Early Childhood Caries And Its Associated Risk Factors In Tunisian Preschool Children: A Cross-Sectional Study
Yamina Elelmi*, Souha Cherni, Fatma Masmoudi, Ahlem Baaziz
Pediatric Dentistry Department, Faculty of Dental Medicine, Research Laboratory, Biological Approach and Dento facial Clinic LR12ES10 Monastir University, Monastir, Tunisia.
*Corresponding Author
Yamina Elelmi,
Pediatric Dentistry Department, Faculty of Dental Medicine, Research Laboratory, Biological Approach and Dento facial Clinic LR12ES10 Monastir University, Monastir, Tunisia.
E-mail: yamina_elelmi@yahoo.fr/yamina.elelmi@fmdm.u-monastir.tn
Received: March 14, 2024; Accepted: April 29, 2024; Published: May 17, 2024
Citation: Yamina Elelmi, Souha Cherni, Fatma Masmoudi, Ahlem Baaziz. Early Childhood Caries And Its Associated Risk Factors In Tunisian Preschool Children: A Cross-Sectional
Study. Int J Dentistry Oral Sci. 2024;11(1):5342-5348.
Copyright: Yamina Elelmi�2024. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Early Childhood Caries (ECC) is a severe form of decay that affects primary dentition in children. It has significant
impact on children's well-being.
Aim: The aim of this study was to assess the prevalence of ECC and its associated risk factors among preschool children in
the region of Monastir, Tunisia.
Material and Methods: It was a descriptive cross-sectional study involving children in preschool establishments in Monastir,
Tunisia. An oral examination of 393 children was conducted and data collection through a questionnaire was completed by
parents. ANOVA test and Pearson chi-square test were used to determine the prevalence of ECC and its associated risk factors.
Results: The prevalence of ECC was 49.9% and the mean dmft index was 1.42+- 0.1. A statistically significant relationship
was found between the prevalence of ECC, the frequency of sweat consumption (p=0.05), the frequency of tooth brushing
(p=0.05),the mother�s level of education (p=0.05) and black stain (p=0.05).
Conclusion: The prevalence of ECC among preschool children was important. Prevention seems to be the best way to
reduce the prevalence of ECC. This involves educating parents about the importance of temporary dentition for an optimal
child development.
2.Case Report
3.Discussion
4.Conclusion
5.References
Keywords
Dental caries; Child; Preschool; Prevalence; Risk Factors.
Introduction
Early childhood caries is a serious internationally- recognized
public health problem because of its high prevalence, its early
appearance, its rapid progress, and its repercussions on teeth. It
greatly affects young children's well-being and it is difficult to be
treated.
It was thoroughly described for the first time in 1962 by Dr Fass.
He called it �Nursing bottle mouth� as he noticed a significant
prevalence of caries among children who were fed by nocturnal
milk bottles.[1]
This disease was initially associated with an inappropriate use of
the nursing bottle. Later, others terminologies were introduced,
such as �rampant caries� referring to a specific particularity of
this disease with regard to its more preferential progression on
smooth surfaces than on pits and cracks.[2]
In 2004, it was defined by the American Academy of Pediatric
Dentistry (AAPD) as the presence of one or more cavitated or
non-cavitated lesions, missing teeth (due to caries) or filled tooth
surfaces in any primary tooth in a child aged 71 months or younger.
[3]
The aetiology of ECC has been proved to be multifactorial, involving
cariogenic microorganisms, exposure to fermentable carbohydrates
through in appropriate feeding practices, and environmental
factors such as the socioeconomic status as well as the
parents� education. [4]
The consequences of this pathology have an incidence on the child�s quality of life on both short-term and long-term basis in
the advanced cases. It can even have considerable economic and
social consequences for the child�s family.
Therefore, in order to identify the high-risk population at the earliest
stage, it is necessary to identify the risk factors of ECC.
The aim of this study was to determine the prevalence of ECC
among children under the age of six in the region of Monastir
and to analyze its risk factors.
Materials And Methods
It was a cross sectional study carried out in preschool establishments
in the region of Monastir, Tunisia. It included children
aged from 2 to 5 years with primary teeth.
Sample size
The required sample size was calculated according to the following
formula n= Z� x (P) (1-P)/d�. [5]
where Z=1.96 is the confidence level for an accuracy of 0.05, p=
60.9% is the prevalence of early childhood caries according to
a similar epidemiological survey conducted in Morocco in 2013,
and d=0.05 corresponds to the chosen accuracy.
After this calculation, the sample size included at least 393 individuals.
The cluster sampling method was used for the selection of the
subjects.
A first draw was made to select 21 kindergartens in the various
places of the region holding children from all socioeconomic levels.
At the level of each cluster, a second draw was made to select
the eligible cluster units (small section, medium section, large section).
Inclusion Criteria
The children included in this study were:
- Those under 6 years of age who were present in the kindergarten
at the time of the study.
- Those with primary dentition.
- Those whose parents completed the questionnaire.
Non-inclusion criteria:
The children non-included in this study were:
- Those who were absent during our visit.
- Those with mixed dentition.
- Those whose parents did not consent to their children�s participation
or who did not complete the questionnaire.
The non-included children equally participated in the interactive
session to increase awareness of the oral health and dental hygiene
services.
Conduct of the study
First, an approval from the Regional delegation of the Ministry of
Family and Child Welfare was obtained. Then, the heads of the
kindergartens were informed about the study. Finally, consents of
the parents were obtained.
During the first visit, the questionnaires were given to the teachers
at these institutions who were asked to distribute them to the
children�s parents. They were given an average of one week to fill
in the required information. During the second visit, the questionnaires
were collected and an oral examination was performed.
Data collection
Data were collected using a questionnaire filled out by the parents
and an oral examination conducted by a single examiner.
The questionnaire included information regarding the parent�s
demographic data, educational level, origin, marital status, medical
coverage, and the duration as well as the type of breastfeeding.
Information about the child included the, general health state,
visits to the dentist, feeding habits during the day and night, duration
and content of the baby bottle and finally the oral hygiene.
Oral examinations were performed at kindergartens by a trained
dentist and were based on the WHO guidelines (WHO 1997, oral
health surveys: basic methods 4th edition). The Children were
seated on a chair facing a window and the examiner respected all
hygienic cautions, including wearing disposable gloves and tongue
droppers to prevent cross-infection between children. No radiographs
were taken.
The oral examinations recorded dmft indexes, including the number
of decayed, extracted, and filled primary teeth. The presence
of black stain was also recorded according to Koch method
which consists in visual inspection of dark dots (less than 0.5 mm
in diameter), forming linear discoloration parallel to the gingival
margin at the dental smooth surfaces of at least two different
teeth without cavitation of the enamel surface. [5]
Statistical analyses
Statistical analyses were performed using SPSS 24.0 and Microsoft
Excel 2010 software.
Significance was considered for p\0.05.
Analysis of data distribution was carried out using the Kolomognou-
smirnov test.
When distributions were normal and variances were equal, the
results were expressed as their mean +/- the standard error of
the mean. ANOVA test and Pearson chi-square test were used to
compare the different variables.
Results
Table 1 shows the data of 393 included subjects (193 boys and
200 girls), according to the selected characteristics.
Of all the children, 45.5% were aged between 4 and 5 years and
87.7% came from a middle socioeconomic level.
A further examination of the parents� academic statuses showed
that 62.2% of the mothers and 50.1% of the fathers reported
having a university level education.
Of all the children, 11.4% suffered from chronic pathology.
Concerning tooth brushing, 14.2% of the children did not
brush their teeth, 63.9% brushed their teeth once a day and
21.9%brushed their teeth twice a day.
Of all the children who brushed their teeth, only 39.5% started
brushing between the age of one and three, 69.1%were assisted
by their parents, and only 12% of them consulted a dentist with
dental caries as the main reason for the visit (55.5%).
Moreover, 39% of the children were breastfed for a long duration
(>-12 months),53% took nocturnal bottle, and 44.5% used cariogenic
aliments in the nocturnal bottle.
Almost 50% of the children took at least one sweet per day.Only
6.1% of the children presented black stain.
The prevalence of ECC was 49.9% (196/393) and the mean dmft
index was 1.42�0.1.
The different components of the dmft index are detailed in the
following table (table2).
With regard to the dmft index components, component �d� (decayed)
represented 90% of the dmft index. Actually, in this study,
515 decayed teeth were noticed while only 28 filled teeth and 17
missed teeth were present.
The distribution of caries prevalence and mean dmft index according
to certain characteristic of the sample are shown in table
3.
The highest prevalence of ECC was noticed in children belonging
to a low socio-economic level(56%), those who were breastfed
for prolonged duration(54.9%), those who did not brush their
teeth(69.9%), those who started brushing their teeth at the age
of three years(51.4%), and those who took sweets more than
twice per day (61.2%) .An increase in the dmft index with age was
found. It was 1.29 for children aged between 2 and 3 years, 1.37
for 4- year-old children and 1.81 for 5- year-old children.
No difference was noticed in the mean dmft indexes based on
gender. It gradually increased with age, though.
The mean dmft index was more important in children who suffered
from chronic pathology (1.89) than in those without chronic
pathology (1.36).
An incredible increase was noticed in the children who already visited a dentist with a value of 3.71. Those who consulted for
caries had the highest mean dmft index (4.52).The Subjects with
black stain(24) presented the lowest prevalence of ECC(33.3%)
and the lowest mean dmft index(0.83).
An association was found between ECC and the frequency of
tooth brushing, the daily frequency of sweets intake, the age at
which the children started brushing, the dental visits, the black
stain, and them others� education level (p=0.05). Yet, no association
with the content of the baby bottle an the type of nursing
was found (p=0.05
With regard to the mean dmft index, a statistically significant correlation
was found with chronic pathologies, dental visits, reason
for visits, brushing frequency, sweets intake frequency, socio-economic
level and mothers� education level (p=0.05).
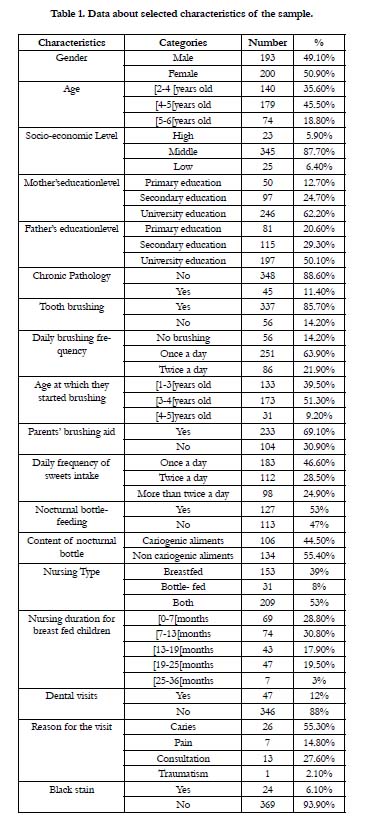

Table 1: Demographic characteristics of participants.
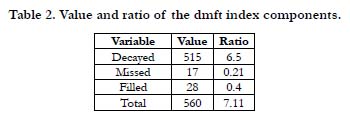
Table 2: COVID-19 encounter and fear of dental treatment.
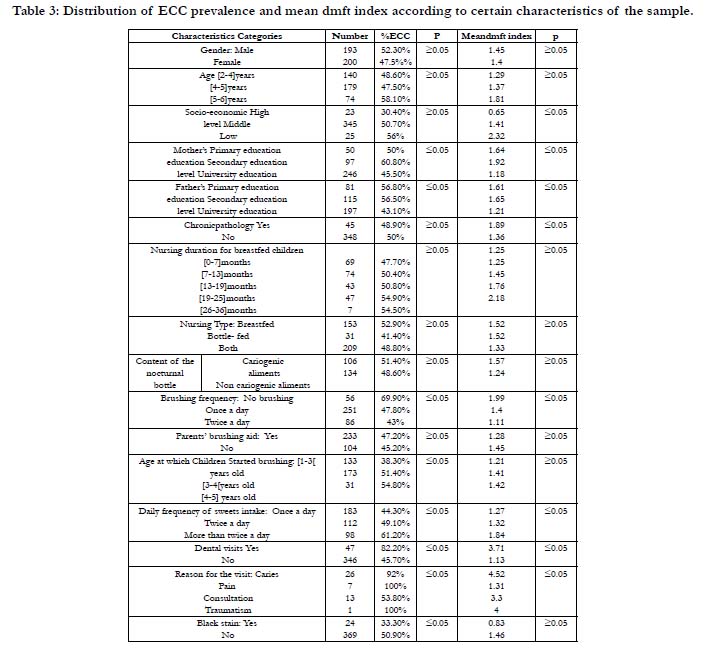
Table 3: Results of Q14. How often should a person brush his teeth per day?
Discussion
The results of this study revealed that caries prevalence in children�s
primary teeth was 49.9% and the mean dmft index was
1.42�0.1, which underlines a relatively important carious affection.
The prevalence of this disease varies from one country to another
and remains generally important in the developing countries.
Two studies in Saddar in Pakistan [7] and in Istanbul in Turkey [8]
showed similar prevalence to the one found in our study, being
close to 51%.
Some countries emerging as major world powers show inferior
prevalence than the one found in our study. For instance, in 2012
[9] the prevalence of caries in India was 27.5% with a mean dmft
index of 0.854 and in Brazil it was 20%. [10]
The most developed countries in the world show an inferior
prevalence compared to the one found in our study. We cite the
example of Brisbane in Australia, Singapore and the United States
with percentages of caries affection, respectively of 33.7%, 40%
and 28%. [11-13]
The observed differences with regard to ECC prevalence can be
explained by the economic conditions as well as the inequality
between the different countries and regions.
The lack of financial and human aptitude to promote oral health
among preschoolers in the emerging countries compared to the
developed countries, and the difficulty to access dental care in
some countries is the main reason for this difference.
The sample consisted of 393 children, including 193 boys. Similar
carious lesions were detected in both genders. No statistically
significant relationship was identified (p=0.05). This was substantiated
by many studies [7, 14] even though some other surveys
proved the opposite. [15]
The absence of correlation between these two parameters can be
due to the fact that kids at that age, regardless of their gender,
are not conscious of the importance of their oral hygiene habits
as they depend on their parents concerning brushing habits and
alimentation.
The results revealed an increase in carious affection with age. In
fact, the mean dmft index was 1.29 for children between 2 and 3
years, 1.37 for 4-year-old children and 1.81 for 5-year-old children.
Even though the statistical relationship in this study was not significant
(p=0.05), most of other studies confirmed this correlation.
[13, 7, 9]
To explain this association, time(being a major component of
Keyes modified scheme) becomes more considerable and teeth
become more and more exposed to oral environment.
Another plausible explanation is related to the alimentation habits.
These habits become uncontrolled with time, especially among
preschoolers.
There is also a lack of monitoring with respect to tooth brushing
that may affect the brushing quality and eventually the overall oral
hygiene quality.
It has been demonstrated in several studies [16] that an adequate
oral hygiene contributes to a decrease in caries. The current
study revealed a statistically significant relationship between daily
brushing frequency and ECC (p=0.05). In fact, children brushing
their teeth once a day presented an ECC prevalence of 47.8%
and a mean dmft index of 1.4 which is remarkably lower than
those found in children without brushing habits, who presented a
prevalence of 69.9% and a mean dmft index of 1.99.
Some urgent procedures should be taken in order to include systematic
correct teeth brushing techniques in preschool establishments.
[17]. Serious preventive approaches, such as awareness
campaigns and intervention programs, should also be introduced
to inform parents and raise public awareness regarding simple
practices to prevent early caries in children.
The statistical relationship between the age at which children
started brushing and ECC prevalence was significant (p=0.05).
The results showed an ECC prevalence of 38.3% for children
who started brushing between 1 and 2 years. However, children
who started after the age of 3 presented a higher prevalence of
ECC. The mean dmft index confirmed this main point as we
found a mean dmft index of 1.21 for the kids who started brushing
between 1 and 3 years and 1.4 for the others.
In view of what was previously mentioned, the time of the oral
cavity exposure to bacteria because of the lack or absence of oral
hygiene may increase the risk of ECC. Hence tooth brushing
should be performed for children twice daily and started as soon
as the first primary tooth erupted as recommended by the American
Association of Pediatric Dentistry [18].
Parents� assistance in the brushing process helps to improve its efficiency.
This has been found in previous studies even though no
significant statistical relationship was retained in our study. In fact,
children supervised during brushing presented a mean dmft index
of 1.28 against an index of 1.45 for non-monitored children. This
association was evoked by some authors [19, 9] who explained it
by the lack of manual dexterity in children, which is essential for
an efficient elimination of bacterial plaque.
The American Association of Pediatric Dentistry recommended
a dental visit at the age of one year, then bi-annual visits to the
dentist for children. [3]
Nevertheless, 88% of the children in our sample never visited the
dentist. This highlights the lack of interest on the part of parents
towards their children�s oral health, especially with regard to primary
dentition.
In fact, for children having previous dental visits, ECC prevalence
was 82.2%, twice as much as the rest of the sample presenting a
prevalence of 45.7%.
The mean dmft index confirmed this association with a value of
3.71 for the kids with dental care visits and 1.13 for the others. In
this study, this relationship was statistically significant both for the
dmft index (p=0.05) and the ECC prevalence (p=0.05).These results
proved that chief complaints were essentially caries-related.
A more important mean dmft index of 1.89 was noticed in children
with chronic pathologies compared to healthy children
whose dmft index was 1.36. This relationship was statistically significant
(p=0.05).This could be explained by the frequent intake
of drugs rich of saccharine.
Beyond the existing disparities throughout the world, ECC prevalence
remains high due to the accessibility and the increasing consumption
of refined sugars because of the modern life style and
nutritional changes caused by globalization. [20, 21]
More than three quarters of the children included in the sample
consumed cariogenic snacks or sweets between meals. In our
study, a statistically significant relationship was found between
the frequency of sweet consumption and both ECC prevalence
(p=0.05) and the mean dmft index (p=0.05).
The results of this study revealed that the higher the frequency of
sweets consumption between meals was, the more important the
carious affection was.
As a matter of fact, children who consumed sweets once a day
presented an ECC prevalence of 44.3% and a mean dmft index
of 1.27. However, children who consumed sweets more than
twice a day presented a prevalence of 61.2% and a mean dmft
index of 1.84.
The latter finding could be explained by the fact that sweets contain
rich amounts of fermentable carbohydrates, required for the
constitution of acids that maintain oral PH at low levels, which
will initiate the demineralization of teeth surfaces and consequently
the cariogenic process.
Concerning the use of nocturnal bottle, our study did not show
any statistically significant relationship between this variable and
ECC prevalence (p=0.05).
Indeed, ECC prevalence in children fed with nocturnal bottle and
in others was similar. The same was found with the mean dmft
indexes.
Our results are inconsistent with those found in many international
studies [22, 7-9] confirming that bottle feeding, especially at
night, is a major risk factor for developing ECC.
These results could be explained by the fact that this pathology
is not related to only nocturnal bottle nursing. For this reason, its
appellation was revised and it is now called early childhood caries,
instead of baby bottle caries.
In this study, the parents were asked about the nursing type offered
to their children as well as the duration.No statistically
significant relationshipwas foundfor ECC prevalence and mean
dmft index.
This was confirmed by a study conducted in India that compared
ECC prevalence according to the nursing type during early childhood.
[9]
However, an increase in ECC prevalence and mean dmft index
was observed with the increase of the nursing period.
In fact, the kids who were nursed over a period of time not exceeding
6 months presented an ECC prevalence of 47.7% and a
mean dmft index of 1.25. These values increased gradually until
reaching a maximum value for the kids who were nursed more
than two years with an ECC prevalence of 54.5% and a mean
dmft index of 2.18.Hence,it remains mandatory to limit the number
of meals to 5 at most.
The socio-economic level is considered as a risk factor for ECC
according to many studies. [23, 24, 9]
An association was found between the socioeconomic level and
the mean dmft index (p=0.05) This index was weaker for the kids
belonging to a high socio-economic level with an index 0.65 and
it increased considerably for the kids from a modest background
with a value of 2.32.s
Children with a modest background presented an ECC prevalence
of 56%, twice more important than the ECC prevalence
recorded in children belonging to a high background with an ECC
prevalence of 30.4%.
A modest socioeconomic background was correlated with nonaccessibility
to health care systems for dental treatments, bad nutritional
habits, and the parents� perception towards the importance
of oral health in children at the early age. [25]
The parents �education level, particularly the mothers�, is defined
in several studies as a confirme d risk factor for ECC. [26, 13, 21]
Our study confirmed this finding. In fact, a decrease in ECC prevalence
was identified in the children whose mothers had received
a university education, with a value of 45.5% compared to the
children whose mothers had only had a secondary education, with
a value estimated at 60.8%. This relation was statistically significant
for both ECC prevalence (p=0.05) and dmft index (p=0.05).
In fact, the higher the educational level of the mother is, the more
conscious she is of the oral hygiene importance and the more
careful she is about her kid�s diet, especially sweets intake.
The relationship was statistically significant concerning the fathers�
education level for both ECC prevalence and mean dmft index values. Our results showed that children whose fathers� received
a university education had an ECC prevalence of 43.1%;
however, children whose fathers received a primary education had
an ECC prevalence of 56.8%.Yet, some other studies have not
proved this association [27].
A statistically significant relationship was found between ECC and
black stain (p=0.05). Children with black stain had lower prevalence
of ECC (33.3%) than those without black stain (50.9%).
A lower mean dmft index was also noted in children with black
stain (0.83) than in those without black stain (1.46). These results
are consistent with many studies suggesting that black stain has a
protective effect against early childhood caries [28, 29].
Conclusion
This study demonstrated significant statistical relationships between
ECC prevalence and different parameters, such as the
frequency of sweets intake, the brushing frequency, the parents�
education level and black stain.
Deciduous teeth are always neglected by parents because of their
temporary aspect.
It is at this level that supplementary efforts should be made by
health care authorities and dentists to raise parents� awareness regarding
the importance the lacteal dentition, having a primordial
role in an optimal biological and behavioral development of the
child.
In preschool establishments, teaching children an adequate brushing
technique is the best way to prevent EEC. Moreover, further
studies are needed to elucidate the causal relationship between
black stain and ECC.
Data Availability
The data of the assessed parameters used to support the finding
of the present study are available from the corresponding author
upon request.
References
-
[1]. Fass EN. Is bottle feedi
ng of milk a factor in dental caries. J Dent Child. 1962 Mar;29(7):245-51. [2]. Curzon ME, Drummond BK. Case report�Rampant caries in an infant related to prolonged on-demand breast-feeding and a lacto-vegetarian diet. J Paediatr Dent. 1987;3:25-8.
[3]. AAPD. Perinatal and Infant Oral Health Care. Pediatr Dent. 2017; 39: 208- 212.
[4]. Tinanoff N, Baez RJ, Diaz Guillory C, Donly KJ, Feldens CA, McGrath C, et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int J Paediatr Dent. 2019 May;29(3):238-248. PubMed PMID: 31099128.
[5]. Kang M, Ragan BG, Park JH. Issues in outcomes research: an overview of randomization techniques for clinical trials. J Athl Train. 2008 Apr-Jun;43 (2):215-21. PubMed PMID: 18345348.
[6]. Koch MJ, Bove M, Schroff J, Perlea P, Garcia-Godoy F, Staehle HJ. Black stain and dental caries in schoolchildren in Potenza, Italy. ASDC journal of dentistry for children. 2001 Sep 1;68(5-6):353-5.
[7]. Narendar D , Nighat N, Nazeer K, Shahbano S, Navara T. Prevalence and factors related to dental caries among pre-school children of Saddar town, Karachi, Pakistan: a cross-sectional study. BMC Oral Health. 2012; 12:59- 67.
[8]. M�NEVVEROGLU AP, Koruyucu M, Seymen F. Risk factors for early childhood caries (ECC) in 2-5 years old children. Journal of Istanbul University Faculty of Dentistry. 2014;48(1):19-30.
[9]. Subramaniam P, Prashanth P. Prevalence of early childhood caries in 8-48 month old preschool children of Bangalore city, South India. Contemporary Clinical Dentistry. 2012 Jan 1;3(1):15-21.
[10]. dos Santos Junior VE, de Sousa RM, Oliveira MC, de Caldas Junior AF, Rosenblatt A. Early childhood caries and its relationship with perinatal, socioeconomic and nutritional risks: a cross-sectional study. BMC Oral Health. 2014 May 6;14:47 PubMed PMID: 24885697.
[11]. Hallett KB, O'Rourke PK. Dental caries experience of preschool children from the North Brisbane region. Aust Dent J. 2002 Dec;47(4):331-8. Pub- Med PMID: 12587770.
[12]. Dye BA, Tan S, Smith V, Lewis BG, Barker LK, Thornton-Evans G, et al. Trends in oral health status: United States, 1988-1994 and 1999-2004. Vital Health Stat 11. 2007 Apr;(248):1-92. PubMed PMID: 17633507.
[13]. Gao XL, Hsu CY, Loh T, Koh D, Hwamg HB, Xu Y. Dental caries prevalence and distribution among preschoolers in Singapore. Community Dent Health. 2009 Mar;26(1):12-7. PubMed PMID: 19385434.
[14]. Mahejabeen R, Sudha P, Kulkarni SS, Anegundi R. Dental caries prevalence among preschool children of Hubli: Dharwad city. J Indian Soc Pedod Prev Dent. 2006 Mar;24(1):19-22. PubMed PMID: 16582526.
[15]. Sufia S, Chaudhry S, Izhar F, Syed A, Mirza BA, Khan AA. Dental caries experience in preschool children: is it related to a child's place of residence and family income? Oral Health Prev Dent. 2011;9(4):375-9. PubMed PMID: 22238736.
[16]. Declerck D, Leroy R, Martens L, Lesaffre E, Garcia-Zattera MJ, Vanden Broucke S, Debyser M, et al. Factors associated with prevalence and severity of caries experience in preschool children. Community Dent Oral Epidemiol. 2008 Apr;36(2):168-78. PubMed PMID: 18333881.
[17]. Tang JM, Altman DS, Robertson DC, O'Sullivan DM, Douglass JM, Tinanoff N. Dental caries prevalence and treatment levels in Arizona preschool children. Public Health Rep. 1997 Jul-Aug;112(4):319-29; 330-1. PubMed PMID: 9258297.
[18]. Dentistry AAOP, Pediatrics AAO. Policy on Early Childhood Caries (ECC): classifications, consequences, and preventive strategies. Pediatric Dentistry. 2011;30(7 Suppl):31�33.
[19]. Ibrahim S, Nishimura M, Matsumura S, Rodis OM, Nishida A, Yamanaka K, Shimono T. A longitudinal study of early childhood caries risk, dental caries, and life style. Pediatric Dental Journal. 2009 Jan 1;19(2):174-80.
[20]. Paul TR. Dental health status and caries pattern of preschool children in Al-Kharj, Saudi Arabia. Saudi Med J. 2003 Dec;24(12):1347-51. PubMed PMID: 14710282.
[21]. erera PJ, Abeyweera NT, Fernando MP, Warnakulasuriya TD, Ranathunga N. Prevalence of dental caries among a cohort of preschool children living in Gampaha district, Sri Lanka: a descriptive cross sectional study. BMC Oral Health. 2012 Nov 13;12:49. PubMed PMID: 23148740.
[22]. Weinstein P, Smith WF, Fraser-Lee N, Shimono T, Tsubouchi J. Epidemiologic study of 19-month-old Edmonton, Alberta children: caries rates and risk factors. ASDC J Dent Child. 1996 Nov-Dec;63(6):426-33. PubMed PMID: 9017177.
[23]. Gillcrist JA, Brumley DE, Blackford JU. Community socioeconomic status and children's dental health. J Am Dent Assoc. 2001 Feb;132(2):216-22. PubMed PMID: 11217596.
[24]. Filstrup SL, Briskie D, da Fonseca M, Lawrence L, Wandera A, Inglehart MR. Early childhood caries and quality of life: child and parent perspectives. Pediatr Dent. 2003 Sep-Oct;25(5):431-40. PubMed PMID: 14649606. [25]. Reisine S, Douglass JM. Psychosocial and behavioral issues in early childhood caries. Community Dent Oral Epidemiol. 1998;26(1):32-44. PubMed PMID: 9671198.
[26]. Schroth RJ, Moffatt ME. Determinants of early childhood caries (ECC) in a rural Manitoba community: a pilot study. Pediatr Dent. 2005 Mar- Apr;27(2):114-20. PubMed PMID: 15926288.
[27]. Masumo R, Bardsen A, Mashoto K, �str�m AN. Prevalence and socio-behavioral influence of early childhood caries, ECC, and feeding habits among 6-36 months old children in Uganda and Tanzania. BMC Oral Health. 2012 Jul 26;12:24. PubMed PMID: 22834770.
[28]. Saba C, Solidani M, Berlutti F, Vestri A, Ottolenghi L, Polimeni A. Black stains in the mixed dentition: a PCR microbiological study of the etiopathogenic bacteria. J Clin Pediatr Dent. 2006 Spring;30(3):219-24.PubMed PMID: 16683670.
[29]. Theilade J, Slots J, Fejerskov O. The ultrastructure of black stain on human primary teeth. Scand J Dent Res. 1973;81(7):528-32. PubMed PMID: 4129441.





