Evolution of Dental Ceramic From The Platinum Foil to CAD-CAM Technologies: Review
Isgrò G*, Sachs A
Researcher at CAD-CAM Dental Technology Centre, Italy.
*Corresponding Author
Dr. Giuseppe Isgro,
CAD-CAM Dental Technology Centre,
Via Del Mare, 3, 98051 Barcellona
PG; (ME), Italy.
Tel: + 39 340 1880831
Fax: +39 090 979 5958
E-mail: g_isgro@tiscali.it
Article Type: Review Article
Received: April 19, 2015; Accepted: May 27, 2015; Published: June 01, 2015
Citation: Isgrò G, Sachs A (2015) Evolution of Dental Ceramic From The Platinum Foil to CAD-CAM Technologies: Review. Int J Dentistry Oral Sci. S1:003, 12-20. dx.doi.org/10.19070/2377-8075-SI01003
Copyright: Isgrò G© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
New ceramic materials and novel fabrication methods have been developed and introduced in dentistry with the aim to improve the longevity of dental ceramic restorations and to extent their use for more demanding clinical situations like construction of multi units posterior fixed partial dentures (FPDs). Dental ceramics have now reached a stage of development where it is possible to make long-span metal free posterior FPDs. Dentists and dental technicians should have knowledge of advances in dental ceramic materials and fabrication methods available to understand advantages and disadvantages of the restorative systems in order to make an optimal choice in each specific clinical situation.
2.Introduction
3.Strengthening Mechanism of Dental Ceramics
4.Internal Reinforcement of the Ceramic
5.Aluminous Porcelains
6.Glass-Ceramics
7.External Reinforcement of the Porcelain
8.Porcelain-Fused-to-Metal
9.Porcelain-Fused-to-Ceramic
10.Advances in Dental Ceramic and CAD-CAM Technologies
11.Indirect contributing factors to strength dental ceramic restoration
12.Discussion
13.Conclusion
14.References
Keywords
Crystal Phase; Glass Phase; Glass-Ceramic; Veneering Porcelain; High Strength Ceramic; Polycrystalline Ceramic; Mechanical Properties; Optical Properties.
Introduction
In 1776 ceramic material was first suggested for a dental application by the French chemist Alexis Duchateau who worked in collaboration with the dentist Dubois de Chemant to produce the first complete denture. The material used was a mixture of potash feldspar (K2O.Al2O3.6SiO2, 70-80%), quartz (SiO2, 10-30%) and kaolin (Al2O3.Si02.2H2O, 0-3%) [1]. Since then the potential of the material was understood and from an aesthetic and a hygiene standpoint ceramic could fulfill the requirements to replace lost natural teeth. Thus, Duchateau’s work gave stimulus to others to continue the development of ceramic with new chemical composition and novel fabrication methods, to produce dental restorations that have translucency, and colour close to natural teeth.
Charles H. Land of Detroit introduced in 1889 the first dental ceramic restoration for a prepared tooth [2]. The ceramic employed was a high fusing feldspathic material (1050°C–1200°C) containing 15 vol.% of crystalline quartz that was condensed over a platinum foil, adapted directly on the prepared natural tooth [2]. Despite its aesthetic advantage due to a high content of feldspathic glass, which provided a translucent restoration [3], the material was extremely brittle (flexural strength 60 MPa) [4] causing fracture during service [5]. At this point, the main disadvantage of the ceramic was the relatively low strength, which limited the use.
Gradually dental ceramics have become popular due to the improvements in strength, and in recent years they have been used in a wide variety of clinical applications. Dental ceramic restorations could be fabricated with a single layer of ceramic or with multi-layers that are composed of ceramic coping and veneering porcelains. Therefore, dentists and dental technicians have a range of ceramic restorative systems that are comprised of specially formulated materials and expensive equipment for the fabrication of a restoration (Table 1).
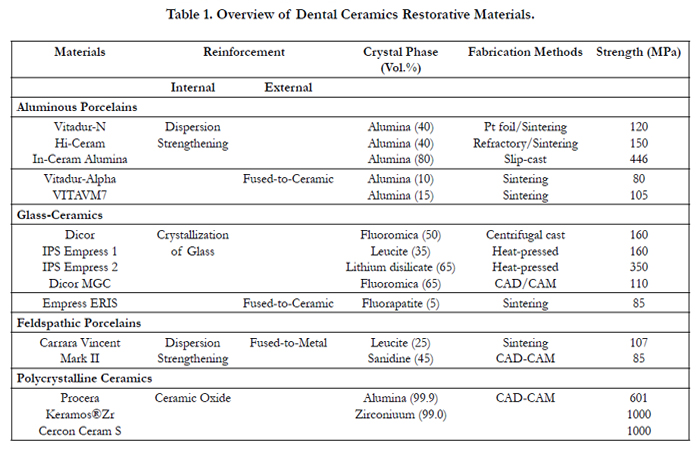

Table 1. Overview of Dental Ceramics Restorative Materials.
Unfortunately, the contemporary dental ceramic restorative systems are not indicated for every clinical application due to their difference in material properties, such as opacity, translucency, strength and toughness of the materials. Thus, the clinician should select an appropriate type of ceramic material for each specific clinical demand, for example high aesthetic quality or strength. Therefore, it is important to understand the mechanical and optical properties, the application and limitations of ceramic materials because this will guide the dentist during the selection, as well as enhancing an effective communication and collaboration with the dental laboratory. In addition, the manufacturing of ceramic dental restorations requires skilled dental technicians with knowledge of ceramic materials and fabrication methods. For this, scientific information on the strengthening mechanisms of ceramic materials and fabrication methods associated with the dental restoration are necessary. Furthermore, the fracture resistance and clinical performance of dental ceramic have improved owing to the design of the restoration, tooth preparation and adhesive cements. These contributing factors are also outlined.
Strengthening Mechanism of Dental Ceramics
Dental ceramics have a chemical composite that contains a high content of feldspathic glass and crystalline phase [2]. The high proportion of glassy phase allows the transmission of the light providing the translucency necessary to produce an aesthetic restoration [6] but it imparts to the material the brittle propriety of glass [7]. The strength of the ceramic depends on surface defects like cracks and micro porosities [8, 9] or on internal voids (Figure 1) [1]. The deformation of the ceramic by the application of external tensile stresses initiates the propagation of cracks (Figure 1b), resulting in the fracture of the material [10]. Considerable research has emphasized enhancing the strength characteristics of dental ceramics and several directions are recognized. One method is to strengthen the glassy ceramic by adding a second crystalline phase. The internal reinforcement of the ceramic is achieved by the dispersion of crystals in the glass matrix (i.e. dispersion strengthening) or by the crystallization of the glass. With these methods new ceramic materials have been developed that have translucent, semi-translucent, semi-opaque and opaque optical proprieties [11] (Figure 2a). Translucent and semi-translucent ceramic materials are used to fabricate single layer restoration while semi-opaque and opaque ceramic materials are employed as external reinforcement of the glassy porcelain material, producing multiple-layered dental ceramic restorations. Another method to reinforce the porcelain is to bond it onto a metal [12] known as porcelain fused to metal (PFM) dental restorations. The improvements in strength of the dental ceramics have been also accomplished by the introduction in dentistry of novel fabrication methods (i.e. heat press and computer aided design, computer aided milling) that produces materials with a homogeneous microstructure thereby reducing internal defects (Figure 1a).
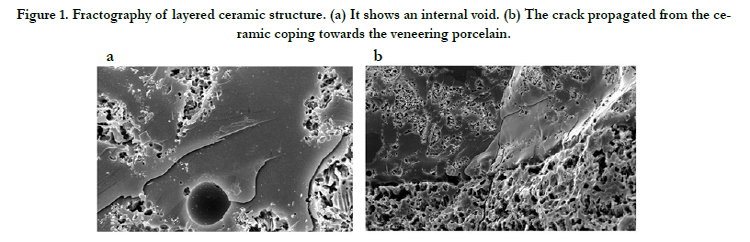
Figure 1. Fractography of layered ceramic structure. (a) It shows an internal void. (b) The crack propagated from the ceramic coping towards the veneering porcelain.
Internal Reinforcement of the Ceramic
All ceramics are brittle materials, some compositions more than others. Approximately 0.1% deformation of any ceramic may result in fracture [13]. A fundamental method to improve the strength and toughness of ceramics is to increase its rigidity (elastic modulus) [14] by introducing in the glass matrix of the material a proportion of crystals that have high strength and elasticity [12, 14, 15]. The crystals within the glass matrix impede the propagation of cracks through the bulk of the material when under tensile stress, increasing therefore the strength of the ceramic [16]. The strength of the ceramic material depends also on the amount and particle size of the crystalline phase [16]. Binns (1962) [15] and Jones et al., (1972) [13] demonstrated that both strength and modulus of elasticity of the ceramic progressively increases with the proportion of crystalline phase with a particle size smaller than 5μm. Based on this concept two categories of ceramic materials, aluminous porcelains and glass- ceramics, have been developed for the construction of dental restorations. However, an important feature distinguishes aluminous porcelains from glassceramics. For the aluminous porcelains most of the crystalline phase is introduced when the composition of the material is prepared (i.e. dispersion strengthening), while in the glass-ceramic the crystalline phase is the product of the crystallization of the glass [17].
Aluminous Porcelains
The dispersion strengthening method, which represents one of the most important development in dental ceramics [18], was first introduced in dentistry by McLean and Hughes in the 1960’s to produce aluminous porcelain [19]. The system consisted of opaque aluminous porcelain coping, which could be built up by hand with a brush, and condensed over a platinum foil and sintered at the temperature of 1050°C. The porcelain material was strengthened by a dispersion of aluminum oxide crystals (Al2O3), into a feldspathic glass. The microstructure consisted of 40 vol.% of alumina, which increased the flexural strength of the material up to 120 MPa but it decreased the transmission of the light resulting in poor translucency of the dental restoration [5, 14] (Figure 2). Thus, the coping was veneered with layers of weaker (i.e. 80 MPa) feldspathic porcelains (VitaDur N, Vita Zahnfabrik, Bad Säckingen, Germany) (Table 1) with better optical properties and fired at a lower temperature. However, the macrostructure of the dental ceramic restoration was affected by flaws and voids (Figure 1a) as a result of poor adaptation and wetting of the porcelain slurry on the platinum foil [20, 21]. In order to minimize defects in the microstructure and to improve the strength of the dental restoration, a new aluminous porcelain was subsequently developed and introduced under the name of Hi-Ceram (Vita Zahnfabrik, Bad Säckingen Germany). The aluminous porcelain slurry was condensed and sintered on a refractory die and it showed a flexural strength of 150 MPa [22]. Still, the disadvantages of both aluminous porcelain materials remained that the strength was inadequate to restore posterior teeth [4] and the dental restoration had a dull appearance.
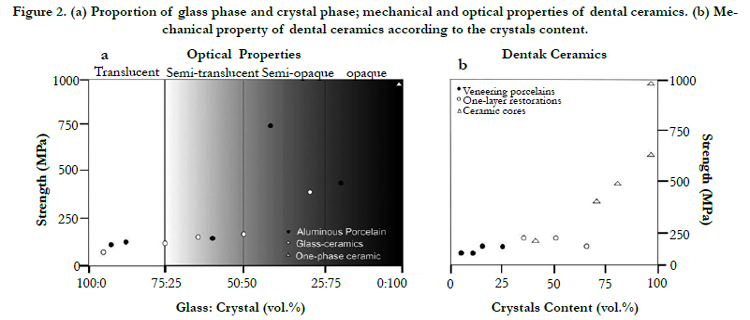
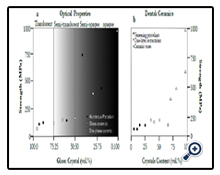
Figure 2. (a) Proportion of glass phase and crystal phase; mechanical and optical properties of dental ceramics. (b) Mechanical property of dental ceramics according to the crystals content.
Glass-Ceramics
Glass-ceramics materials are the result of a controlled crystallization of glass [9] by which a second crystal phase, to reinforce the glass, is produced. The crystallization process is achieved by subjecting the glass to a careful heat treatment which results in the nucleation, and growth of crystals within the glass [17, 23]. The conversion process from glass to ceramic is called ceramming [5,24] and involves a two-stage heat treatment. The first stage allows the formation of nuclei by means of nucleating agents that were melted into the glass. After a required period of time, the temperature is raised to cause crystal growth. The crystallization process produces glass-ceramic with a macrostructure that consists of a residual glass matrix with fine randomly oriented crystals and without voids, micro-cracks or other porosity [23] (Figure 3). This feature imparts to the material much higher strength than the original glass. The first glass-ceramic was introduced in dentistry by MacCulloch in 1968 to produce posterior teeth for dentures. The glass-ceramic system was based on lithium, zinc oxide and silica (Li2O.ZnO.SiO2) and metal phosphates were used as nucleating agents [25]. At that time, MacCulloch suggested that glass-ceramics could be used for producing full anatomy crowns, inlays and veneers by casting molten glass.
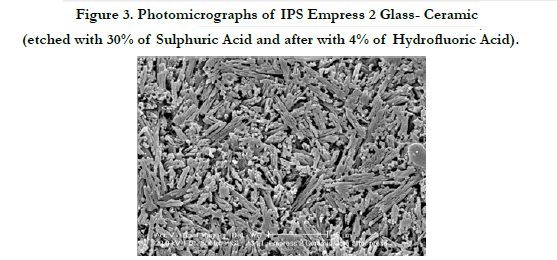
Figure 3. Photomicrographs of IPS Empress 2 Glass- Ceramic (etched with 30% of Sulphuric Acid and after with 4% of Hydrofluoric Acid).
Based on this principle in 1984 a new glass-ceramic was introduced under the trade name of Dicor (Dentsply Inc., York, Pa) for the production of dental ceramic restorations [26]. Its composition was primarily magnesium aluminosilicate glass with 50 vol.% of fluoromica crystals (K2 Mg5 Si8 O20 F4) [27]. It represents the first technique to process dental ceramic that used the lost-wax and casting techniques, at that time already extensively used in the dental laboratory for the construction of PFM dental restorations. The glass was first centrifugally cast at temperatures of 1370°C into a phosphate- based refractory mould. After the glass restoration was re-embedded in an investment material and converted by means of a secondary heat treatment of six hours at the temperature of 1075°C into a ceramic [28, 29]. The completion of the restoration required the application to go through firing cycles of thin layers (50-100μm ) of colorant glass to mimic the natural tooth colour [27]. Clearly, this represented an aesthetic limitation because of the surface colour. An alternative technique was to cut back the full ceramic crown and veneered it with a feldspathic enamel porcelain layer (Dicor Plus, Willi’s Glass) to provide depth translucency effect [4]. The disadvantages of the Dicor system were ceramic shrinkage due to the casting followed by the ceramic procedure [24], the time required for the fabrication of the restoration and that the material was provided as a single milky white translucent shade [27].
To overcome these difficulties a new glass-ceramic was developed at the University of Zurich in collaboration with a dental company (Ivoclar-Vivadent, Schaan, Liechtenstein) and introduced in the market under the trade name of IPS Empress. This system was supplied in pre-cerammed cylinders of various shades that contained 35 vol.% of leucite (K2O-Al2O3-4SiO2) crystals measuring between 1 to 5 μm dispersed in glass matrix [30]. The manufacture of dental ceramic restorations with the IPS Empress system was similar to the Dicor system except that the glass-ceramic was processed by means of a heat-pressing technique. First the glass-ceramic was softened at 1150ºC inside the channel provided by the design of the refractory mould. Then, the ceramic was pressed into the mould at 5 bar air-pressure by means of a special designed furnace [31]. This pressing process eliminated the shrinkage of the ceramic material resulting in a good fit of the restoration [4, 5, 30] and in a better distribution of the crystalline phase within the glass matrix [31, 32] (Figure 3).
The developed glass-ceramic materials exhibited a flexural strength in the range of 160 MPa [28, 33], which value was comparable to those of the early aluminous porcelains [19, 22], but the glass- ceramic materials improved the aesthetics of the dental ceramic restoration. Therefore, they were best suited to fabricate single layer full crown, inlay, onlay and veneer dental restorations [26, 31]. Further improvement of the dental glass-ceramic was the development of a strong material thus expanding its application for more demanding clinical situations.
External Reinforcement of the Porcelain
Substrates like metal and high strength ceramic materials are often used to reinforce the weak feldspathic veneering porcelains that have a strength of 80 MPa [34, 35], applied to reproduce the morphology and aesthetic of natural teeth. As a result, multiplelayered restoration shows an improved clinical performance such as longevity (i.e. PFM) or aesthetic and biocompatibility (i.e. porcelain fused to ceramic coping) compared to single layer dental ceramic restorations (i.e. full crown, inlay, onlay).
Porcelain-Fused-to-Metal
Porcelain-fused-to-metal system was introduced as a restorative material in 1962 when Weinstein et al., (1962) [36] developed a thermally compatible feldspathic porcelain that was fused onto a gold coping. It is still widely used today. The composition of the porcelain designed for metal is essentially feldspathic glass that contains about 18 vol.% of leucite (K2O-Al2O3-4SiO2) crystals [29] (Table 1). Leucite is a mineral with a thermal expansion in the range of 17 to 20 ppm/°C that raises the low thermal expansion of feldspathic glasses that is in the range of 6 to 10 ppm/°C in order to match the thermal expansion of the metal (i.e.14 ppm/°C) [29]. The thermal compatibility in the PFM system reduces the risk of cracking on cooling of the veneering material during fabrication [37]. In addition to this, the metals coping, at the fit surface of the restoration can withstand the tensile stress produced by occlusal force owing to their ductile behaviour. Metals have yield strengths (YS) ranging from 450 to 862 MPa [7] which means that stress below these values does not cause permanent deformation. Furthermore, cracks that propagate from the surface of the veneering porcelain are stopped by the underlying metal coping preventing the fracture in two halves of the restoration. Presently PFM are the most clinically successful system that provides porcelain restoration with high reliability. Therefore, they are indicated in the construction of long-span FPDs to be used in areas of high stress. On the other hand, the PFM system presents several disadvantages. Firstly, there is a potential of alloy corrosion leading to toxicity and allergy [38]. Secondly, the restoration requires, for depth translucency effect, substantial tooth reduction in order to provide enough space for metal coping, opaque, dentine and enamel porcelains [4]. If there is little room for the translucent porcelains, the light is reflected from the opaque porcelain that is necessary to mask the metal coping and the dental restoration appears too bright.
Porcelain-Fused-to-Ceramic
The increasing demand for restorative materials with improved aesthetics, strength and biocompatibility have brought about the development of high strength ceramics substrates as substitute for the metal framework. The concept of this type of high strength ceramic came with the extensive use of crystals to strengthen the glass. The materials in this method contain more than 50 vol.% concentrations of crystals in the glass matrix (Figures 2 and 3). Although the higher content of crystalline phase makes ceramic coping an opaque material, still it has better aesthetic properties compared to PFM. This is due to the residual glass matrix and the nature of the crystals, which provide the materials with a certain amount of translucency [23, 39].
The first high strength ceramic material for dental restoration was developed by Sadoun [40] in 1980’s and marketed under the tradename of In-Ceram (Vita Zahnfabrik, Bad Säckingen, Germany). The ceramic material consisted of 80 vol.% of alumina crystals dispersed in a lanthanum aluminosilicate glass matrix [41] (Figure 4). The framework was shaped by a unique procedure known as slip-cast technique. The slip, which is a dispersion of alumina particles ranging in size from 1 to 5 μm [37] in water, was applied with a brush onto a gypsum refractory die. The water from the slip, was absorbed by the porous mould and then the framework was sintered in a furnace for 4 hours at 1100°C. The porous alumina was subsequently infused with a low-viscosity sodium lanthanum glass and fired at 1150°C for 4 hours [29]. The higher concentrations of alumina in combination with the slip-cast processing provided the dental ceramic restoration with an outstanding mechanical property. The flexural strength of the In-Ceram dental ceramic has been reported to be 446 MPa [42], which is four times greater than the earlier conventional aluminous porcelains. Therefore, the In-Ceram system was the first dental ceramic indicated for the production of posterior crowns and anterior FPDs. The disadvantages of this system were extensive tooth reduction to produce an aesthetic restoration, the time needed for the manufacture of the ceramic framework and the need for special equipment [4].
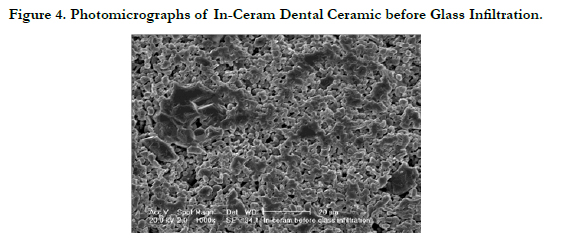
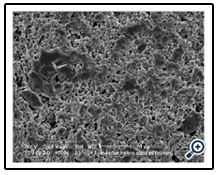
Figure 4. Photomicrographs of In-Ceram Dental Ceramic before Glass Infiltration.
In the 1990’s another high strength glass-ceramic material for the production of multi-layered dental ceramic restorations was introduced and marketed under the trade name of IPS Empress 2 (Ivoclar- Vivadent, Schaan, Liechtenstein). The main crystalline phase of the ceramic material consists of 65 vol.% of elongated and randomly oriented lithium disilicate (Li2Si2O5) crystals (Figure 3) measuring between 0.5 to 5 μm in length [30]. The microstructure also contains a second crystalline phase made of 5 vol.% of lithium orthophosphate (Li3PO4) crystals measuring approximately 0.1 to 0.3 μm [5, 30]. The fabrication of the restoration involves first the production of the framework, by means of the lost-wax technique in combination with a heat-pressing method. Then, the ceramic framework is veneered with a glass-ceramic consisting of fluorapatite crystals dispersed in aluminosilicate glass matrix [30] (Table 1) to reproduce the final morphology and color of the natural tooth. The measured flexural strength of the ceramic material is 350 MPa [43] and therefore, it is recommended for the production of single anterior and posterior crowns and three-unit anterior FPDs. A new marketed high strength dental ceramic system is IPS e.max Press. The microstructure, mechanical proprieties and application are the same as those of IPS Empress 2.
Advances in Dental Ceramic and CAD-CAM Technologies
In recent years computer-aided-design (CAD) and computer-aided- milling (CAM) technologies have been introduced in dentistry as new methods to manufacture dental ceramic restorations either in the dental practice (referred to as the chair side concept) or in a milling centre [30, 44, 45]. CAD-CAM technologies require three functional steps [44, 46]. Firstly, the acquisition of digital data either from the prepared teeth of the oral cavity or it is recorded from a model cast. Secondly, the restoration design is proposed by the CAD software taking into account all functional aspects.
Thirdly, the shape of the restoration is produced from a prefabricated block of ceramics by subtractive manufacturing process [47] using the CAM software and a computer numerical control (CNC) milling machine.
Several dental ceramic systems that embrace the concept of CAD-CAM technologies have been introduced but they differentiate in chemical composition of the material used [44]. Marketed systems like Cerec 3 and Cerec inLab (Sirona, Bensheim, Germany) are CAD-CAM systems that process a number of machinable ceramics which evolved from existing dental ceramics [27] for the manufacturing of dental ceramic restorations. The Cerec 3 system, processes a feldspathic porcelain (Vitablocks Mark II, Vita Zahnfabrik, G) which contains 45 vol% of sanidine as the major crystalline phase [42, 48] with a flexural strength of 85 MPa [42]; and two glass-ceramics, one has leucite as crystalline phase (ProCAD, Ivoclar-Vivadent Schaan, L) and the other contains 65 vol.% of mica crystals (Dicor MGC, Dentsply Inc., York, Pa) [49] with a flexural strength of 110 MPa [27, 30, 42, 45]. The advantage of this system is that it allows inlays, onlays, veneers or full crowns to be fabricated and cemented in a single visit of the patient. The Cerec inLab system processes blocks of aluminous porcelain (In-Ceram, Vita Zahnfabrik, Germany) that are pre-sintered by the manufacturer, to fabricate three unit bridges. After the framework is milled, it is infiltrated with lanthanum glass and fired for 40 minutes. This represents an advantage over the slip-cast technique where 4 hours for the infiltration are required [27, 45]. The framework is then veneered with porcelain in a conventional manner in the dental laboratory.
The introduction of the CAD-CAM technologies has opened the way to new advanced ceramics such as high-purity powder alumina (99.9% Al2O3) [50, 51] and yttria-stabilized tetragonal zirconium polycrystalline (Y-TZP) [52, 53] ceramic materials (Figures 2 and 5).
The Procera dental ceramic (Nobel Biocare, Göteborg, Sweden) system manufactures single ceramic coping made of 99.9% alumina powder [51]. First the image of the tooth preparation is obtained by scanning the plaster die. Then the image is enlarged by the CAD software by 20% to compensate for the volumetric shrinkage of alumina powder during sintering [51]. Next, the milling machine directed by the CAM software produces the refractory die on which the alumina powder is manually applied [44]. Then, the outer surface of the ceramic in the green body is milled and the coping is densely sintered with a dry pressing technique and fired at the temperature of 2050ºC. The final product consists of a dense crystalline structure with an average grain size of 4 μm and a flexural strength of 601 MPa [51]. The coping is returned to the dental laboratory for the application of the veneering porcelains. The Procera system is employed only in the fabrication of single crowns placed in the anterior and posterior region of the mouth [51].
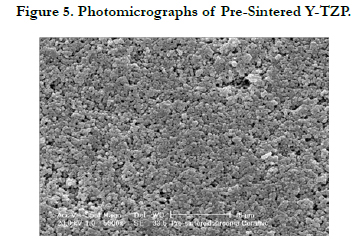
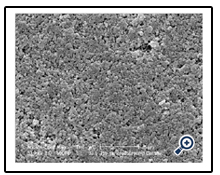
Figure 5. Photomicrographs of Pre-Sintered Y-TZP.
The Y-TZP has better mechanical and optical properties than alumina [52] and it can be used for the fabrication of the framework, for anterior and posterior bridges and full crown dental ceramic restorations. The notable mechanical properties such as strength and toughness of Y-TZP come from a transformation phase termed “transformation toughening”[54]. The strength mechanism of the Y-TZP depends on the addition of approximately 2-3% mol of yttrium oxide (Y2O3) into the material. As a result, the zirconium particles retain at room temperature a no-equilibrium or metastable tetragonal (TZP) phase [53-55]. The presence of cracks introduced by the manufacturing process [56] causes the metastability of the zirconium particles to convert into the stable monoclinic phase. The transformation phase which depends on the particle size and quantity of Y 2O3 [53-57] increases the volume of the particles by 4%, thereby inducing compressive stress on the crack tip inhibiting the propagation of crack and increasing the resistance of the material to fracture [54]. The flexural strength of the sintered Y-TZP has been reported to be between 914 to 1021 MPa [56, 57], which is far higher than all the ceramic systems used in dentistry before.
Currently two commercially available dental ceramic systems such as KeramosZr® produced by CAD-CAM Dental Technology Center® (Barcellona PG, Me, Italy) and Cercon Smart Ceramics (DeguDent GmbH, Hanau, Germany), utilize Y-TZP ceramic to manufacture underlying ceramic frameworks and full anatomy crown. However, these two dental ceramic systems use different CAD- CAM technologies to process the partially sintered Y-TZP blank. KeramosZr® system is considered to be a true CAD-CAM system because the dental ceramic restoration is digital designed by the software, while in the Cercon system the framework is made first in wax by the dental technician and after the wax it is scanned. In both systems the image is enlarged by 20% by the CAM software to compensate for the dimensional change of the Y-TZP material during the sintering process [56]. Due to the high strength of the Y-TZP, the milling in the pre sintered condition represents an advantage in terms of time and it does not require the use of expensive diamond tools because the green blank has the consistency of chalk. Then in both systems the milled dental restoration in the green body is sintered at the temperature of 1400ºC to transform the material into ceramic [53].
Indirect contributing factors to strength dental ceramic restoration
The thickness ratio of ceramic coping and veneering porcelain combined with the geometry of the crown and bridge frameworks determine the strength of the whole dental ceramic restoration [59, 60]. Although ceramic materials with high flexural strength and high elastic modulus have been developed, dental technicians tend to use these proprieties to produce a thinner coping in order to make more space for the aesthetic veneering porcelain. As a consequence, the ceramic coping will deform [10] during functional load due to the decrease of its stiffness, reaching easily the critical strain of 0.1%. Wakabayashi and Anusavice [61] showed that the fracture resistance of the dental ceramic restoration depends on the rigidity of the whole structure, which can be achieved by increasing the thickness of the ceramic coping with a thinner veneering porcelain layer. In the case of FPDs the dimensions of the connectors which connect the copings to the pontic are important for the longevity of the restoration. It has been shown from fractographic analysis [61] that failure of FPDs tends to occur at the connectors where cracks initiate and propagate towards the pontic, which is the area of loading. Tooth preparation also is a factor in the failure of dental ceramics as the design of the restoration depends on the shape of the preparation. A smooth preparation of the tooth gives adequate support to the crown by providing uniform ceramic thickness and accuracy of the fit [11]. Routinely, tooth reduction should be between 1.5-2.0 mm in the incisal or occlusal surfaces, while on the labial and lingual side the reduction should be between 1.0-1.5 mm [28]s. The design of the tooth preparation should also include a shoulder that has a width of at least 1 mm for the whole circumference of the tooth. It is also important to smooth and round the angels of the preparation to reduce the stress concentration [11] on the inner surface of the dental ceramic restoration.
The fracture resistance of a dental ceramic restoration may be improved by the adhesion to the underlying tooth structure [5]. Different adhesive luting systems such as glass ionomer-based or resin composite-based cements, are available to lute a restoration [62]. However, for some dental ceramic systems in which the materials contain a portion of glass, only resin-based cement is recommended to lute the restoration. Horn (1983) [63] has developed method which combines mechanical and chemical bonding in order to increase the adhesion between the porcelain and tooth structure. This new adhesive technique provides mechanical retention for the resin-based cement by etching the fit surface of the ceramic restoration with hydrofluoric acid owing to its ability to remove the glass phase [64] of the ceramics thus creating surface irregularities [5, 62]. Mechanical retention can also be produced on the tooth structure by etching the dentin with phosphoric acid [5, 62]. The chemical bonding is provided with a silane coupling agent (i.e. dentin adhesive) and then the restoration is cemented. In addition, resin-based cement has the potential to increase the fracture resistance of a dental ceramic restoration [5, 37, 65, 66]. Isgró et al., (2010) [66] demonstrated using the deflection test that the polymerisation shrinkage of resin-based cement induces a beneficial compressive stress state across the glass-ceramic discs tested. This finding accounts for the improved clinical performance of adhesively cemented dental ceramics restorations. Unfortunately, this adhesive technique cannot be applied to alumina or zirconium polycrystalline ceramics, because it is impossible to etch the materials with hydrofluoric acid or to treat them with a silane coupling agent [65] as there is no glass phase in the macrostructure (Figure 5).
Discussion
Ceramics are used in restorative dentistry because they are biocompatible and they have high aesthetic qualities. Their selection for restoring missing teeth depends on the needed strength and desired level of aesthetics, the amount of tooth structure that can be preserved and the available laboratory support. Two elements are important for the success of a dental ceramic restoration: 1 advances in the chemical composition leading to more strength but less aesthetic; 2. advance in fabrication methods. This review of the developments of dental ceramics shows that major improvements of the mechanical properties of ceramics have so far only been achieved by changing the chemical composition of the material. Crystals have been added to the chemical composition of the ceramics, up to a level where the glass matrix (Figure 6) has been completely replaced as in polycrystalline ceramics such as Y-TZP (Figure 5).
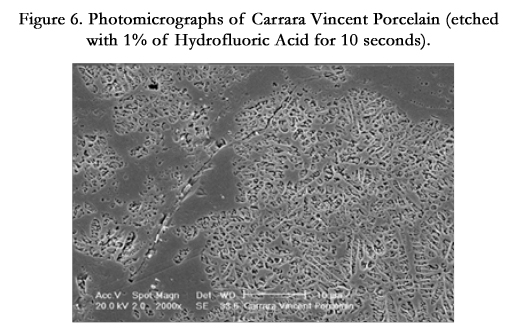
Figure 6. Photomicrographs of Carrara Vincent Porcelain (etched with 1% of Hydrofluoric Acid for 10 seconds).
Although crystallised ceramics have a high strength, the absence of residual glass does not allow the transmission of the light, affecting therefore the translucency of the material [68]. This represents a serious limitation for use when an aesthetic dental ceramic restoration is required. An alternative method to improve the optical properties of a dental ceramic restoration is to fuse a translucent porcelain material, (i.e. high glass content) onto an opaque ceramic coping (i.e. high crystals content). This design combines aesthetics with mechanical strength. However, it is not clear whether the strength of the multiple-layered structure is improved sufficiently to be able to with stand to the functional forces in the oral environment thus extending the longevity of the dental ceramic restoration. Several causes, such as thermal incompatibility of the components materials, might affect the dental ceramic restoration owing to the residual thermal stresses. Isgró and co-authors [69] used the deflection test to visualize stressinduced deformation in layered dental ceramics. The maximum mean deflection of the layered ceramic discs occurred with the largest mismatch in thermal contraction values of the ceramic and veneering porcelain [69]. A distorted multi-layer dental ceramic could affect the strength and the fit of the restoration and lead to its premature failure. In addition, stress distributions and therefore failure behaviour, can be quite different in multiple-layered ceramics structure, with materials having different elastic properties, than in a monolithic structure.
Specific fabrication methods have been combined with new dental ceramic materials, producing restoration with less defects. For instance, for the construction of a dental restoration use of heat pressed glass-ceramics offers several advantages over the use of traditional aluminous porcelains and their sintering method. In the traditional method, in which the ceramic powder is mixed with the liquid binder and condensate, the ceramic in green state shrinks during sintering, resulting in warping and distortion of the dental restoration [10] and correction firings are necessary. The pressing technique produces a dental ceramic restoration with the final shape and produces it with a homogeneous microstructure, free of defects (Figure 3) that can occur during the condensation process [2, 10, 29] (Figure 1a). However, a good result of a heatpressed ceramic depends on the viscous flow characteristic of the glass matrix and its dependence on temperature [10].
Also CAD-CAM technology offers some important advantages. It eliminates error sources that might arise from indirect procedures such as wax-up and investment expansion. In addition, the Y-TZP blanks, supplied in a partially or fully sintered state, are industrially pre-fabricated by the manufacturer to be pore-free [27] (Figure 5). After the milling procedure, the Y-TZP restoration in green state is sintered in one firing. This eliminates macrostructural change which can occur during the build-up of ceramic layers during repeating firing procedures. It has been observed that leucite ceramic undergoes microstructural and thermal expansion changes due to additional crystallization of the glass as a result of repeating firing [70, 71].
Although many advances in dental ceramics have been reached, research for an ideal material continues to be the central issue. The search for a dental ceramic material with the required aesthetics and the strength for restoring continuing missing teeth in the posterior region of the mouth is not over yet.
Conclusion
In restorative dentistry, ceramic is a biocompatible and aesthetic material but its use was in the past restricted to restore posterior continuing missing teeth. However, several advances in dental ceramics concerns the composition, have created improved ceramic materials which have made them indicated for the fabrication of free-metal restorations to restore continuing missing teeth in both the anterior and posterior region of the mouth. The developments have been, to the introduction of high strength ceramics, for the fabrication of one-layer restorations, and the fabrication multiple-layered restoration made of ceramic coping to support aesthetic porcelain. Another development has been the introduction of novel fabrication methods of dental ceramic restorations. These developments have increased the longevity of dental ceramic restorations while maintaining acceptable aesthetic standards. As a result, the dentist can now meet the demands of patients when an aesthetic and biocompatible restoration combined with strength is required.
References
- Binns D (1983) The chemical and physical properties of dental porcelain. In: McLean, J.W. editor. Dental ceramics. Proceedings of the first international symposium. Chicago: Quintessence Publishing Co. Inc. 41-82.
- McLean JW (1979) The science and art of dental ceramics. Vol. I: The nature of dental ceramics and their clinical use. Quintessence, Chicago. 19-21-69.
- McLean JW (1980) The science and art of dental ceramics. Vol. II: Bridge design and laboratory procedures in dental ceramics. Quintessence, Chicago 28.
- Wall JG, Cipra JG (1992) Alternative Crown Systems. Dent Clin North Am 36(3): 765-782.
- Van Noort R (2002) An introduction to dental materials. Mosby Published. 231-246.
- Southan DE (1983) The porcelain jacket crown. In: McLean JW editor Dental ceramics. Proceedings of the first international symposium. Chicago: Quintessence Publishing Co. Inc. 207-230.
- O’Brien WJ (1997) Dental materials and their selection. (2nd edn). Quintessence Publishing Co, Inc. USA. 180-289.
- Kelly JR, Giordano R, Pober R, Cima MJ (1990) Fracture surface analysis of dental ceramics. Int J Prosthodont 3(5): 430-440.
- Anusavice KJ (1996) Phillips’s science of dental materials. (10th edn) ,WB Saunders Company, Philadelphia. 583-618.
- Kingery WD, Bowen HK , Uhlmann DR (1976) Introduction to Ceramics. (2nd edn), John Wiley & Sons ,USA. 787.
- McLean JW, Jeansonne EE, Chiche G, Pinault A (1994) All-ceramic crowns and foil crowns. In: Esthetics of anterior fixed prosthodontics. Chiche, G and Pinault A (Eds) Chicago Quintessence. 97-113.
- O’Brien WJ (2000) Strengthening mechanisms of current dental porcelains. Compendium 8: 625-630.
- Jones DW ,Jones PA, Wilson HJ (1972) The modulus of elasticity of dental ceramics. Dent Practit 22: 170-173.
- McLean JW, Kedge MI (1987) High-strength ceramics. Quintessence Inter 2: 97-106.
- Binns DB (1962). Some physical properties of two-phase crystal-glass solids. In: Science of ceramics. Vol. 1. Stewart GH, editor. London: Academic Press. 315-334.
- Jones DW (1983) The strength and strengthening mechanism of dental ceramics.In: McLean JW editor. Dental ceramics. Proceedings of the first international symposium. Chicago: Quintessence Publishing Co. Inc. 83-136.
- McMillan PW (1979) Glass-Ceramics. (2nd edn), England Academic press. 1(5); 222-232.
- Jones DW (1985) Development of dental ceramics. Dent Clin North Am 4: 621-644.
- McLean JW ,Hughes TH (1965) The reinforcement of dental porcelain with ceramic oxides. Brit Dent J 21: 251-267.
- Southan DE, Jørgensen KD (1972) Faulty porcelain jacket crowns. Austral D J 6: 436-40.
- Southan DE, Jørgensen KD (1973) Faulty porcelain jacket crowns. Austral D J 18:152-156.
- Rizkalla AS , Jones DW (2004) Mechanical properties of commercial high strength ceramic core. Dent Mater 20: 207-212.
- Beall GH (1992) Design and properties of glass-ceramic. Annu Rev Mater Sci 22: 91-119.
- Schärer P ,Sato T ,Wohlwend A (1988) A comparison of the marginal fit of three cast ceramic crown system. J Prosthet Dent 59: 534-542.
- MacCulloch WT (1968) Advances in dental ceramics. Br Dent J 361-365.
- Grossman DG (1985) Cast glass ceramics. Dent Clin North Am 4: 725-739.
- Kelly JR, Nishimura I, Campbell SD (1996) Ceramics in dentistry: Historical roots and current perspectives. J Prosthet Dent 75: 18-32.
- Adair PJ Grossman DG (1984) The castable ceramic crown. Int J Periodont Rest Dent 4:32-45.
- Denry IL (1996) Recent advances in ceramics for dentistry. Crit Rev Oral Biol Med 7: 134-43.
- Albers HF (1999) Ceramic materials. Adept Report. 1-20.
- Dong JK, Luthy H ,Wohlwend A, Shärer P (1992) Heat-pressed ceramics: Technology and strength. Int J Prosthodont 5: 9-16.
- Drummond JL, King TJ ,Bapana MS ,Koperski RD (2000) Mechanical property evaluation of pressable restorative ceramics. Dent Mater 3: 226-233.
- Uctasli S ,Wilson HJ, Unterbrink G , Zaimoglu A (1996) The strength of a heat-pressed all-ceramic restorative material. J Oral Rehabil 4: 257-261.
- Sherrill CA O’Brien WJ (1974) Transverse strength of aluminous and feldspathic porcelain. J Dent Res 3: 683-690.
- Campbell SD (1989) A comparative strength study of metal ceramic and all-ceramic esthetic materials: Modulus of rupture. J Prosthet Dent 62: 476-479.
- Weinstein M, Katz S ,Weinstein (1962) A Fused porcelain-to-metal teeth. US patent no 3.052.982.
- McLean JW (2001) Evolution of dental ceramics in the twentieth century. JProsthet Dent 85: 61-66.
- Hondrum SO (1992) A review of the strength properties of dental ceramics. J Prosthet Dent 67:859-65.
- Giordano R (2002) A comparison of all-ceramic restorative systems. J Massachusetts Dent Soc 4: 16-20.
- Sadoun M (1989) Slip cast alumina ceramics. International conference on Dental ceramics; Leeds Castl, England.
- Kelly JR (1997) Ceramics in restorative and prosthetic dentistry. Annu Rev Mater Sci 27: 443-468.
- Seghi RR ,Sorensen JA (1995) Relative flexural strength of six new ceramic materials. Int J Prosthodont 8: 239-246.
- Sorensen JA, Mito WT, Chamberlan TH (1999) Core ceramic flexural strength from water storage and reduced thickness. J Dent Res 78.
- Mehl A, Hickel R (1999) Current state of development and perspectives of machine-based production methods for dental restorations. Int J Comput Dent 2: 9-35.
- Fasbinder DJ (2003) CAD/CAM ceramic restorations in the operatory and laboratory. Compendium 8: 595-604.
- Rekow ED (1993) High-technology innovations-and limitation-for restorative dentistry. Dent Clin North Am 3: 513-524.
- Besimo CE, Spielmann HP, Rohner HP (2001) Computer-assisted generation of all-ceramic crowns and fixed partial dentures. Int J Comput Dent 4: 243-262.
- Denry IL, Hollaway JA, Tarr LA (1999) Effect of heat treatment on microcrack healing behaviour of a machinable dental ceramic. J Biomed Mater Res 48: 791-796.
- Thompson JY, Bayne SC, Heymann HO (1996) Mechanical properties of a new mica-based machinable glass ceramic for CAD/CAM restorations. J Prosthet Dent 76: 619-623.
- Andersson M ,Bergma BO ,Bessing C ,Gunnel E ,Lundquist P, et al. (1989) Clinical results with titanium crowns fabricated with machine duplication and spark erosion. ACTA Odntol Scand 47: 279-286.
- Andersson M, Odén A (1993) A new all-ceramic crown. A dense-sintered, high-purity alumina coping with porcelain. ACTA Odontol Scand 51: 59-64.
- Giordano R (2000) A comparison of all-ceramic restorative systems: Part 2. Gen Dent 48: 38-40.
- Luthardt RG, Holzhüter M ,Sandkuhl O ,Herold V ,Walter M (2002) Reliability and properties of ground Y-TZP-zirconia ceramics. J Dent Res 7:487-491.
- Piconi C ,Maccauro G (1999) Review. Zirconia as a ceramic biomaterial. Biomaterials 20: 1-25.
- Callister WD (1997) Materials science and engineering. An introduction. (4th edn) John Wiley& Sons, USA. 533.
- Kosmač T ,Oblak C, Jevnikar P, Funduk N, Marion L (1999) The effect of surface grinding and sandblasting on flexural strength and reliability of YTZP zirconia ceramic. Dent Mater 15: 426-433.
- Guazzato M, Albakry M ,Ringer SP, Swain MV (2004) Strength, fracture toughness and microstructure of a selection of all-ceramic materials. Part II Zirconia-based dental ceramics. Dent Mater 5: 449-456.
- Kugel G ,Perry RD ,Aboushala (2003) A Restoring anterior maxillary dentition using alumina and zirconia based CAD/CAM restorations. Compendium 8: 569-579.
- Kelly JR ,Tesk JA, Sorensen JA (1995) Failure of all-ceramic fixed partial dentures in vitro and in vivo: Analysis and modelling. J Dent Res 74: 1253-1258.
- Esquvel-Upshaw JF, Anusavice KJ (2000) Ceramic design concepts based on stress distribution analysis. Compendium 8: 649-654.
- Wakabayashi N , Anusavice KJ (2000) Crack initiation modes in bilayered alumina/porcelain disks as a function of core/veneer thickness ratio and supporting substrate stiffness. J Dent Res 79: 1398-1404.
- Borges GA, Sophr AM, de Goes MF, Sobrinho LC, Chan DCN (2003) Effect of etching and airborne particle abrasion on the microstructure of different dental ceramics. J Prosthet Dent 89: 479-488.
- Horn H (1983) Porcelain laminate veneers bonded to etched enamel. Dent Clinc North Am 27: 671-683.
- Burke FJ ,Watts DC (1994) Fracture resistance of teeth restored with dentinbonded crowns. Quintessence Int 25: 335-340.
- Qualtrough AJE Piddock V (1997) Ceramics update. J Dent 25: 91-95.
- Isgró G Addison O Fleming GJP (2010) Deformation of dental ceramics following adhesive cementation 89: 87-90.
- Seghi RR, Denry IL, Rosenstiel SF (1995) Relative fracture toughness and hardness of new dental ceramics. J Prosthet Dent 74: 145-150.
- Grossman DV (1988) The science of castable glass ceramics. In Preston JD, editor. Perspectives in Dental Ceramics. Chicago: Quintessence Publishing Co. Inc 117-133.
- Isgró G ,Wang H, Kleverlaan CJ ,Feilzer AJ (2005) The effects thermal mismatch and fabrication procedures on the deflection of layered all-ceramic disc. Dent Mat 21: 649-655.
- Mackert JR, Evans AL (1991) Quantitative x-ray diffraction determination of leucite thermal instability in dental porcelain. J Am Ceram Soc 74: 450- 453.
- Mackert RJ (1988) Effects of thermally induced changes on porcelain-metal compatibility. In Preston JD, editor. Perspectives in Dental Ceramics. Chicago: Quintessence Publishing Co. Inc 52-64.





