Root Morphology Of Mandibular Anterior Teeth In Mecca City Population
Abdulaziz S. Almatrafi1, Ammar K. Alhazmi1, Khalid A. Alshahrani1, Wahdan M.A. Elkwatehy2*
1 Faculty of Dentistry, Umm AlQura University, Mecca, Kingdom of Saudi Arabia.
2 Dental Public Health and Preventive Dentistry Department, Faculty of Dentistry, Mansoura University, Egypt and Faculty of Dentistry, Umm AlQura University, KSA.
*Corresponding Author
Wahdan M.A. Elkwatehy,
Dental Public Health and Preventive Dentistry Department, Faculty of Dentistry, Mansoura University, Egypt and Faculty of Dentistry, Umm AlQura University, KSA.
E-mail: elkwatehywahdan@gmail.com
Received: September 18, 2021; Accepted: November 13, 2021; Published: November 24, 2021
Citation: Abdulaziz S. Almatrafi, Ammar K. Alhazmi, Khalid A. Alshahrani, Wahdan M.A. Elkwatehy. Root Morphology Of Mandibular Anterior Teeth In Mecca City Population. Int J Dentistry Oral Sci. 2021;8(11):5146-5151. doi: dx.doi.org/10.19070/2377-8075-210001034
Copyright: Wahdan M.A. Elkwatehy�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Root canal morphology is of utmost importance to the success of endodontic treatment.
Objectives: The present study aim is to determine the variation in root canal morphology of the loweranterior permanent
teeth using cone-beam computed tomography (CBCT) in a Saudi population especially Mecca city population.
Material and Methods: Cross-sectional study usingCBCT images of 388 patients included according to specific criteria to
evaluate the number of canals and their configuration according to Vertucci's classification.
Results: The prevalence of the second canal of mandibular canine was11% (11.3 in male and 10.7 in female), for mandibular
lateral incisor was 22.3% (28.5 for male and 16.7 for female) and mandibular central incisor represented 21% (22% for male
20.1% for female), these differences were not significant for canine (p=0.454) and central incisor (p=0.277) but significant
for lateral incisor (p=0.028). Regarding position, there were no significant differences between right and left side (p=0.517,
p=0.627 and p=0.507 for canine, lateral and central incisors respectively).According to Virtucci�s classes;type I was the most
prevalent followed by type III, II and V for lateral and central incisors and type III, V and II for canine.There were statistically
significant differences between male and female for lateral and central incisors morphology (p=0.003 and p=0.013) while the
difference was non significant for canine (p=0303).There were no significant differences between right and left side ( p=0.476,
p=0.707 and p=0.362 for canine, lateral and central respectively).
Conclusion: Type I Vertucci�sconfiguration was the most common type in all lower anterior teeth. The presenceof second
canal is more prevalent in mandibular lateral and central incisors and the morphology of their root canals is significantly different
between males and females.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Cone-Beam Computed Tomography CBCT; Mandibular Anterior Teeth; Root Canal Morphology.
Introduction
One of the most common causes of endodontic treatment failure
is intraradicular infection due to untreated canal anatomy [1].
Since unfilled canals are thought to be a potential reason for contamination
and can promote periapical disease after treatment,
their exact recognition would be fundamental [2]. Theknowledge
about root canal morphology is of utmost importance to the success
of endodontic treatment [3]. It was previously assumed that
mandibular anterior teeth had only one root canal [4].
Root canal morphology of permanent mandibular anterior teeth
may be compromised by the involvement of the second canal, lateral
canal, and apical deltas [2]. For permanent mandibular anterior
teeth, one of the most prevalent canal morphology is a single
root having a single canal [4]. However, there is a difference between
the numbers of canals among the different populations [5].
Iranian people had a prevalence of two root canals in 27.3% of
mandibular central, 29.4% of mandibular lateral, and 28.2% of
mandibular canine [6]. The Chinese population shows the prevalence
of the second canal in central incisors 9.8%, Lateral incisors
21.5%, canines 9.2% [7]. Indian population study showed
that,18.63% had two root canals in canine and 28.43% had two
root canals in central and lateral incisor [8].
Cone-beam computed tomography (CBCT) provides a threedimensional
image in three different planes. Detection of the configuration and root canal convergence and divergence can be
viewed [9]. Mecca city have diverse population with expected variation
in root canal morphology of mandibular anterior teeth, thus
the current study was designed to determine the root canal morphology
of the permanent lower anterior teeth using cone-beam
computed tomography in Mecca city population.
Materials And Methods
The study design and ethical approval
The currentstudy was a cross-sectional study using Electronic
Health Records (EHR) at Umm Al-Qura University, Faculty of
Dentistry, Mecca, Saudi Arabia. Ethical approval(Ref #161-19)
was obtained from the Research Ethical Committee at the Faculty
of Dentistry, Umm Qura University. The confidentiality of the
participants was maintained.
Sample size determination
The sample size (S) was calculated by the following equation
(s=N/(1+Ne^2 ))[10].
N= number of population e= level of precision, calculated with
5% margin error acceptance and 95% confidence level. The required
sample was 388 participants.
Sample selection
The sample was selected after applying the inclusion/exclusion
criteria to 966 EHR. The focus group was Saudi population in
Mecca city included according to the following inclusion criteria:
Unrestored lower anterior teeth, complete root formation with
closed apex, Saudi people. Patients with deep caries, crown or
bridge, periapical lesion and root resorption, posts and root canal
fillings, missing anterior teeth were excluded from the study.
Root canal evaluation
CBCT dental imaging system (iCATvisionQ, Imaging Sciences
International, Hatfield, PA, USA) operates at 120 kVp and 3-7
mA. was used to evaluate the root canal morphology of lower
anterior teeth.The study was conducted on 388 CBCT images of
lower anterior teeth to estimate the number of root canals and
their types.CBCT images evaluated 1552 permanent mandibular
incisors, 776 permanent mandibular canines. Configuration of
the canal categorized according to the method of Vertucci's [3].
(Figure 1)
Type I: A single canal extends from the pulp chamber to the canal
terminus.
Type II: two separate canals depart the pulp chamber and connect
each other to create one canal at the canal terminus.
Type III: one canal departs the pulp chamber, split into two canals
then merging each other to create one canal at the apex.
Type IV: Two separate canals present from the pulp chamber to
the canal terminus.
Type V: One canal depart the pulp chamber, split into two separate
canals with two apical foramina.
Type VI: Two separate canals depart the pulp chamber, connect
each other in the body of the root, and separate short of the apex
to exit as two distinct canals.
Type VII: One canal depart the pulp chamber, divides and then
reconnect in the body of the root, and at the end separates into
two distinct canals short of the apex.
Type VIII: Three separate and well defined canals extend from
the pulp chamber to the apex.
The number of canals and root canal configuration of permanent
lower anterior teeth were examined in three dimensions by three
researchers after training and measurement of intra and inter examiner
consistency. Kapa test results was 86% for intra examiner
and 91 % for inter examiner stability.
Results
The prevalence of two canals was 11% for canine, 22.3% for lateral
and 21% for central incisor. According to position, the differences
between right and left side were not significant for #3
(p=0.517), #2 (p=0.657) and #1 (p=0.507).On comparison between
male and female, there were no significant differences between
them for #3 (p=0.454) and #1 (p=0.277) while there was
significant difference for #2 (p=0.028*). (Table 1, Figure 1 and 2)
The differences between right and left side were not significant
for both male and female participants, for male [#3 (p=0.751),
#2(p=0.311), #1 (p=0.500) and total of #2 + #1 (p=0.369)] and
for female [#3 (p=0.611), #2 (p=0.378), #1 (p=0.638) and total
of #2 + #1 (p=0.591)]. (Table 2)
According to Vertucci's classes,the difference between male and
femalewas not significant for #3 (p=0.303) while the differences
between them were statistically significant for #2 (p=0.003*) and
#1 (p=0.013*). The differences between right and left sidewere
not significant for #3 (p=0.476), #2 (p=0.707) and #1 (p=0.362).
(Table 3)
The differences between right and left side root canal types were
not significant for both male and female. For male participants
[#3 (p=0.667), #2 (p=0.857) and #1 (p=0.844)] and female participants
[#3 (p=0.641), #2 (p=0.772) and #1 (p=0.221)]. (Table 4)
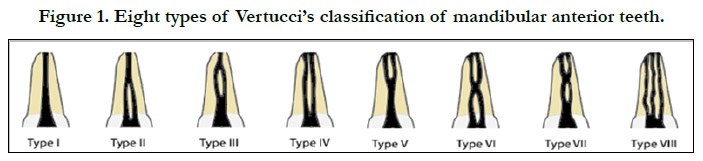
Figure 1. Eight types of Vertucci�s classification of mandibular anterior teeth.
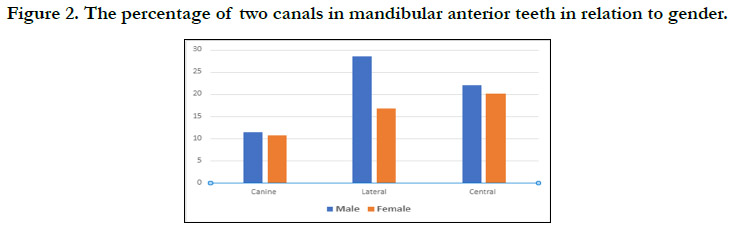

Figure 2. The percentage of two canals in mandibular anterior teeth in relation to gender.
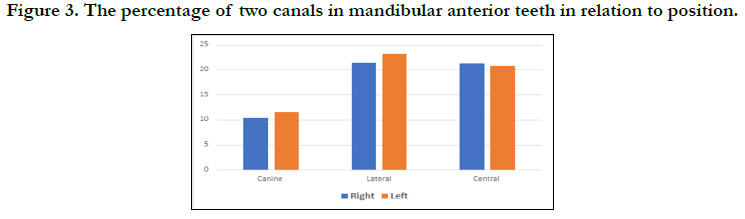

Figure 3. The percentage of two canals in mandibular anterior teeth in relation to position.
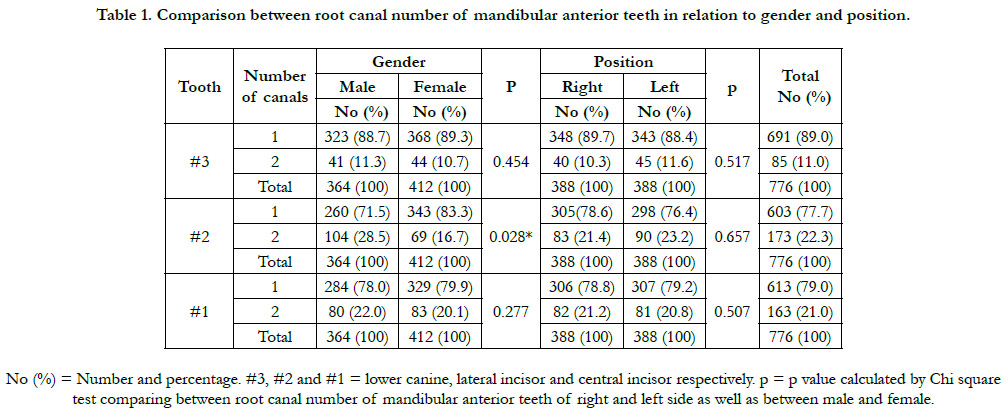

Table 1. Comparison between root canal number of mandibular anterior teeth in relation to gender and position.
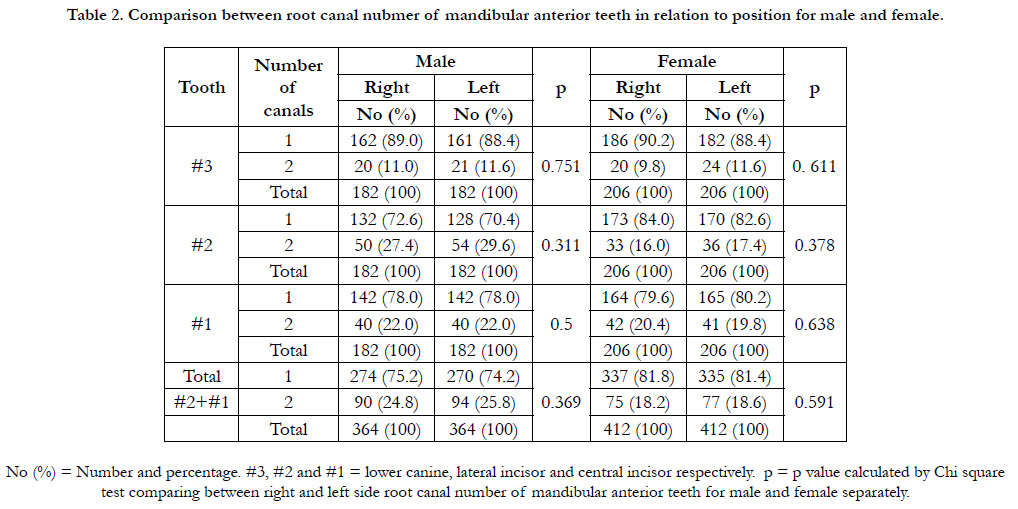
Table 2. Comparison between root canal nubmer of mandibular anterior teeth in relation to position for male and female.
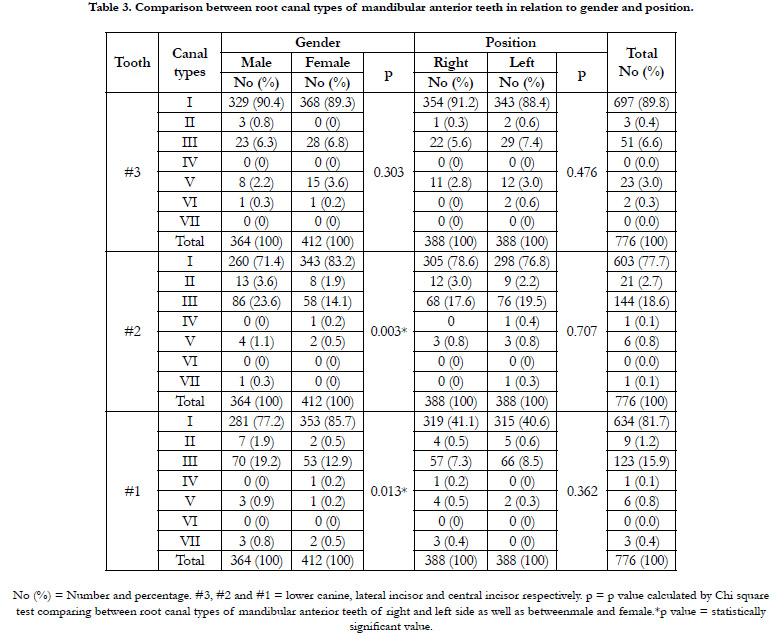
Table 3. Comparison between root canal types of mandibular anterior teeth in relation to gender and position.
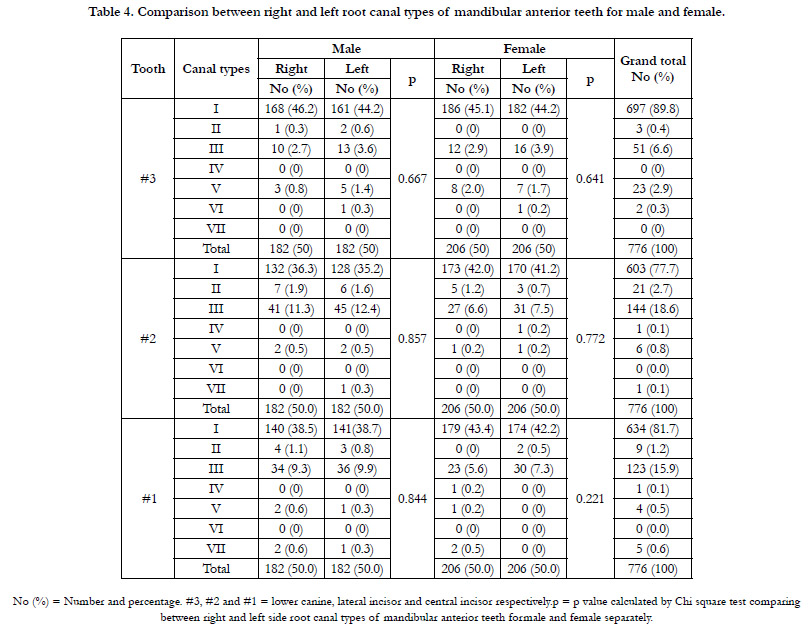
Table 4. Comparison between right and left root canal types of mandibular anterior teeth for male and female.
Discussion
Many reasons are leading to endodontic treatment failure, one of
the most common causes is missed canal due to improper diagnosis,
other causes include ledges, transportations, perforations,
separated instruments. Any of these influences the result of root
canal therapy. These operational errors are not specifically responsible
for endodontic failure. These mistakes negatively affect the
proper cleaning, shaping, and obturation of the root canal, which
in turn inhibits the prevention of endodontic infection [11-13].
CBCT used in different branches of dentistry, in endodontic
treatment like surgical apexification, root hemisection, and root
morphology. The key benefit of CBCT imaging is non-harmful
for the patient and allowing to clarify the image from sagittal,
axial, and coronal dimensions and provide imagining for anatomical
structures inside and outside the tooth and underlying bone
structures [14-16]. The most important advantages of CBCT are
lower radiation dose, accurate measurement, and lower cost relative
to traditional CT [17, 18].
The results of the current study indicated that, all the lower permanent
incisors have one root, the prevalence of the second canal
in permanent lower incisors was 21.6% (22.3% for lateral and
21% for central). The prevalence of two canals in lower incisors
of Mecca city populations was within the range recorded by previous
literature review where it was from 11.6% to 65.3%[12].
The present results were higher than the prevalenceobtained by
Madeira and Hetemet al. (11.6%)[19], Miyashita et al. (12.4%)
[20], and Liu et al. (13.2%)[21].The current prevalence was agreed
with that reported by Green (20%)[22] and Han et al. (21.55%)
[12]. On the other hand the reported prevalence in the present
study was less than that reported byBenjamin and Dowson (41.4)
[23], Vertucci (27.5%)[24], Kartal et al. (45%)[25], Caliskan et al.
(31.37%)[26], Al-Qudah and Awawdeh (26.2%)[27], Aminsobani
et al. (29%)[6], Rahimi et al. (36.62%)[4] and Kamtane et al. (36%)
[8].
The prevalence of the second canal in permanent mandibular canine
teeth of Mecca city population was (11%) which was higher
than the prevalence reported by Zhao et al. (3%)[7], Zhengyan et
al. (4.2%) [28], Rahimi et al. (8.4%) [4], Han et al. (6.7%) [11] and
Haghanifar et al. (9.4%)[29]. On the other hand, the prevalence
was less than that obtained byVertucci (22%) [24] and Sert et al.
(24%)[30].
In the current study,the prevalence of the second canal in lower
permanent incisorsin male was 25.3% (right side is 24.8%
and 25.8% in left side) and the difference was non significant
(p=0.369). For female, the prevalence was 18.4% (right side is
18.2% and 18.6% in left side)and the difference was non significant
(p=0.591), these findings weer higher than that reported by-
Green [22].
The prevalence of the second canal in permanent mandibular caninein
male was 11.3% (right side is 11% and 11.6% in left side)
and the difference was non significant (p=0.751). For female, the
prevalence was 10.7% ( right side is 9.8% and 11.6% in left side)
and the difference was non significant (p=0.611), these results
were closed tothe results reported by Rahimi et al.[4].
Totally there were no differences between right and left side regarding
lower permenant teeth (Table 1 and 2). The intermediate
prevalence of two root canals in Mecca population may be due to
diversity of its population and may be due to special characteristics
of Mecca population that different races had inter-married
and stayed there due to the holy nature of Makkah to all Muslim
population.
The findings of the present study showed that, Virtucci�s Type
I is the most prevalent type (89.8% for canine, 77.7% for lateral
and 81.7 for central incisor) followed by type III (6.6% for #3,
18.6% for #2 and 15.9% for #1), type II (0.4% for #3, 2.7% for
#2 and 1.2% for #1) and type V (2.9% for #3, 0.8% for #2 and
0.5% for #1).Thes findings were agreed with the results obtained
by numerous researches showed that Vertucci�s type I is the most
prevalent type [31-33].
It has shown that, among double root canals, Vertucci's type III
was the most prevalentfor mandibular anterior teeth and this
support the results obtained byLin et al.[13]. The highest prevalence
of the various types of canals associated with Vertucci's
classification were types I, III, II and V which differe than that
obtained byAminsobhani et al.[6] who reported that, the prevalence
was types I, II, IV, III, and V respectively. The present findings
showed that, Vertucci's type III has the highest prevalence
as a two canaled mandibular incisors and this not agreed with
resultsreported by Altunsoy et al. [32] where they found Vertucci's
type V had the highest prevalence in double root canals.Another
study showed that the highest prevalence was the type's I, II, III,
and IV, respectively [4]. The prevalence of Vertucci's types were
I, III, V, respectively reported by da Silva et al.[34]. These differences
may be due to different ethnicity of the participants.
The present results indicated that, the endodontists should take
care during treatment of lateral and/or central incisors as there
were significant differences between male and female (p=0.003
and p=0.013). Also, the results indicated that, there were no specific
precautions during treating right or left side either for male
or male as there were no significant differences among them (Table 4
Conclusion
Type I Vertucci�s classification was the most common type in all
mandibular anterior teeth. Type IV and VII Vertucci's canal configuration
were the least prevalent type in canine. Type IV, VI and
VII were the least prevalent in lateral incisor. Type IV, V and VII
were the least prevalent in mandibular central incisors.
The presence of the second canal and Type III Vertucci�s classification
was relatively high in mandibular lateral and central incisors
so more attention should be given for these teeth during
endodontic treatment.
The Prevalence of the second canal in mandibular right and left
canines was the lowest, and mandibular right and left lateral incisors
was the highest.
The configuration of double rooted lateral and central incisors is
significantly differ in males than females.
Limitation
CBCT has limitations like image artifact and, it is sensitive to
technique errors so it needs special training for interpretation.
Moreover, CBCT is not a substitution for periapical, bitewing,
and panoramic x-rays it is used only for a particular diagnosis.
There is a restricted usage of CBCT in endodontics for the evaluation
of complex root canal morphology, root resorption, and
related conditions [18].
References
-
[1]. Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated
teeth can fail. IntEndod J. 2001 Jan;34(1):1-10. PubMed PMID: 11307374.
[2]. Saati S, Shokri A, Foroozandeh M, Poorolajal J, Mosleh N. Root Morphology and Number of Canals in Mandibular Central and Lateral Incisors Using Cone Beam Computed Tomography. Braz Dent J. 2018 May- Jun;29(3):239-244. PubMed PMID: 29972448.
[3]. Vertucci F.J. Root canal morphology and its relationship to endodontic procedures. Endod. Top. 2005; 10: 3�29.
[4]. Rahimi S, Milani AS, Shahi S, Sergiz Y, Nezafati S, Lotfi M. Prevalence of two root canals in human mandibular anterior teeth in an Iranian population. Indian J Dent Res. 2013 Mar-Apr;24(2):234-6. PubMed PMID: 23965453.
[5]. Pan JYY, Parolia A, Chuah SR, Bhatia S, Mutalik S, Pau A. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC Oral Health. 2019 Jan 14;19(1):14. PubMed PMID: 30642318.
[6]. Aminsobhani M, Sadegh M, Meraji N, Razmi H, Kharazifard MJ. Evaluation of the root and canal morphology of mandibular permanent anterior teeth in an Iranian population by cone-beam computed tomography. J Dent (Tehran). 2013 May;10(4):358-66. PubMed PMID: 24396355.
[7]. Zhao Y, Dong YT, Wang XY, Wang ZH, Li G, Liu MQ, Fu KY. [Conebeam computed tomography analysis of root canal configuration of 4 674 mandibular anterior teeth]. Beijing Da XueXueBao Yi Xue Ban. 2014 Feb 18;46(1):95-9. PubMed PMID: 24535357.
[8]. Kamtane S, Ghodke M. Morphology of Mandibular Incisors: A Study on CBCT. Pol J Radiol. 2016 Jan 13;81:15-6. PubMed PMID: 26834865.
[9]. Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography.J Endod. 2007 Sep;33(9):1121-32. doi: 10.1016/j.joen.2007.06.011. Epub 2007 Jul 19. PMID: 17931947.
[10]. Ryan TP. Sample Size Determination and Power, Sample Size Determination and Power. 2013.
[11]. Eleftheriadis GI, Lambrianidis TP. Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. IntEndod J. 2005 Oct;38(10):725-34. PubMed PMID: 16164687.
[12]. Han T, Ma Y, Yang L, Chen X, Zhang X, Wang Y. A study of the root canal morphology of mandibular anterior teeth using cone-beam computed tomography in a Chinese subpopulation. J Endod. 2014 Sep;40(9):1309-14. PubMed PMID: 25043332.
[13]. Lin Z, Hu Q, Wang T, Ge J, Liu S, Zhu M, Wen S. Use of CBCT to investigate the root canal morphology of mandibular incisors. SurgRadiol Anat. 2014 Nov;36(9):877-82. doi: 10.1007/s00276-014-1267-9. Epub 2014 Feb 11. PMID: 24515289.
[14]. Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. EurRadiol. 1998;8(9):1558-64. PubMed PMID: 9866761.
[15]. Bornstein MM, W�lner-Hanssen AB, Sendi P, Von Arx T. Comparison of intraoral radiography and limited cone beam computed tomography for the assessment of root-fractured permanent teeth. Dent Traumatol. 2009 Dec;25(6):571-577. PubMed PMID: 19843131.
[16]. Patel S, Horner K. The use of cone beam computed tomography in endodontics. Int J Endod. 2009; 42: 755�756.
[17]. Cohenca N, Simon JH, Roges R, Morag Y, Malfaz JM. Clinical indications for digital imaging in dento-alveolar trauma. Part 1: traumatic injuries. Dent Traumatol. 2007 Apr;23(2):95-104. PubMed PMID: 17367457.
[18]. Mallya S, Lam E. White and Pharoah� s Oral Radiology. 2018;1608. [19]. Madeira MC, Hetem S. Incidence of bifurcations in mandibular incisors. Oral Surg Oral Med Oral Pathol. 1973 Oct;36(4):589-91. PubMed PMID: 4517109.
[20]. Miyashita M, Kasahara E, Yasuda E, Yamamoto A, Sekizawa T. Root canal system of the mandibular incisor. J Endod. 1997 Aug;23(8):479-84. Pub- Med PMID: 9587315.
[21]. Liu J, Luo J, Dou L, Yang D. CBCT study of root and canal morphology of permanent mandibular incisors in a Chinese population. ActaOdontol Scand. 2014 Jan;72(1):26-30. PubMed PMID: 24255962.
[22]. GREEN D. A stereomicroscopic study of the root apices of 400 maxillary and mandibular anterior teeth.Oral Surg Oral Med Oral Pathol. 1956 Nov;9(11):1224-32. PubMed PMID: 13370115.
[23]. Benjamin KA, Dowson J. Incidence of two root canals in human mandibular incisor teeth. Oral Surg Oral Med Oral Pathol. 1974 Jul;38(1):122-6. PubMed PMID: 4525678.
[24]. Vertucci FJ. Root canal anatomy of the mandibular anterior teeth. J Am Dent Assoc. 1974 Aug;89(2):369-71. PubMed PMID: 4527223.
[25]. Kartal N, Yanikoglu F�. Root canal morphology of mandibular incisors. J Endod. 1992;18:562�564.
[26]. Caliskan MK, Pehlivan Y, Sepet�ioglu F, T�rk�n M, Tuncer SS. Root canal morphology of human permanent teeth in a Turkish population. J Endod. 1995 Apr;21(4):200-4. PubMed PMID: 7673821.
[27]. Al-Qudah AA, Awawdeh LA. Root canal morphology of mandibular incisors in a Jordanian population.IntEndod J. 2006 Nov;39(11):873-7. Pub- Med PMID: 17014525.
[28]. Zhengyan Y, Keke L, Fei W, Yueheng L, Zhi Z. Cone-beam computed tomography study of the root and canal morphology of mandibular permanent anterior teeth in a Chongqing population. TherClin Risk Manag. 2015 Dec 23;12:19-25. PubMed PMID: 26730198.
[29]. Haghanifar S, Moudi E, Bijani A, Ghanbarabadi MK. Morphologic assessment of mandibular anterior teeth root canal using CBCT. Acta Med Acad. 2017 Nov;46(2):85-93. PubMed PMID: 29338272.
[30]. Sert S, Aslanalp V, Tanalp J. Investigation of the root canal configurations of mandibular permanent teeth in the Turkish population. IntEndod J. 2004 Jul;37(7):494-9. PubMed PMID: 15189440.
[31]. Altunsoy M, Ok E, Nur BG, Aglarci OS, Gungor E, Colak M. A conebeam computed tomography study of the root canal morphology of anterior teeth in a Turkish population. Eur J Dent. 2014 Jul;8(3):302-306. PubMed PMID: 25202207.
[32]. Kayaoglu G, Peker I, Gumusok M, Sarikir C, Kayadugun A, Ucok O. Root and canal symmetry in the mandibular anterior teeth of patients attending a dental clinic: CBCT study. Braz Oral Res. 2015;29:S1806- 83242015000100283. PubMed PMID: 26154376.
[33]. Verma GR, Bhadage C, Bhoosreddy AR, Vedpathak PR, Mehrotra GP, Nerkar AC, Bhandari A, Chaubey S. Cone Beam Computed Tomography Study of Root Canal Morphology of Permanent Mandibular Incisors in Indian Subpopulation. Pol J Radiol. 2017 Jul 7;82:371-375. PubMed PMID: 28794810.
[34]. da Silva EJ, de Castro RW, Nejaim Y, Silva AI, Haiter-Neto F, Silberman A, Cohenca N. Evaluation of root canal configuration of maxillary and mandibular anterior teeth using cone beam computed tomography: An in-vivo study. Quintessence Int. 2016 Jan;47(1):19-24. PubMed PMID: 26417615.





