The Rehabilitation Management of Chronic Disc Displacement of TMJ with a Specific Functional Device: Long Term Results of 141 Patients
Di Paolo C1*, Falisi G2, Costantini S1, Panti F1, Rampello A1
1 Department of Oral and Maxillofacial Sciences, “Sapienza” University of Rome, Italy.
2 Department of Life, Health, and Environmental Sciences, School of Dentistry, University of L’Aquila, Italy.
*Corresponding Author
Carlo Di Paolo,
Professor,
Department of Oral and Maxillofacial Sciences, “Sapienza”
University of Rome, Via Caserta 6, 000161 Rome,
Italy.
Fax: +39 068550353
E-mail: carlo.dipaolo@uniroma1.it
Article Type: Case Study
Received: May 25, 2015; Accepted: June 19, 2015; Published: June 23, 2015
Citation: Di Paolo C, et al., (2015) The Rehabilitation Management of Chronic Disc Displacement of Tmj with a Specific Functional Device: Long Term Results of 141 Patients. Int J Dentistry Oral Sci. S3:001, 1-10. dx.doi.org/10.19070/2377-8075-SI03001
Copyright: Di Paolo C© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Biomechanical intra capsular dysfunctions may develop into a pathological state that leads to the limitation of mouth opening caused by displacement of the articular disc without reduction, called closed lock.
Various surgical and nonsurgical therapies for the treatment of this pathology have been proposed.
Objectives: The aim of this study was to evaluate, through a retrospective longitudinal study, the efficacy and efficiency of the conservative treatment with a new device, called RADICA, specifically designed and patented for chronic joint lock treatment.
Methods: 141 patients were recruited according to specific criteria from those arrived at our observation unit in the decade 2001-2012. All patients were analyzed by measuring and comparing in the short and medium term specific clinical parameters according to the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD). The data were evaluated by descriptive statistics and Kendall Tau-band Goodman and Kruskal's gamma coefficient tests.
Results: The results achieved by the application of the conservative treatment protocol with the RADICA device have shown evident and significant improvements of all parameters related to the functional recovery or to the different painful states analyzed.
Conclusion: In view of these findings, this study suggest that this pathological state should be treated as early as possible to get an effective and efficient therapeutic response that minimizes the progressive alteration of joint structure and limits the increase of comorbidity. Moreover, these data indicate that the distracting RADICA device represents the device of choice for the treatment of TMD joint lock.
2.Introduction
3.Materials and Methods
4.Analysis of Results
4.1 Mouth opening
4.2 TMD pain
4.3 Cervical pain
4.4 Cephalic pain
4.5 Mouth opening
4.6 Joint pain
4.7 Cervical pain
4.8 Cephalic pain
4.9 Efficiency
5.Discussion and Conclusion
6.References
Keywords
TMD; Chronic Closed Lock; Occlusal Appliance Therapy.
Introduction
The literature shows a wide range in the prevalence of signs and symptoms related to temporomandibular disorders (TMD), detected among different populations [1-3]. LeResche estimated that the symptoms related to TMD are present in large segments of the world population, affecting approximately 10% of people over 18 years of age and she still reports that 2% of these patients suffer from a limitation of mouth opening caused by a irreducible disk dislocation (closedlock) [4-6].
This study documents the prevalence of disc displacement without reduction (closed lock) among thousands of consecutive patients requiring a visit for temporomandibular problems, at the Gnathology Service of "Sapienza" University of Rome, between 2001 and 2012.
The closed lock is ranked, among the diagnostic criteria of reference, with the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) and it is classified as an advanced dysfunctional state manifesting in various clinical forms. Among the different treatments proposed in the literature [7-11] for this joint disease, both surgical and conservative approaches are present. At present, literature agrees on the fact that the first treatment choice should be conservative [12], but lacks in suggesting specific treatment programs.
The Gnathology Service of the University of Rome " La Sapienza" has realized over the years a therapeutic conservative noninvasive protocol, developing and patenting a specific occlusal device for the treatment of this dysfunctional state. This device, called RADICA (with patent office dated: September 3, 1991: License number and protocol of 1860 C/1, n°91 A-000571), aims at a gradual rebalancing of the condyle-disc ratio, stimulating the functional recovery and remission of pain, with the goal to cure the disease and prevent regressive adaptations of the joint tissues.
The purpose of this work is to perform a follow-up evaluation of the RADICA treatment for the resolution of the closed lock of the TMJ. To evaluate the efficacy and efficiency of the device, a 20-years retrospective longitudinal study was conducted, through the examination of clinical records of patients admitted to the observation unit for this chronic dysfunctional state. The study is part of a procedure of consecutive controls that the authors perform to evaluate the outcome and thus the suitability of the treatment protocols conducted on TMD patients [13-17].
Material and Methods
The study was performed in 2012. Patients were selected from the medical records (in progressive numerical order, according to the time of registration of the first visit) of the archive of the Gnathology Service of the Head-Neck Department of Policlinic Umberto 1 of the University of Rome " La Sapienza".
The medical record from which this analysis started was the No. 1614 of 10.23.1990; the last record analyzed was the No. 8742 registered on 12.18.2011.
Basic criteria required for the inclusion of the medical record in the study sample were:
- Diagnosis of irreducible dislocation of the articular disc (according to the system RDC\TMD)
- Treatment performed by applying the distracting splint Radica to evaluate the efficacy and efficiency of the therapeutic protocols applied.
All records with a different diagnosis were excluded.
- Limitation of the mouth opening attributed to other causes: systemic diseases, deformities, trauma etc;
- For uniformity reasons and follow-up controls of the results, the following exclusion criteria were also adopted:
- Medical records different from those currently in use, calibrated in relation to the integrated criteria RDC/TMD,
- Absence of follow-up for at least 12 months from the end of the active therapy;
According to these selection criteria, all medical records of patients registered between 1990 and 2001 have been excluded. Therefore, the period examined was that from 01.21.2001 to 06.13.2011. During this period, patients affected by closed lock and treated with conservative methods were 141, representing 5.14% of those treated for TMD (2739).
To further define a homogeneous sample group for the evaluation of the effects of the applied therapeutic protocol, some of these patients were excluded because of the presence of the following problems:
- 7 patients (4.9%) had chosen to refuse the treatment,
- 5 patients (3.5%) had a discontinued therapy,
- 7 patients (4.9%) were treated only with other conservative therapeutic methods, such as drugs, mandibular manipulation and physiotherapy.
- 14 (9.9%) patients had no post-therapy controls longer than,or equal to 12 months.
After selection, the final sample on which the effects of the applied therapeutic protocol were evaluated was composed of 108 patients.
The treatment protocol contemplated the application of the occlusal splint Ra.Di.Ca, administered with appropriate and specific instructions, plus a series of home exercises for the education of mandibular movements.
The evaluation of the treatment protocol efficacy was performed by comparing at time T0 (before treatment), T1 (at the end of treatment) and T2 (more than 12 months after the end of the therapy), the following clinical parameters:
- Mouth opening
- Articular pains
- Cephalic pain
- Cervical pain
The measurement of the compared parameters was carried out by a team of calibrated specialists who used standardized and codified techniques.
- The mouth opening was measured using the coded millimeter caliber techniques.
- Pain and tenderness were measured with the Verbal Numeric Scale (VNS).
Of the 108 patients treated with Radica and home exercises, a group of 39 patients has also performed physiotherapy. The group of 39 subjects also subjected to physiotherapy was analyzed as an autonomous subgroup called GP (physiotherapy group), in order to highlight eventual differences and to evaluate the impact of the association of these two treatments on the closed lock.
The data on the efficacy were then analyzed separately in 10-years age subgroups, created from the sample of 108 patients, in order to highlight any information that could be hidden to other types of analysis.
In order to evaluate the efficacy of the applied therapeutic protocols, the quantitative values measured at T0, T1 and T2, with a millimeter caliber and Verbal Numerical Rating Scale (VNS), were transformed into qualitative values and distributed in four groups:
- Insufficient mouth opening: up to 30 mm.
- Moderate mouth opening: between 31 and 40 mm.
- Moderate-large mouth opening: between 41 and 50 mm.
- Wide mouth opening: over 50 mm.
Similarly, the VNS values were divided into three groups:
- Absent or mild infrequent pain: between 0 and 20.
- Moderate pain: between 30 and 50.
- Severe pain: between 60 and 100.
The results at T0 and T1 were compared through the use of tables and charts and statistically analyzed with Kendall Tau-band the Goodman and Kruskal's gamma coefficient tests.
The diagnosis of the disk dislocation without reduction, in addition to the clinical records coded in accordance with the RDC, also made using the Magnetic Resonance Imaging (MRI) of the TMD in 73.1% (79) of the 108 recruited patients. It was more complicated to submit patients relating to a public facility to a control MRI merely for scientific purposes. The number of patients who agreed to undergo to an MRI post- therapy was 42 (38.8%). On the resonance imaging with open and closed mouth, an evaluation of the articular disc recapture after therapy was performed.
This analysis considered three possible variants:
- Full restore of the condyle-disc ratio;
- Partial restore of the condyle-disc ratio;
- Absence of the restore of the condyle-disc ratio.
The evaluation of the efficiency of the therapy was carried outthrough the detection of:
- Duration of therapy,
- Patient compliance to treatment,
- Issues related to the application of the treatment protocol, such as performing home exercises, respecting the correct timing of device application or device breakage.
It is highlighted that all used splint Radica were constructed following a standardized procedure and by the same laboratory. All the patients were subjected to a protocol with specific application criteria that can be slightly varied, depending on the status of the disease and on the needs of the single patient. The treatment was performed during two phases, the first is more active, lasting not less than 6 weeks and not more than 15, the second was a maintenance and control phase, with a variable duration ranging from 6 to 24 months. The daily application timing in the active phase contemplated the splint application during the sleep hours and for a period ranging from 1 to 3 not consecutive hours during daytime. In the phase of maintenance, the splint has been applied only during daylight hours and for a maximum period of 1 hour for other 4/6 weeks. When necessary, the splint was first joined and then replaced by night or intermittent use stabilization plaques for a period of up to 12 months.
The follow-up control (T2) was made by applying the clinical criteria described above and using the same detection standardized and codified techniques (RDC/TMD) in use during the treatment period, but performed by personnel different from that who followed patients during the therapy.
Analysis of Results
The first data observed are related to the gender and age of the analyzed sample. The female gender represented 86.5% (122) of the 141 observed closed-lock, a data in line with the literature that specifies a very unfavorable ration for women in the prevalence of these pathologies [1, 18-21].
The most frequent reasons for the patient to seek treatment were local pain (51.06%, 72 patients) and limitation of the mouth opening (47.5%, 67 patients). According to their age were divided into subgroups of 10 years each. The purpose of this division was to evaluate possible statistical differences also related to the efficacy analysis.
The youngest patient joining the observation unit was the number 7133, aged 13, while the oldest was the number 7959, aged 75 and the average age of patients was 38.2 years old. Similar data have been reported several times in the literature [19-21].
In these age groups, the average time between the first symptom and the demand for care were calculated. The mean average of the sample cohort was 25.6 months and the patients between 30 and 49 years have waited longer before seeking treatment (34 months).
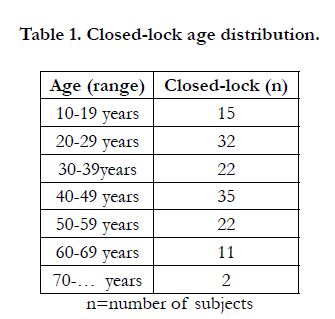

Table 1. Closed-lock age distribution.
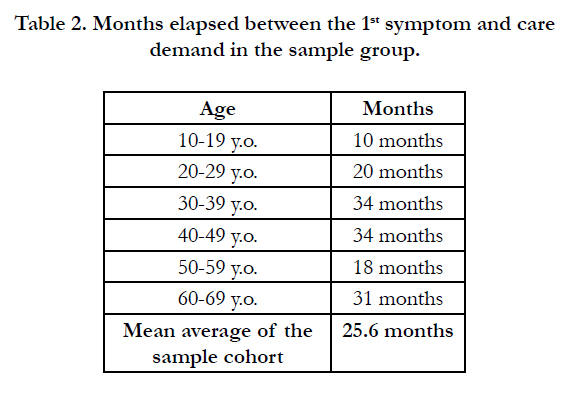
Table 2. Months elapsed between the 1st symptom and care demand in the sample group.
Table 2 shows, the evaluation of the efficacy of Radica treatment was made on the sample of 108 patients, on which the complete therapy protocol had been applied. The results are presented by comparing the semiological parameters related to the mouth opening, TMD, cervical and cephalic pain detected at T0 and T1. At T0, the 108 patients had an average mouth opening of 31.01 mm, with the greatest mouth opening of 45 mm, measured in the patient number 8252, and the minimum mouth opening, 18 mm, measured in the patient number 7332.
The mean articular pain detected with the VNS scale was 63. The maximum pain was 100, observed in 5 patients, and the minimum 30, in 19 patients.
The mean cervical pain was 59.5 and the maximum value of 100 was observed in 6 patients. The minimum value of 0 was found in 38 patients.
The mean cephalic pain was 60.06 and the maximum value 100 was found in 8 patients. The minimum value of 0 was found in 27 patients.
The quantitative values of mouth opening, detected in millimeters, were inserted into four groups of qualitative analysis: insufficient, from 0 to 30, moderate, from 31 to 40, moderate-wide, between 41 and 50 and wide, over 50. The VNS quantitative values were inserted into three groups of qualitative analysis (absent or slight, between 0 and 20; moderate, between 30 and 50 and severe between 60 and 100).
On the basis of this subdivision, the T0 sample of 108 patients showed:
- Mean opening of the mouth (31.01 mm).
- Severe joint pain (63 VNS).
- Mean cervical pain (59.5 VNS).
- Severe cephalic pain (60,06 VNS).
At the check carried out at the end of the treatment (T1), the mean mouth opening detected in the sample was 41.56 mm, while the articular, cervical and cephalic pains were respectively 9.25 VNS, 20.5 VNS and 13.3 VNS. The qualitative analysis of these parameters corresponds to:
- Moderate-wide mouth opening (41.56 mm).
- Absent or mild and intermittent joint pain (9.25 VNS).
- Moderate cervical pain (20.5 VNS).
- Absent or mild and intermittent cephalic pain (13.3 VNS).
- TMD pain 53.75 VNS (85.31%).
- Cervical pain 39VNS (65.54%).
- Cephalic 46.73VNS (77.80%).
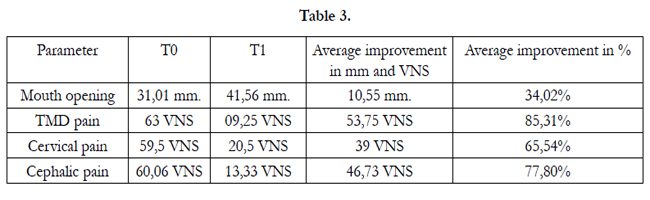
Table 3
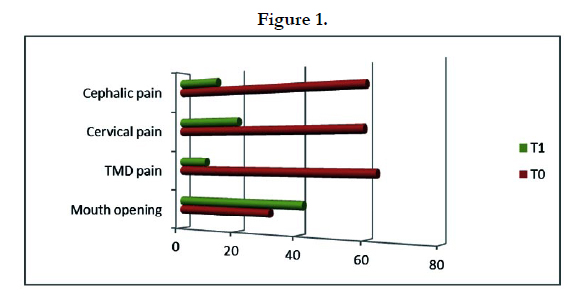
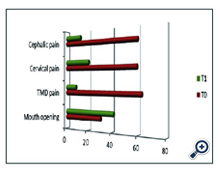
Figure 1
The GP subgroup, created in order to verify the efficacy of the physiotherapy in association with RADICA, has been evaluated with the above mentioned semiological parameters, measured at T0 and T1 and compared with the entire sample (Table 4).
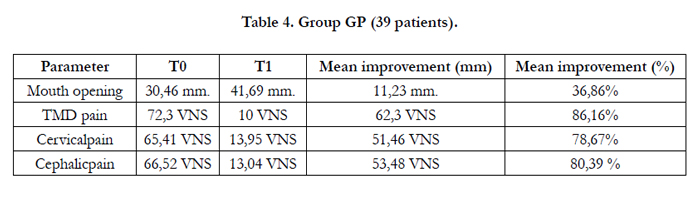
Table 4. Group GP (39 patients)
The analysis of these data, compared to the entire sample, showed an mean increase of mouth opening greater than 0.68 mm (2.84%), an increased reduction of TMD pain of 8.55 VNS (0.85%), a greater reduction of the cervical pain of 12.46 VNS (13.13%), and a greater reduction of the cephalic pain of 6.75 VNS (2.59%).
These data, in line with the results from the literature, show how a multidisciplinary therapy determines the best treatment outcomes. In this case, there was a marked improvement in the cervical pain, additional target of the therapy, compared to the whole sample [28, 29] The following chart compares the improvements achieved with the therapy in the entire sample and in the GP group (Figure 2).
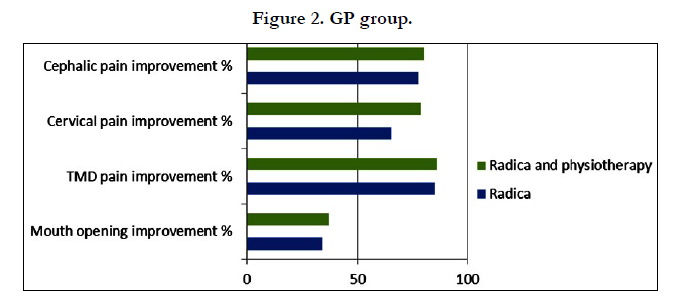
Figure 2. GP group.
The analysis of the treatment outcomes was performed by comparing six age groups, formed according to the decade the patient belongs. Each group has been in turn crossed with the semiological evaluations, reported in the “materials and methods” section, in order to identify possible directions which could not arise with other types of analysis. In the following Table, the mean values of therapeutic outcomes have not been reported, if calculated on fewer than ten patients (Table 5).
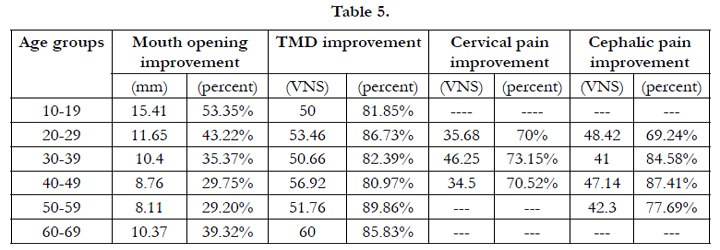
Table 5
The results of the therapies, analyzed by the age groups, show a direct correlation between the increase in mouth opening and the patient's age. With increased age, the increase in mouth opening obtained with therapy decreases, both in terms of millimeters and percentage.
The improvement changes highlighted by the descriptive and qualitative analysis were subjected to statistical evaluation using the Goodman and Kruskal's gamma and the Kendall Tau-band coefficient tests (with correction for ties). For evaluation of these ordinal qualitative data, the coefficients gamma and Kendall Tau-b were preferred. The results are presented in charts and tables.
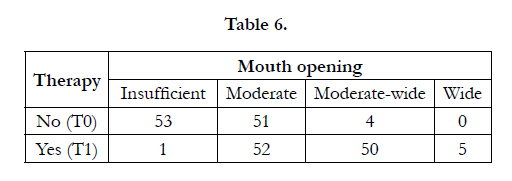
Table 6
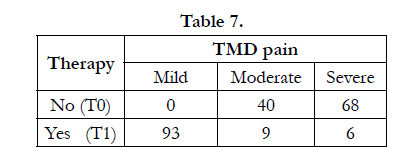
Table 7
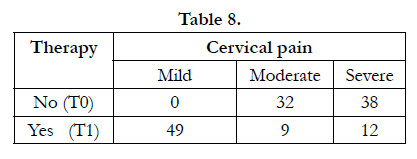
Table 8
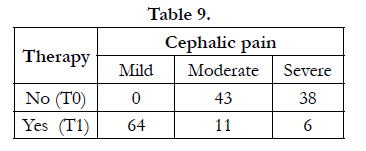
Table 9
It is also observed that at T1, 3 of the 6 severe articular and cephalic pains not responding to the therapy were found in the same patients (numbers 6843, 6667, 7332). They were three female patients, aged respectively 26, 27 and 17 years.
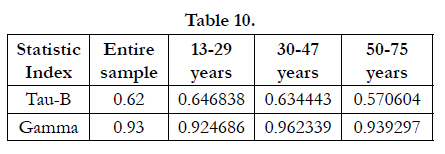
Table 10
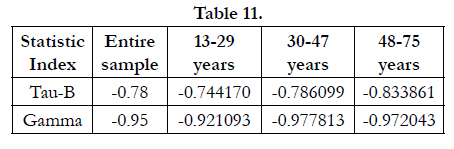
Table 11
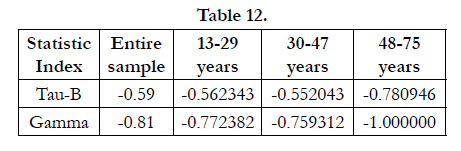
Table 12
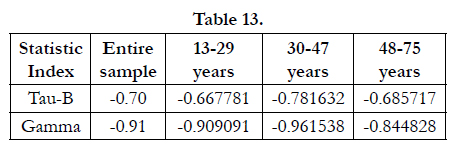
Table 13
The 42 patients who underwent a control MRI showed the following results:
- 10 patients (23.8%) gained a complete condyle-disc ratio.
- 19 patients (45.2%) gained a partial condyle-disc ratio.
- 13 patients (30.9%) did not gain the condyle-disc ratio.
The evaluation of the efficiency of the applied treatments has been carried out in the first place by evaluating the duration of the therapy, including controls and maintenance. Also, the times for recovery of the various examined parameters are shown (minimum, medium and maximum), after which no further improvements were observed. The calculation was made by cutting the ends.
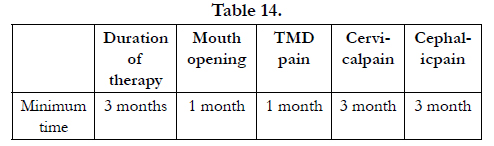
Table 14
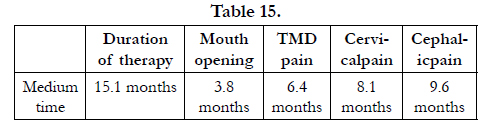
Table 15
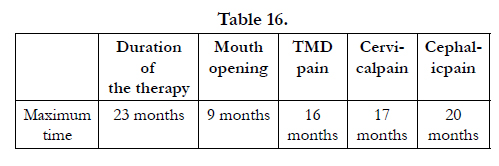
Table 16
In general, the functional recovery (mouth opening) was obtained in a shorter time compared to the joint pain. The latter has improved faster than other investigated types of the pain.
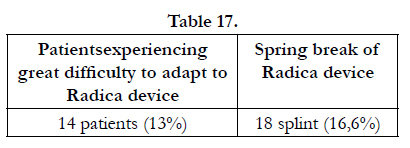
Table 17
It was also found that cases of occlusal joint alteration were not reported, neither clinically nor by patient`s indication.
Of the 108 patients, 8 were free of dental elements in the lower posterior areas.Thus, together with the Radica splint, an inferior not toothed plate was applied, to allow the correct functioning. In the upper arch, no edentulous that could prevent the splint application were found.
The compliance was evaluated by detecting the number of patients who complied with the timing of the application of Radica, an event that the authors consider essential to achieve the therapeutic goals. The 70.3% (76 patients) followed the correct protocol and the 82.4% (89 patients) performed home exercises as prescribed.
The main problems that the occlusal device Radica presented were the obstruction created in the oral cavity and the spring breaks. The latter event sometimes occurred more than once in the same device. The following data refer to the devices requiring at least one spring replacement. It is also specifies that the breaks occurred 2 times in3 patients not affected by parafunctional habits.
Of the 108 patients, 89 (82.4%) have been subjected to a follow- up evaluation of the therapeutic results obtained, at least 12 months after the end of the therapy.
The present slight variations do not show significant percentage changes. Regarding the mouth opening, this remains in the moderate-wide zone. Moreover, all measured pains remain stable between T1 and T2.
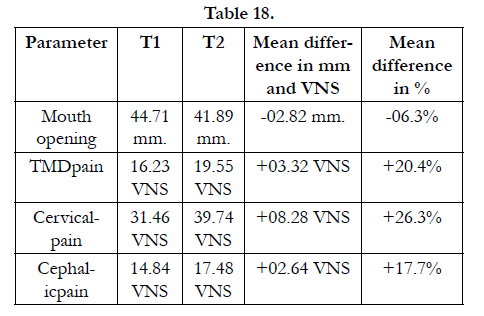
Table 18
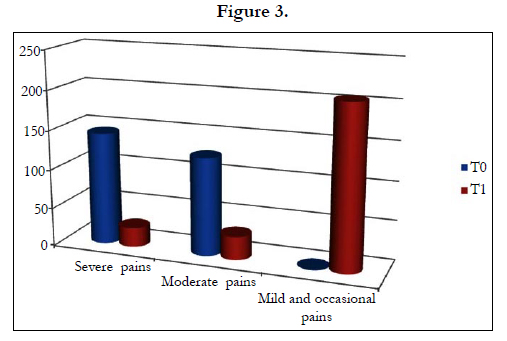
Figure 3
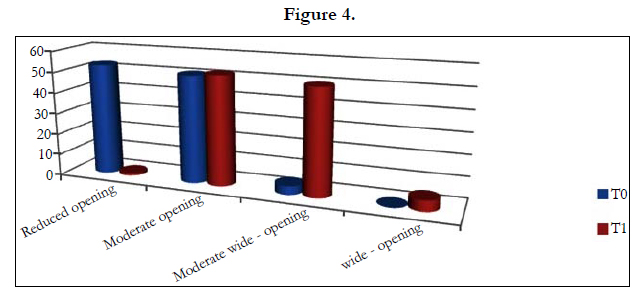
Figure 4
Discussion and Conclusion
This study is a retrospective analysis with longitudinal follow-up of clinical cases. A large amount of data emerged from the evaluation of several semiological parameters. Thus, only the most significant data in relation to the proposed objectives will be discussed, starting from general considerations of epidemiological nature.
During the decade 2001-2011, the Gnathology Service of the Head-Neck Department of the Policlinico Umberto 1, Rome, recorded 2739 consecutive patients with temporomandibular disorders: 141 of them received a diagnosis of irreducible dislocation of the articular disc. The prevalence of this dysfunctional state was found to be 5.14%.
In the literature there are many studies regarding the epidemiological impact of DTM in the population, but few of them indicate the prevalence of the closed lock in the population needing care in a specialized center. Our data, therefore, are in line with those reported by Dahlström in 1998 [30] who registered 1500 consecutive patients requiring treatment for DTM, diagnosed according to the criteria established by the International Classification of Diseases, 9th Revision. The study of Dahlström reported a 6% prevalence of closed lock, similar to that observed in this study.
The examination of anamnestic data shows that during the time between the onset of the disease and the clinical observation (Table 2), variations related to the age were revealed. The mean age of patients was 38.2 years, similar to that found in other studies, the mean age was 40 years and the most affected decade was that between 40 and 49 years (Table 1). Between 30 and 49 years, anaverage time of 34 months between the first symptom and clinical observation was reported, while the average time of the entire sample was 25.6 months (Table 2). The most affected decade is therefore also included in the age groups of patients who waited longer before coming to clinical observation. These patients waited on average nearly 10 months more than the average of the whole sample and two years more than the average recorded in younger patients. These ones, probably because still under the parent care, arrived to clinical observation 10 months after the appearance of the first symptom. The typical course of the disease, characterized by widespread symptoms, often sporadic and, in the case of the closed lock, recessive in signs and symptoms, is considered the cause for the delay in seeking care in all age groups. Meanwhile, the recurring medical history of the path the patient made before reaching the observation unit indicates that the main reasons for such delay are both social commitments typical of this age, and the difficulties in finding specialized centers for a prompt and correct diagnostic-therapeutic framing. For these reasons, the authors believe that the greatest body of submerged diagnoses, widely documented in the literature with a large variability of prevalence, especially refers to the age group between
30 to 49 years.
The experience gained by the Gnathology Service in the examination of these clinical cases and the results obtained by the performed conservative treatments suggest that counteracting this serious pathological state as early as possible may help to achieve better therapeutic results, minimizing the progressive alteration of the joint structures and limiting the increase in comorbidity [31-36] (Table 3). Such consideration is supported by the analysis of the results obtained from the application of the treatment protocol, according to the decade to which the patient belongs (Table 4). The patients in the second decade of life (the first decade of observation), require medical treatment much earlier than the other age groups and are characterized by lower percentages of prevalence of headache and neck pain. At the same time, they also display the greatest recovery of mouth opening after therapy. The percentage data on the increase in mouth opening after the therapy (Table 4) show that the treatments performed on patients in the second decade of life have led to a 53% increase in mouth opening, around 10% more than those performed on patients in the third decade of life who waited twice longer before going the observation unit. The data obtained indicate that the recovery capacity tends to decrease by 2% with the decrease of the decade. This study was not able to determine whether this result is due to the effect of the disease on the joint structures or to the physiological decrease in mouth opening that occurs with age increase [37]. Nonetheless, the findings indicate that the highest percentage of headache and neck pain was recorded among the patients who waited longer before seeking for treatment and the minor percentage among patients who waited less.
Regarding the specific aims of the study, the comparison of clinical data showed that the proposed treatment was found to be very effective in the treatment of the irreducible, chronic and painful TMD disc dislocation.
In particular, the mean differences between functional and pain values detected at T0 and T1are evidenced (Table 3).
- Mean joint pain passed from 63 VNS (T0) to 9.26 VNS (T1), with an average improvement of 85%.
- Mean cervical pain passed from 59.5 VNS (T0) to 20.5 VNS (T1), with an average improvement of 65%.
- Mean cephalic pain passed from 60.06 VNS (T0) to 13.3 VNS (T1), with an average improvement of 78%.
- Mean mouth opening passed from 31.01 mm (T0) to 41.56 mm (T1), with an average increase of mouth opening of 34%.
When the basic gnathological protocol was assisted by physiotherapy (Table 5), the mean cervical pain improved even more significantly, passing from 65.41 VNS (T0) to 13.95 VNS (T1), with an average improvement of 78%.
These findings indicate that, in order to improve the comorbidity between severe headache and closed lock, it is recommended to treat the patient with professional physiotherapy.
The qualitative analysis of the data at T0 and T1 has confirmed the clear positive trend produced by the gnathological treatment for all the analyzed parameters. The descriptive analysis of the severity of joint, cervical and cephalic pain, compared at T0 and T1, has evidenced the following differences:
- Severe pain passed from 144 (55.6% at T0) to 24 (9.2% at T1).
- Moderate pain passed from 115 (44.4% at T0) to 29 (11.2% at T1).
- Absent or mild and occasional pain passed from 0 (T0) to 206 (79.5% T1).
It is outlined that, out of the 24 (9.2%) severe pains reported atT1, 12 (4.6%) were related to the cervical pain, and 9 of these patients (3.4%) were not part of the GP group, thus not treated with the physiotherapy. This finding is a further confirmation of how physiotherapy has been particularly effective in the treatment of cephalic pain in comorbidity with closed lock [38].
The mouth opening, as shown in Table 6, demonstrates a marked improvement in parallel with the pain values.
- The reduced mouth openings passed from 53 (49% at T0) to1 (0.9% in T1).
- The moderate-wide mouth openings increased from 4 (3% at T0) to 50 (46% in T1).
The Kendall Tau-band the Goodman and Kruskal's gamma coefficients, always approaching the extremes +1 and -1, statistically validate the therapeutic results obtained from the application of the treatment protocol.
Shiffman et al. in 2007 established that for the care of the closed lock, the rehabilitation therapy achieved by a muscular splint with indirect action, associated with medical, cognitive behavioral and physiotherapy, generated benefits able to limit the need for surgery to few specific cases [12]. In 2001, Hiroshi Kurita et al., treated 51 joint diseases with a three-dimensional mandibular repositioning device and compared the results through magnetic resonance imaging. The results showed that the mandibular repositioning device is a splint indicated in the treatment of reducible dislocation and occasionally for the not reducible dislocation of the articular disc, but only in cases where the joint structures are slightly altered [39]. The Radica device, created and adapted specifically for the treatment of the closed lock and applied with personalized timing, favored the recapture of the articular disc, decompressing the retrodiscal tissues, initiating their healing and that of the structures associated with them.
The entire therapy lasted on average 15.1 months, with periods ranging from 3 to 23 months. The patients received on average 10 checkup visits, one every 30\50 days.
The observed parameters showed recovery times different from each other and from one patient to another:
- The parameter improving faster was the mouth opening. Recovery times observed ranged from 1 to 9 months. After 9 months, no further improvements were recorded, the average value was 3.8 months, the median value was 4 months and the mode value was 2 months.
- Joint pain recovery times observed ranged from 1to 16 months. After 16 months no further improvements were recorded, the average value was 6.4 months, the median value 6 months and the mode value 2 and 5 months.
- Cervical pain recovery times observed ranged from3to 17 months. After 17 months no further improvements were recorded, the average value was 8.1 months, the median value 8 months and the mode value 9 months.
- Cephalic pain recovery times observed ranged from 3 to 20 months. After 20 months no further improvements were recorded, the average value was 9.6 months, the median value 9 months and the mode value 9 months.
The above data indicate that the articular pain condition is definitely improved three months after the functional recovery (restoration of the mouth opening), while for the relief of the cervical pain a longer time was required, even compared to that of the cephalic pain.
Overall, the patients showed a good compliance.
Secondary alterations of the previous occlusal joint were neither clinically reported by the medical staff of the Service, nor by any patient.
The follow-up control in T2, made at least 12 months after the end of the therapy indicate that the pain and functional values collected at the clinical examination should be considered generally in line with those found at the end of the therapy.
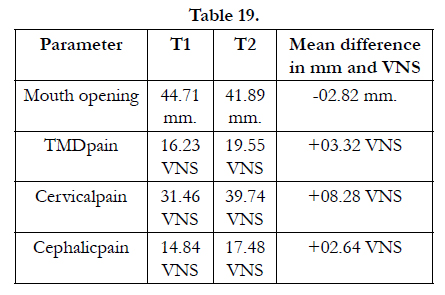
Table 19
Based on the analysis of the short and long term results and from experience gained over the last twenty years, we can say that the device RADICA provides the following benefits:
- Recovery of month opening
- Partial recovery of the articular disc
- Good relief of pain (articular, cephalic and cervical)
- Independence from specific manual skills
- Reproducibility of the application
- Tailor and integrate treatment protocol
Furthermore, the application of RADICA allows the clinician to evaluate, in a few weeks, the response to the treatment of the joint tissues, allowing a differential diagnosis between cases requiring surgical intervention and those that can be solved by the conservative treatments.
The analysis of these data represents an invitation for clinicians to consider this treatment protocol, applied and improved over twenty-five years of clinical experience, among the main options for the treatment of this TMJ pathology.
References
- Poveda Roda R, Bagán JV, Díaz Fernández JM, Hernández Bazán S, Jiménez Soriano Y (2007) Review of temporomandibular joint pathology. Part I: Classification, epidemiology and risk factors. Med Oral Patol Oral Cir Bucal 12(4): E292-8.
- Gesch D, Bernhardt O, Alte D, Schwahn C, Kocher T, et al. (2004) Prevalence of signs and symptoms of temporomandibular disorders in an urban and rural German population: results of a population-based Study of Health in Pomerania. Quintessence Int 35(2): 143-150.
- Macfarlane TV, Blinkhorn AS, Davies RM, Kincey J, Worthington HV (2002) Oro-facial pain in the community: prevalence and associated impact. Community Dent Oral Epidemiol 30(1): 52-60.
- Drangsholt M, LeResche L (1999) Temporomandibular disorder pain. In: Epidemiology of pain. In (edtn), Crombie IK, Croft PR, Linton SJ, LeResche L, Von Korff M. IASP Press, Seattle. 203-233.
- LeResche L (1997) Epidemiology of Temporomandibular Disorders: Implications for the Investigation of Etiologic Factors. Crit Rev Oral Biol Med 8(3): 291-305.
- LeResche L (1995) Research diagnostic criteria for temporomandibular disorders. In: Fricton JR, Dubner R, editors. Orofacial pain and temporomandibular disorders. Raven Press, New York. 189-203.
- Cavalcanti do Egito Vasconcelos B, Bessa-Nogueira RV, Rocha NS (2006) Temporomandibular joint arthrocententesis: evaluation of results and review of the literature. Braz J Otorhinolaryngol 72(5): 634-638.
- Mujakperuo HR, Watson M, Morrison R, Macfarlane TV (2010) Pharmacological interventions for pain in patients with temporomandibular disorders. Cochrane Database Syst Rev 10: 1-53.
- Al-Ani MZ, Davies SJ, Gray RJ, Sloan P, Glenny AM (2004) Stabilisation splint therapy for temporomandibular pain dysfunction syndrome. Cochrane Database Syst Rev.
- Rigon M, Pereira LM, Bortoluzzi MC, Loguercio AD, Cardoso JR, et al. (2011) Arthroscopy for temporomandibular disorders. Cochrane Database Syst Rev.
- Shi Z, Guo C, Awad M (2013) Hyaluronate for temporomandibular joint disorders. Cochrane Database Syst Rev.
- Schiffman EL, Look JO, Hodges JS, Swift JQ, Decker KL, et al. (2007) Randomized Effectiveness Study of Four Therapeutic Strategies for TMJ Closed Lock. J Dent Res 86(1): 58–63.
- Paolo C, Panti F, Rampello A (1998) Retrospective study on the application of occlusal splints in 312 patients with temporomandibular disorders. Minerva Stomatol 47(5): 187-95.
- A Rampello, G Falisi, C Di Paolo, F Panti (2010) A new aid in TMD Therapy: the Universal Neuromuscular Immediate Relaxing appliance “UNIRA”. Oral Implantol (Rome) 3(1): 20-32.
- Paul C, Davide Rampello. A, De Luca S. Therapy non-surgical of the Closed Lock: methods in comparison, RIS September 1991.
- Paolo C, Rampello A (1993) Lock articolare dell’ATM. Terapia non chirurgica. Dental Cadmos 18: 48–74.
- Paul C, E Baldoni (1989) Plaque repositioning nell'incoordinazione condilomeniscale TMJ. XXII National Congress of the Italian Society of Dentistry and Maxillofacial Surgery, Rome 69 December IV. 157–160.
- DA Seligman, AG Pullinger, WK Solberg (1988) The Prevalence of Dental Attrition and its Association with Factors of Age, Gender, Occlusion, and TMJ Symptomatology. J Dent Res 67(10): 1323-1333.
- Daniele Manfredini, Fabio Piccotti, Giuseppe Ferronato, Luca Guarda- Nardini (2010) Age peaks of different RDC/TMD diagnoses in a patient population. Journal of Dentistry 38(5): 392-399.
- White BA, Williams LA, Leben JR (2001) Health care utilization and cost among health maintenance organization members with temporomandibular disorders. Journal of Orofacial Pain 15(2): 158-169.
- Fabio RP (1998) Physical therapy for patients with TMD: a descriptive study of treatment, disability, and health status. Journal of Orofacial Pain 12(2): 124-135.
- Nitzan DW, Samson B, Better H (1997) Long-term outcome of arthrocentesis for sudden-onset, persistent, severe closed lock of the temporomandibular joint. J Oral Maxillofac Surg 55(2): 151–157.
- FA Al-Belasy, MF Dolwick (2007) Arthrocentesis for the treatment of temporomandibular joint closed lock: a review article. Int J Oral Maxillofac Surg 36(9): 773–782.
- Khalid Zawawi H, (2003) An Index for the Measurement of mal Maximum Mouth Opening. Can Dent Assoc 69(11): 737–741.
- Murakami K, Kaneshita S, Kanoh C, Yamamura (2002) Ten-year outcome of nonsurgical treatment for the internal derangement of the temporomandibular joint with closed lock. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 94(5): 572–575
- R González-García, FJ Rodríguez-Campo, F Monje, J Sastre-Pérez, JL Gil- Díez Usandizaga (2008) Operative versus simple arthroscopic surgery for chronic closed lock of the temporomandibular joint: a clinical study of 344 arthroscopic procedures. Int J Oral Maxillofac Surg 37(9): 790-796.
- Michael Mezitis, George Rallis, Nicholas Zachariades (1989) The normal range of mouth opening. J Oral Maxillofac Surg 47(10): 1028–1029.
- Tùrp JC, Jockstad A, Motschall E, Schindler HJ, Windecker-Getaz I (2007) Is there a superiority of multimodal as opposed to simple therapy in patients with temporomandibular disorders? A qualitative systematic review of the literature. Clin Oral Implants Res 18(Suppl 3): 138-150.
- Hidemichi Yuasa, Kenichi Kurita (2001) Randomized clinical trial of primary treatment for temporomandibular joint disk displacement without reduction and without osseous changes: A combination of NSAIDs and mouthopening exercise versus no treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 91(6): 671–675.
- Dahlström L (1998) Diagnoses among referrals to a Swedish clinic specialized in temporomandibular disorders. Acta Odontologica Scandinavica 56(3): 143-147.
- V Ballegaard, P Thede-Schmidt-Hansen, P Svensson, R Jensen (2008) Are headache and temporomandibular disorders related? A blinded study. Cephalalgia 28(8): 832–841.
- Daniela Gonçalves AG, Marcelo Bigal E, Luciana Jales CF, Cinara Camparis M, José G (2010) Headache and Symptoms of Temporomandibular Disorder: An Epidemiological Study. Headache: The Journal of Head and Face Pain 50(2): 231–241.
- Louis Reik Jr, Mahlon Hale (1981) The Temporomandibular Joint Pain-dysfunction Syndrome: A Frequent Cause of Headache. Headache: The Journal of Head and Face Pain 21(4): 151–156.
- M Stiesch-Scholz, M Fink, H Tschernitschek (2003) Comorbidity of internal derangement of the temporomandibular joint and silent dysfunction of the cervical spine. J Oral Rehabil 30(4): 386–391.
- A De Laat, H Meuleman, A Stevens, G Verbeke (1998) Correlation between cervical spine and temporomandibular disorders. Clinical Oral Investigations 2(2): 54-57.
- Luis Buenaver F, Robert Edwards R, Michael Smith T, Sandra Gramling E, Jennifer Haythornthwaite A (2008) Catastrophizing and Pain-Coping in Young Adults: Associations With Depressive Symptoms and Headache Pain. The Journal of Pain 9(4): 311–319.
- C Gallagher, V Gallagher, H Whelton, M Cronin (2004) The normal range of mouth opening in an Irish population. J Oral Rehabil 31(2): 110–116.
- Niklas Johannink, Lena Röwekamp (2010) What is the best treatment for TMD comparing physiotherapy and other approaches? Hogeschool Van Amsterdam, Amsterdam.
- Hiroshi Kurita, Akiko Ohtsuka, Kenji Kurashina, Sigvard Kopp (2001) A study of factors for successful splint capture of anteriorly displaced temporomandibular joint disc with disc repositioning appliance. J Oral Rehabil 28(7): 651–657.





