume and cross-sectional area of the oropharyngeal airway before and after Twin-block treatment. Compared to untreated Class II patients the oropharynx and hypopharynx showed significant enlargement. Only two previous studies have evaluated oropharyngeal airway changes in the Twin-block appliance using linear dimensions from lateral cephalometric radiographs [9,10]. These studies only measured distance p but not t and were orientated to measuring the thickness and inclination of the soft palate. The design of the present study was to use p and t to measure the change in oropharyngeal airway size before and after Twin-block appliance treatment.
The hypothesis under test was that functional orthopaedic treatment with the Twin-block appliance increases the oropharyngeal airway as well as correcting the jaw relationships in Class II division 1 patients.
Methods
A consecutive series of patients requiring functional appliance treatment for Class II division 1 malocclusion were selected from a previous prospective study [31]. Records from 20 cases were analysed, 10 males and 10 females, average age 14 years with an age range of 11 to 18 years. The average treatment time was 9.4 months.
A control group was derived from published normative data where this was available. For oropharyngeal dimensions the study of Mislik et al [16] was used. For cephalometric measurements, the normative data published by Bhatia and Leighton [32] derived from London School Children, was chosen because of its nearest geographic proximity. For each set of pre-treatment and posttreatment cephalometric measurements taken from the patient, an equivalent set was derived from normative data tables controlled for age and sex according to the method of Valant and Sinclair [33].
The following inclusion criteria were applied:
• Class II division 1 malocclusion
• Age range 9-20 years
• Overjet greater than 6mm
• ANB angle greater than 4°
The following exclusion criteria were applied:
• Patients with congenital syndromes
• Obvious asymmetry
• Prior appliance therapy
• Crowing requiring extractions
The setting was the Orthodontic department, Royal Preston Hospital District General Hospital, Preston U.K.
The subjects were all treated by the standardised technique described by Trenouth [34]. This involved first, prefunctional semi-rapid maxillary expansion after Mew [35] and alignment of the upper arch. Second, Class II correction using a modification of the Twin-block functional appliance introduced by Clark [36,37] but with steeper bite blocks and excluding the extra oral traction and intermaxillary elastics. Third, retention using an upper removable appliance with a very steep anterior facing bite plane.
The treatment outcome was measured from lateral cephalometric radiographs taken before and after functional appliance treatment. All radiographs were taken on the same equipment, with the teeth in centric occlusion and the Frankfort plane in true horizontal. It was important to standardise head position because Hellsing [38] has shown that variation in head position can alter the oropharyngeal airway dimension. Also taking the records in centric occlusion was important because changing from open to closed jaw position alters the volume of the oropharynx [39]. All subjects were instructed to relax, breath out and not to swallow during radiographic exposure.
The radiographic enlargement was indicated by a millimetre scale incorporated into the machine. The pre and post-treatment radiographs were manually traced by the same operator with a sharp pencil using acetate paper on an illuminated light box.
The following points were located; (Figure 1):
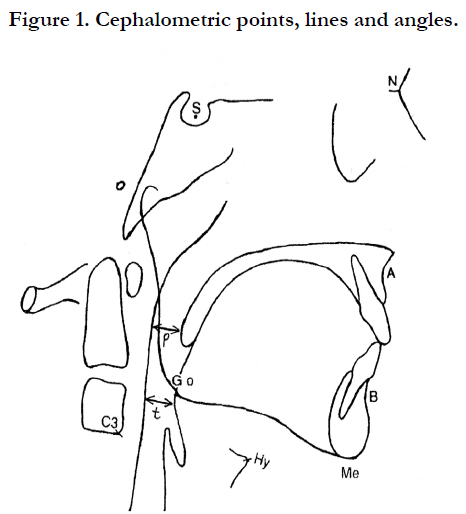
Figure 1. Cephalometric points, lines and angles.
N-Nasion, the most anterior point on the frontonasal suture.
S-Sella, the centre of the sella turcica.
A-Subspinale, the deepest point on the concave outline of the upper labial alveolar process extending from the anterior nasal spine to prosthion.
B-Supramentale, the deepest point on the bony curvature between the infradentale and pogonion.
Go-Gonion – the midpoint at the angle of the mandible.
Me-Menton, the lowest point on the lower border of the mandibular symphysis.
Hy-Hyoidale, the most superior and anterior point on the body of the hyoid bone.
C3-the most anteroinferior point on the third cervical vertebra.
The following distances were measured and corrected for radiographic magnification:
p, the shortest distance between the soft palate and the posterior pharyngeal wall.
t, the shortest distance between the tongue and the posterior pharyngeal wall.
C3 - Hy, C3 - Me, C3 - Go, Hy -Go, Hy -Me, Go- Me.
The following angles were measured:
SNA, SNB and ANB by subtraction of SNB from SNA.
Statistical analysis was carried using Power Analysis Statistical System PASS, and Number Cruncher statistical system, NCSS, UT, USA.
An a priori sample size calculation found that 20 cases were required to detect a 2.5mm difference in primary outcome measure t with a standard deviation of 2.3mm (average of previous studies Table 1) with an 80% power and statistical significance of p<0.01.
The data was found to be normally distributed and a paired t-test used to detect significant differences between the various cephalometric measurements before and after treatment. Statistical significance was set at p<0.01 with non-overlap of confidence limits.
Correlation was also performed between the airway measurements and the other cephalometric measurements that changed during treatment.
An error assessment was performed by retracing 30 of the original 40 cephalometric radiographs selected using random number tables.
The systematic error was determined by calculating the mean of the differences between the first and second tracings (MD) [40]. The 95% confidence intervals were also calculated. This contained zero indicating any systematic bias was not statistically significant (Table 2).
The maximum error (ME) was calculated from the intra-subject standard deviation [40]. When the standard deviations for each subject were plotted against their mean values for each of the eleven variables, no significant relationships were found, nor was there any systematic bias. This indicated that the measurement error did not increase with the measurements increasing magnitude. The mean difference between repeat readings (MD) was less than the maximum error (ME) in all cases indicating an acceptable level of random error (Table 2).
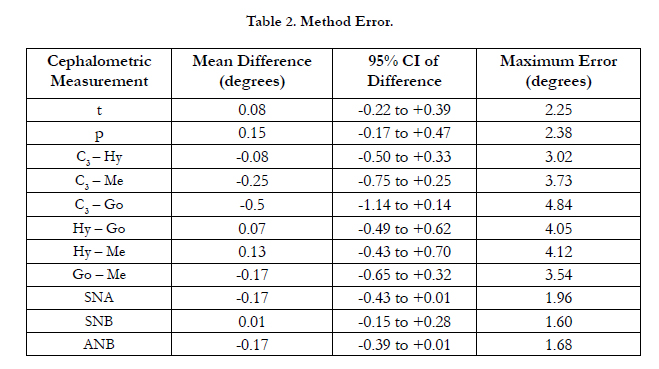
Table 2. Method Error.
Results
For both t and p there was a highly statistically significant increase with non-overlap of confidence intervals for the Twin-block patients during treatment (Table 3). The control group data showed a non-significant difference for the same time period (Table 4).
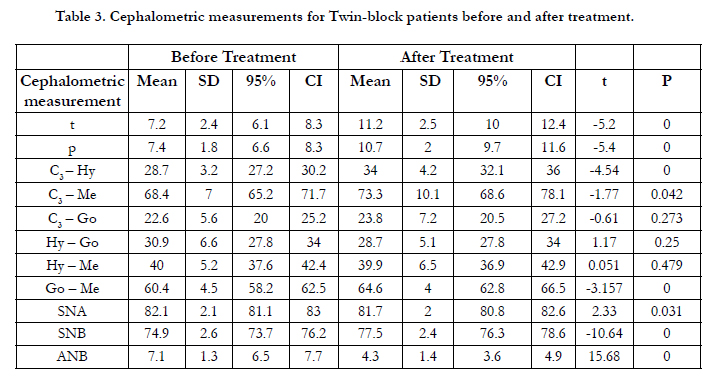
Table 3. Cephalometric measurements for Twin-block patients before and after treatment.
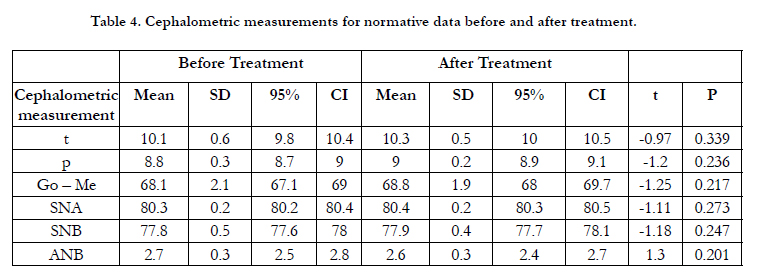
Table 4. Cephalometric measurements for normative data before and after treatment.
In the case of t, the mean increase was 4.0mm compared to 3.2mm for p, which indicates considerable widening of the oropharyngeal airway during treatment. The control data only showed an increase of 0.17mm for t and 0.09mm for p over the same time period. The differences between the change in the Twin-block group and control data was statistically highly significant for both t and p (Table 5).
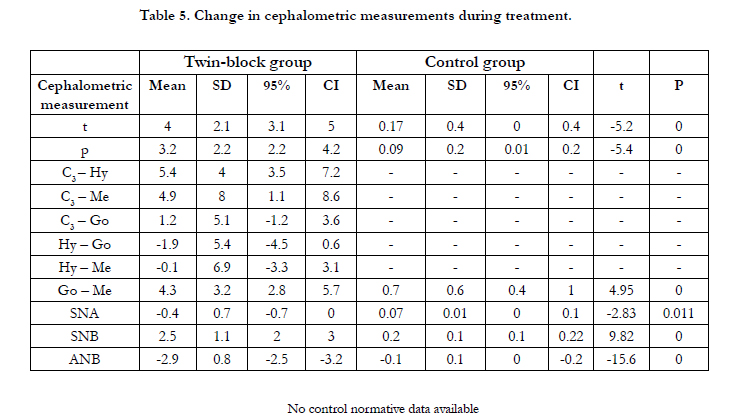
Table 5. Change in cephalometric measurements during treatment.
The distances C3–Hy and Go-Me also increased during treatment to a degree that was statistically significant with non-overlap of confidence intervals (Table 3). There was no control data available for C3–Hy but that for Go-Me showed a non-significant difference (Table 4). C3–Hy distance increased on average by 5.4mm indicating forward movement of the hyoid bone away from the cervical spine as the oropharyngeal airway increased. There was no control data available. Go-Me increased on average by 4.3mm indicating that the mandible lengthened during treatment. The control data changed only by 0.7mm over the same period of time. The difference between the change in the Twin-block group and control data was highly significant for Go-Me (Table 5).
Whilst the distance C3–Me showed a statistically significant increase the confidence intervals overlapped probably due to a large degree of variation (SD) inferring a borderline difference (Table 3). No control data was available for C3–Me. However, the mean increase of 4.9mm was large indicating a forwards movement of the mandible relative to the cervical spine (Table 5).
For the distances C3–Go, Hy–Go and Hy–Me there were small but statistically non-significant changes with overlap of confidence intervals (Table 3). It would seem that the hyoid bone maintained a constant relationship with the mandible.
For angle SNA there was a statistically non-significant change with overlap of confidence intervals (Table 3). The control data showed a non-significant difference (Table 4). The change in SNA in the Twin-block group during treatment was -0.4°. This was statistically non-significant with overlap of confidence intervals when compared to control data (Table 5). Thus the position of the maxilla relative to the cranial base does not appear to change
during treatment.
Both angle SNB and ANB showed a very highly statistically significant change during treatment (Table 3), whilst the control data showed a non-significant change (Table 4). Angle SNB showed a mean increase of 2.5° whilst angle ANB decreased by 2.9°. Both were statistically significant with non-overlap of confidence intervals, when compared to the control data (Table 5). Thus the skeletal reduction in Class II relationship was achieved largely by forward positioning of the mandible during treatment.
Discussion
The results for the distances t and p before and after treatment (Table 3) were comparable to previous studies (Table 1). For the control group normative data (Table 4) there was no significant change in distances t or p during the equivalent treatment period. This was consistent with the findings of previous workers that there was no significant change in the oropharyngeal dimensions during the growth period under study (11 to 18 years). [16,5,7,9-11]. The present study would appear to support the research hypothesis that the dimensions of the oropharyngeal airway t and p were significantly increased by Twin-block functional appliance therapy.
In the present study the distance t showed positive correlation with Go-Me (r = 0.5), C3-Hy (r = 0.3), C3 – Me (r = 0.4) and to a lesser extent SNB (r = 0.2). Trenouth and Timms [41] in a cross-sectional study of 70 subjects aged 10 to 13 years found a similar correlation of t (OPA) with Go-Me (r = 0.3) and C3-Hy (r = 0.3). Similar results were obtained by Hakan and Palmo [26] who found the minimal cross sectional area of the oropharynx correlated with Go-Gn (r = 0.39) to a greater extent than SNB (r = 0.22). Thus increase in the oropharyngeal airway was mainly related to lengthening of the mandible (Go-Me) rather than its position relative to the cranial base (SNB). The hyoid bone tends to follow the mandible as the airway increases. A significant correlation has been found between jaw relation, hyoid position and width of the pharyngeal cavity [42].
Whilst functional appliance therapy increases the oropharyngeal airway dimensions, treatment involving extraction of premolars and incisor retraction has been found to cause a reduction in the airway dimensions [43-45, 47-49]. Similarly the use of headgear has been shown to reduce the oropharyngeal airway [50-52]. In fact a recent review on the link between sleep disordered breathing and Class II malocclusion urged caution when premolar extraction was followed by incisor retraction. They recommended accepting residual overjet to avoid compromising the airway [53].
Oropharyngeal airway size has also been shown to be related to skeletal pattern being greater in Class III than Class II and intermediate in Class I [42,54-58,26,59,60,46,61,62]. Also Class I and Class II subjects with vertical growth patterns have significantly narrower upper pharyngeal airways [63] Class II malocclusion is known to be associated with oral breathing especially where there is mandibular retrusion and increased lower face height [64].
Changes in oropharyngeal airway size with orthognathic surgery have been well documented. Significant reductions occur with mandibular set back osteotomies [65-73]. Mandibular setback combined with maxillary advancement surgery results in a lesser decrease in the oropharyngeal airway with an increase in the nasopharyngeal region [74-78].
The reduction in oropharyngeal airway after mandibular surgery may be compensated for by cervical hyperflexion and so may not show up as suggested by Timms [79] and demonstrated by a number of studies [80,81,68,82,83]. Upper airway reduction can lead to extension of the cranio-cervical angle to relieve the obstruction [84]. Cranio-cervical angle was found to be on average 10 degrees larger in patients with obstructive sleep apnoea [85].
Patients with obstructive sleep apnoea have been shown to have reduced dimensions of the oropharyngeal airway [86-98,24]. Gokce et al [10] found that sagittal distances, cross-sectional area and volume measurements of the oropharyngeal airway all had negative correlation with the apnoea-hypopnea index and positive correlation with sleep efficiency and mean oxygen saturation. Obstructive sleep apnoea syndrome is characterised by signs and symptoms related to arterial oxygen desaturation cessation of breathing resulting in arousal and sleep fragmentation caused by pharyngeal obstruction during sleep.
Obstructive sleep apnoea can result in serious morbidity and mortality mainly as a result of cardiovascular disease and road traffic accidents [99-109]. Children with obstructive sleep apnoea are more prone to having poor learning skills, behavioural problems, attention deficit hyperactivity disorder and depression [110-114].
The site of airway obstruction during episodes of apnoea is usually located in the oropharyngeal region involving the soft palate, dorsum of the tongue and posterior pharyngeal wall. The most constricted area of the airway has an inverse relation to the resistance to air flow. Poiseuille’s law demonstrates that even a modest decrease in the radius of the airway will result in a disproportionate increase in airway resistance (halving the radius results in a 16 times increase in resistance). There have even been reports of cases where mandibular setback surgery actually led to obstructive sleep apnoea [115,116,67]. Alternatively Class II correction using functional appliances has been found not only to enlarge the oropharyngeal airway but to improve nocturnal breathing. Maxillary expansion followed by Herbst appliance treatment has been found to decrease the number of respiratory effort-related arousals and respiratory disturbance index [8].
In conclusion it would seem that Class II patients already have a reduced oropharyngeal airway. Treatment involving extraction of premolars and retraction of incisor segments would further reduce the airway as would headgear. Therefore such an approach would be contra-indicated. Conversely functional appliance treatment would increase the airway dimensions obviating any potential airway problems.
Conclusions
- Simple linear dimensions p, the shortest distance between the soft palate and the posterior pharyngeal wall and t, the shortest distance between the tongue and the posterior pharyngeal wall, correlate highly with three-dimensional volumetric and two-dimensional area measurements and are valid methods of airway assessment.
- Twin-block appliance treatment increases the oropharyngeal airway as demonstrated by a statistically significant increase in both p and t. These findings are supported by previous similar studies published in the literature.
- In Class II division 1 malocclusion the oropharyngeal airway is already reduced compared to Class I and III. Treatment involving premolar extraction and incisor retraction further reduces the airway as does headgear and is contraindicated. Functional appliance treatment is the method of choice as it enlarges the oropharyngeal airway reducing the potential for obstructive sleep apnoea.
References
- Robin P (1902) Observation sur un nouvel appareil de redressement.Rev Stomat 9: 423-432.
- Robin P (1902) Demonstration pratique sur la construction et la mise on bouche d ́un nouvel appareil de redressement. Rev Stomat 9: 561-590.
- Robin P (1934) Glossoptosis due to atresia and hypotrophy of mandible. Amer J Dis Child 48: 541-547.
- Grim DL (1995) Seeing the larger medical picture: Airway enhancement for true orthodontic health. J Gen Orthod 6(3): 5-8.
- Ӧzbek MM, Memikoglu UT, Gögen H, Lowe AA, Baspinar E (1998) Oropharyngeal airway dimensions and functional-orthopedic treatment in skeletal class II cases. Angle Orthod 68(4): 327-336.
- Yassaei S, Bahrololoomi Z, Sorush M (2007) Changes of tongue position and oropharynx following treatment with functional appliance. J Clin Pediatr Dent 31(4): 287-290.
- Hänggi MP, Teuscher UM, Roos M, Peltomäki TA (2008) Long-term changes in pharyngeal airway dimensions following activator-headgear and fixed appliance treatment. Eur J Orthod 30(6): 598-605.
- Schütz TCB, Dominguez GC, Hallinan MP, Cunha TCA, Tufik S (2011) Class II correction improves nocturnal breathing in adolescents. Angle Orthod 81(2): 222-228.
- Jena AK,Singh SP, Utreja AK (2013) Effectiveness of twin-block and mandibular protraction appliance – IV in the improvement of pharyngeal airway passage dimensions in Class II malocclusion subjects with a retrognathic mandible. Angle Orthod 83(4): 728-734.
- Ghodke S, Utreja AK, Singh SP, Jena AK (2014) Effects of twin-block appliance on the anatomy of pharyngeal airway passage (PAP) in Class II malocclusion subjects. Prog Orthod 15: 68-76.
- Iwasaki T, Takemoto Y, Inada E, Sato H, Saitoh I, et al. (2014) Threedimensional cone-beam computed tomography analysis of enlargement of the pharyngeal airway by the Herbst appliance.Am J Orthod Dentofacial Orthop 146(6): 776-785.
- Restrepo C, Santamaria A, Pelaez S, Tapias A (2011) Oropharyngeal airway dimensions after treatment with functional appliances in Class II retrognathic children. J Oral Rehabil 38(8): 588-594.
- Kinzinger G, Czapka K, Ludwig B, Glasl B, Gross U, et al. (2011) Effects of fixed appliances in correcting Angle Class II on the depth of the posterior airway space. J Orofac Orthop 72(4): 301-320.
- Lin Y-C, Lin H C, Tsai H H (2011) Changes in the pharyngeal airway and position of the hyoid bone after treatment with a modified Bionator in growing patients with retrognathia. J Exp Clin Med 3(2): 93-98.
- Singh GD, Garcia-Motta AV, Hang WM (2007) Evaluation of the posterior airway space following Biobloc therapy: Geometric morphometrics. J Craniomandibular pract 25(2): 84-89.
- Mislik B, Hänggi MP, Signorelli L, Peltomäki TA, Patcas R (2014) Pharyngeal airway dimensions: a cephalometric, growth-study-based analysis of physiological variations in children aged 6-17. Eur J Orthod 36(3): 331-339.
- McNamara JA (1984) A method of cephalometric evaluation. Am J Orthod 86(6): 449-469.
- Rodenstein DO, Dooms G, Thomas Y, Liistro G, Stanescu DC, et al. (2001) Pharyngeal shape and dimensions in healthy subjects, snorers and patients with obstructive sleep apnoea.Thorax 45(10): 722-727.
- Finkelstein Y, Wexler D, Horowitz E, Berger G, Nachmani A, et al. (2001) Frontal and lateral cephalometry in patients with sleep-disordered breathing. Laryngoscope 111(4): 634-641.
- Pirila – Parkkinen K, Lopponen H, Nieminen P, Tolonen U, Pääkko E, et al. (2011) Validity of upper airway assessment in children a clinical, cephalometric and MRI study. Angle Orthod 81(3): 433-439.
- Alves M Jr, Franzotti ES, Baratieri C, Nunes LK, Nojima LI, et al. (2012) Evaluation of pharyngeal airway space amongst different skeletal patterns. Int J Oral Maxillofac Surg 41(7): 814-819.
- Malkoc S, Usumez S, Nur M, Donaghy DE (2015) Reproducibility of airway dimensions and tongue and hyoid positions on lateral cephalograms. Am J Orthod Dentofacial Orthop 128(4): 513-516.
- Lowe AA, Gionhaku N, Takeuchi K, Fleetham JA (1986) Three-dimensional CT reconstructions of tongue and airway in adult subjects with obstructive sleep apnoea. Amer J Orthod Dentofacial Orthop 90(5): 364-374.
- Battagel JM, L̀Estrange PR (1996) The cephalometric morphology of patients with obstructive sleep apnoea (OSA). Eur J Orthod 18(6): 557-569.
- Riley RW, Powell NB (1990) Maxillofacial surgery and obstructive sleep apnoea syndrome. Otolaryngol Clin N Amer 23(4): 809-826.
- Hakan E, Palomo JM (2013) An airway study of different maxillary and mandibular sagittal positions. Eur J Orthod 35(2): 262-270.
- Ogawa T, Enciso R, Shintaku WH, Clark GT (2007) Evaluation of crosssection airway configuration of obstructive sleep apnoea. Oral Surg Oral Med Oral Path Oral Radiol Endodont 103(1): 102-108.
- Major MP, Flores-Mir C, Major PW (2006) Assessment of lateral cephalometric diagnosis of adenoid hypertrophy and posterior upper airway obstruction: a systematic review. Am J Orthod Dentofacial Orthop 130(6): 700-708.
- Aboudara C, Nielsen I, Huang JC, Maki K, Miller A J, et al. (2009) Comparison of airway space with conventional lateral head films 3-dimensional reconstruction from cone-beam computed tomography. Am J Orthod Dentofacial Orthop 135(4): 468-479.
- Li L, Liu H, Cheng H, Han Y, Wang C, et al. (2014) CBCT evaluation of the upper airway morphological changes in growing patients of Class II division 1 malocclusion with mandibular retrusion using Twin-block appliance: a comparative research. PLoS ONE 9(4): e94378.
- Trenouth MJ, Desmond S (2012) A randomized clinical trial of two alternative designs of Twin-block appliance. J Orthod 39(1): 17-24.
- Bhatia SN, Leighton BC (1993) A Manual of Facial Growth: A Computer Analysis of Longitudinal Cephalometric Growth Data.(1stedn), Oxford University Press.
- Valant JR, Sinclair PM (1989) Treatment effects of the Herbst appliance. Am J Orthod Dentofacial Orthop 95(2): 138-147.
- Trenouth MJ (1989) A functional appliance system for the correction of Class II relationships. Br J Orthod 16(3): 169-176.
- Mew JCR (1977) Semi-rapid maxillary expansion. Br Dent J 143: 301-306.
- Clark WJ (1982) The twin-block traction technique. Eur J Orthod 4(2): 129-138.
- Clark WJ (1988) The twin-block technique: a functional orthopaedic appliance system. Am J Orthod 93(1): 1-18.
- Hellsing E (1989) Changes in the pharyngeal airway in relation to extension to the head. Eur J Orthod 11(4): 359-365.
- Glupker L, Kula K, Parks E, Babler W, Stewart K, et al. (2015) Three-dimensional computed tomography analysis of airway volume changes between open and closed jaw positions. Am J Orthod Dentofacial Orthop 147(4): 426-434.
- Bland JM, Altman DG (1996) Statistical notes: measurement error. Brit Med J 313(7059): 744.
- Trenouth MJ, Timms DJ (1999) Relationship of the functional oropharynx to craniofacial morphology. Angle Orthod 69(5): 419-423.
- Allhaija ESA, Al-Khateeb SN (2005) Uvulo-glosso-pharyngeal dimensions in different anteroposterior skeletal patterns. Angle Orthod 75(6): 1012- 1018.
- Wang Q, Jia P, Anderson NK, Wang L, Lin J (2012) Changes of pharyngeal airway size and hyoid bone position following orthodontic treatment of Class I bimaxillary protrusion. Angle Orthod 82(1): 115-121.
- Chen Y, Hong L, Wang CL, Zhang S, Cao C, et al. (2012) Effect of large incisor retraction on upper airway morphology in adult bimaxillary protrusion patients. Angle Orthod 82(6): 964-970.
- Shama K, Shrivastav S, Sharma N, Hotwani K, Murrell MD (2014) Effects of first premolar extraction on airway dimensions in young adolescents: A retrospective cephalometric appraisal. Contemp Clin Dent 5(2): 190-194.
- Kim M-A, Park Y-H (2014) Does upper premolar extraction affect the changes of pharyngeal airway volume after bimaxillary surgery in skeletal class III patients? J Oral Maxillofac Surg 72(1): 165 e1-10.
- Germec-Cakan D, Taner T, Akan S (2011) Uvulo-glossopharyngeal dimensions in non-extraction, extraction with minimum anchorage and extraction with maximum anchorage. Eur J Orthod 33(5): 512-520.
- Xu K, Chen W, Liu Y (2010) Effects of large retraction of incisors due to orthodontic treatment on the upper airway dimensions in young adult patients with malocclusion. J Clin Stomatol 26: 600-603.
- Hu Z, Yin X, Liao J, Zhou C, Yang Z, et al. (2015) The effect of teeth extraction for orthodontic treatment on the upper airway: a systematic review. Sleep Breath 19(2): 441-451.
- Hiyama S, Ono T, Ishiwata Y, Kuroda T (2001) Changes in mandibular position and upper airway dimensions by wearing cervical headgear during sleep. Am J Orthod Dentofacial Orthop 120(2): 160-168.
- Godt A, Koos B, Hagen H, Goz G (2011) Changes in upper airway width associated with Class II treatments (headgear vs activator) and different growth patterns. Angle Orthod 81(3): 440-446.
- Pirilä-Parkkinen K, Pirttiniemi P, Nieminen P, Löppönen H, Tolonen U, et al. (1999) Cervical headgear therapy as a factor in obstructive sleep apnea syndrome. Pediatr Dent 21(1): 39-45.
- Kandasamy S, Goonewardene M (2014) Class II malocclusion and sleep disordered breathing. Semin Orthod 20(4): 316-323.
- Muto T,Yamazaki A, Takeda S (2008) A cephalometric evaluation of the pharyngeal airway space in patients with mandibular retrognathia and prognathia and normal subjects. Int J Oral Maxillofac Surg 37(3): 228-231.
- Grauer D, Cevidanes LSH, Styner MA, Ackerman JL, Proffit WR (2009) Pharyngeal airway volume and shape from cone-beam computed tomography: Relationship to facial morphology. Am J Orthod Dentofacial Orthop 136(6): 805-814.
- Zhong Z, Tang Z, Gao X, Zeng X (2010) A comparison study of upper airway among different skeletal craniofacial patterns in non-snoring Chinese children. Angle Orthod 80(2): 267-274.
- Hong J, Oh K, Kim B, Kim Y, Park Y (2011) Three –dimensional analysis of pharyngeal airway volume in adults with anterior position of the mandible. Am J Orthod Dentofacial Orthop 140(4): e161-e169.
- Claudino LV, Mattos CT, Ruellas ACO, Sant’Anna EE (2013) Pharyngeal airway characterization in adolescents related to facial skeletal pattern: A preliminary study. Am J Orthod Dentofacial Orthop 143(6): 799-809.
- Hakan El, Palomo JM (2011) Airway volume for different dentofacial skeletal patterns. Am J Orthod Dentofacial Orthop139(6): e511-e521.
- Ceylan I, Oktay H (1995) A study on the pharyngeal size in different skeletal patterns. Am J Orthod Dentofacial Orthop 108(1): 69-75.
- Kim Y-J, Hong J-S, Hwang Y-I, Park Y-H (2010) Three-dimensional analysis of pharyngeal airway in preadolescent children with different anteroposterior skeletal patterns. Am J Orthod Dentofacial Orthop 137(3): 306-307.
- Abdelkarim A (2012) A cone beam CT evaluation of oropharyngeal airway space and its relationship to mandibular position and dentocraniofacial morphology. J World Fed Orthod 1(2): e55-59.
- De Freitas MR, Alcazar NM PV, Janson G, de Freitas KMS, Henriques JFC (2006) Upper and lower pharyngeal airways in subjects with Class I and Class II malocclusions and different growth patterns. Am J Orthod Dentofacial Orthop 130(6): 742-745.
- Rossi RC, Rossi NJ, Rossi NJC, Yamashita HK, Pignatari SSN (2015) Dentofacial characteristics of oral breathers in different ages: a retrospective case-control study. Progress in Orthod 16: 23.
- Greco JM, Frohberg U, VanSickels JE (1990) Long-term airway space changes after mandibular setback using bilateral sagittal split osteotomy. Int J Oral Maxillofac Surg 19(2): 103-105.
- Enacar A, Aksoy AU, Sencift Y, Haydar B, Aras K (1994) Changes in hypopharyngeal airway space and in tongue and hyoid bone positions following the surgical correction of mandibular prognathism. Int J Adult Orthod Orthognath Surg 9(4): 285-290.
- Hochban W, Schurmann R, Brandenburg U, Conradt R (1996) Mandibular setback for surgical correction of mandibular hyperplasia-does it provoke sleep-related breathing disorders? Int J Oral Maxillofac Surg 25(5): 333-338.
- Achilleos S, Krogstad O, Lyberg T (2000) Surgical mandibular setback and changes in uvuloglossopharyngeal morphology and head posture: a shortand long-term cephalometric study in males. Eur J Orthod 22(4): 383-394.
- Tselnik M, Pogrel MA (2000) Assessment of the pharyngeal airway space after mandibular setback surgery. J Oral Maxillofac Surg 58(3): 282-285.
- Kawamata A, Fujishita M, Ariji Y, Arifi E (2000) Three-dimensional computed tomographic evaluation of morphologic airway changes after mandibular setback osteotomy for prognathism. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 89(3): 278-287.
- Eggensperger N, Smolka W, Iizuka T (2005) Long-term changes of hyoid bone position and pharyngeal airway size following mandibular setback by sagittal split ramus osteotomy. J Craniomaxillofac Surg 33(2): 111-117.
- Kawakami M, Yamamoto K, Fujimoto M, Ohgi K, Inoue M, et al. (2005) Changes in tongue and hyoid positions and posterior airway space following mandibular setback surgery. J Craniomaxillofac Surg 33(2): 107-110.
- Muto T, Yamazaki A, Takeda S, Sato Y (2008) Effect of bilateral sagittal split ramus osteotomy setback on the soft palate and pharyngeal airway space. Int J Oral Maxillofac Surg 37(5): 419-423.
- Marsan G, Vasfi Kuvat S, Oztas E, Cura N, Susal Z, et al. (2009) Oropharyngeal airway changes following bimaxillary surgery in Class III female adults. J Craniomaxillofac Surg 37(2): 69-73.
- Mattos CT, Vilani GNL, Sant’Anna EF, Ruellas ACO, Maia LC (2011) Effects of orthognathic surgery on oropharyngeal airway: a meta-analysis. Int J Oral Maxillofac Surg 40(12): 1347-1356.
- Park SB, Kim YI, Son WS, Hwang DS, Cho BH (2012) Cone-beam computed tomography evaluation of short-and long-term airway change and stability after orthognathic surgery in patients with Class III skeletal deformities: bimaxillary surgery and mandibular setback surgery. Int J Oral Maxillofac Surg 41(1): 87-93.
- Gokce SM, Gorgulu S, Gokce HS, Bengi AO, Karacayli U, et al. (2014) Evaluation of pharyngeal airway space changes after bimaxillary orthognathic surgery with a 3-dimensional simulation and modelling program. Am J Orthod Dentofacial Orthop 146(4): 477-492.
- Hart S, McIntyre BP, Kadioglu O, Currier GF, Sullivan SM, et al. (2015) Postsurgical volumetric airway changes in 2-jaw orthognathic surgery patients. Am J Orthod Dentofacial Orthop 147(5): 536-546.
- Timms D (1990) Letter to editor (Re Wenzel A, Williams S, Ritzau M. Relationships of changes in craniofacial morphology, head posture and nasopharyngeal airway size following mandibular osteotomy 1989; 96:138-143). Am J Orthod Dentofacial Orthop 97(1): 29A-30A.
- Wenzel A, Williams S, Ritzau M (1989) Relationships of changes in craniofacial morphology, head posture and nasopharyngeal airway size following mandibular osteotomy. Am J Orthod Dentofacial Orthop 96(2): 138-143.
- Athanaslou AE, Toutountzakis N, Mavreas D, Ritzau M, Wenzel A (1991) Alterations of hyoid bone position and pharyngeal depth and their relationship after surgical correction of mandibular prognathism. Am J Orthod Dentofacial Orthop 100(3): 259-265.
- Cho D, Choi DS, Jang I, Cha BK (2015) Changes in natural head position after orthognathic surgery in skeletal Class III patients. Am J Orthod Dentofacial Orthop 147(6): 747-754.
- Gu GM, Nagata J, Suto M, Anraku Y, Nakamura K, et al. (2000) Hyoid position, pharyngeal airway and head posture in relation to relapse after the mandibular setback in skeletal Class II. Clin Orthod Res 3: 67-77.
- Solow B, Sandham A (2002) Cranio-cervical posture: a factor in the development and function of the dentofacial structures. Eur J Orthod 24(5): 447-456.
- Solow B, Ovesen J, Nielsen PW, Wildschiødtz G, Tallgren A (1993) Head posture in obstructive sleep apnoea. Eur J Orthod 15(2): 107-114.
- DeBerry-Borowiecki B, Kukwa A, Blanks B (1988) Cephalometric analysis for diagnosis and treatment of obstructive sleep apnoea. Laryngoscope 98(2): 226-234.
- Sher AE (1990) Obstructive sleep apnoea syndrome: A complex disorder of the upper airway. Otolaryngol Clin North Am 23: 593-608.
- Riley RW, Guilleminault C, Herran J, Powell N (1983) Cephalometric analysis of flow-volume loops in obstructive sleep apnoea patients. Sleep 6(4): 303-311.
- Bohlman ME, Haponik EF, Smith PL, Allen RP, Bleecker ER, et al. (1983) CT demonstration of pharyngeal narrowing in adult obstructive sleep apnoea. Am J Roentgenol 140(3): 543-548.
- Lyberg T, Krogstad O, Djupesland G (1989) Cephalometric analysis in patients with obstructive sleep apnea syndrome: I. Skeletal Morphology.J Laryngol Otol 103(3): 287-292.
- Lyberg T, Krogstad O, Djupesland G (1989) Cephalometric analysis in patients with obstructive sleep apnea syndrome: II. Soft tissue morphology. J Laryngol Otol 103(3): 293-297.
- Strelzow VV, Blanks RH, Basile A, Strelzow AE (1988) Cephalometric airway analysis in obstructive sleep apnea syndrome. Laryngoscope 98(11): 1149-1158.
- Partinen M, Guilleminault C, Quera-Salva MA, Jamieson A (1988) Obstructive sleep apnea and cephalometric roentgenograms: The role of anatomic upper airway abnormalities in the definition of abnormal breathing during sleep. Chest 93(6): 1199-1205.
- Crumley RL, Stein M, Gamsu G, Golden J, Dermon S (1987) Determination of obstructive site in obstructive sleep apnoea. Laryngoscope 97(3): 301-308.
- Pracharktam N, Nelson S, Hans MG, Broadbent BH, Redline S, et al. (1996) Cephalometric assessment in obstructive sleep apnea. Am J Orthod Dentofacial Orthop 109(4): 410-419.
- Battagel JM, Johal A, Kotecha B (2000) A cephalometric comparison of subjects with snoring and obstructive sleep apnoea. Eur J Orthod 22(4): 353-365.
- Bacon WH, Turlot JC, Krieger J, Stlerle JL (1989) Cephalometric evaluation of pharyngeal obstructive factors in patients with sleep apnoea syndrome. Angle Orthod 60(2): 115-122.
- Pae EK, Lowe AA, Fleetham JA (1997) A role of pharyngeal length in obstructive sleep apnoea patients. Am J Orthod Dentofacial Orthop 111(1): 12-17.
- He J, Kryger MH, Zorick FJ, Conway W, Roth T (1988) Mortality and apnea index in obstructive sleep apnea. Experience in 385 male patients. Chest 94(1): 9-14.
- Gonzalez-Rothi RJ, Foresman GE, Block AJ. (1988) Do patients with sleep apnea die in their sleep? Chest 94(3): 531-538.
- Findley L, Levinson M, Bonnie R (1992) Driving performance and automobile accidents in patients with sleep apnoea. Clin Chest Med 13(3): 427-435.
- Partinen M, Jamieson A, Guilleminault C (1988) Long-term outcome for obstructive sleep apnea syndrome patients mortality.Chest 94(6): 1200- 1204.
- Ancoli-Israel S, Kripke DF, Klauber MR, Fell R, Stepnowsky C, et al.(1996) Morbidity, mortality and sleep-disordered breathing in community dwelling elderly. Sleep 19(4): 277-282.
- Lavie P, Herer P, Peled R, Berger I, Yoffe N, et al. (1995) Mortality in sleep apnea patients: a multivariate analysis of risk factors. Sleep 18(3): 149-157.
- Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, et al. (2000) Association of sleep-disordered breathing, sleep apnea and hypertension in a large community-based study. Sleep Heart Health Study JAMA 283(14): 1829-1836.
- Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, et al. (2001) Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med 163(1): 19-25.
- Barbé, Percás J, Munoz A, Findley L, Antó JM , Agusti AG (1998) Automobile accidents in patients with sleep apnea syndrome. An epidemiological and mechanistic study.Am J Respir Crit Care Med 158(1): 18-22.
- Klitzman D, Miller A (1994) Obstructive sleep apnea syndrome: complications and sequelae. Mount Sinai J Med 61: 113-121.
- Marin JM, Carrizo SJ, Vicente E, Agusti AG (2005) Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 365(9464): 1046-1053.
- Ali NJ, Pitson DJ, Stradling JR (1993) Snoring, sleep disturbance and behaviour in 4-5 year olds. Arch Dis Child 68(3): 360-366.
- Weissbluth M, Davis AT, Poncher J, Reiff J (1983) Signs of airway obstruction during sleep and behaviour developmental and academic problems. J Dev Behav Pediatr 4(2): 119-121.
- Chervin RD, Dillon JE, Bassetti C, Ganoczy DA, Pituch KJ (1997) Symptoms of sleep disorders, inattention and hyperactivity in children.Sleep 20(12): 1185-1192.
- Goldstein NA, Post JC, Rosenfeld RM, Campbell TF (2000) Impact of tonsillectomy and adenoidectomy on child behaviour. Arch Otolaryngol Head Neck Surg 126(4): 494-498.
- Gozal D (1998) Sleep-disordered breathing and school performance in children. Pediatrics 102(3): 612-620.
- Guilleminault C, Riley R, Powell N (1985) Sleep apnea in normal subjects following osteotomy with retrusion. Chest 88(5): 776-778.
- Riley RW, Powell NB, Guilleminault C, Ware W (1967) Obstructive sleep apnea syndrome following surgery for mandibular prognathism. J Oral Maxillofac Surg 45(5): 450-452.





